





Oesophageal perforations are uncommon and are usually associated with a high morbimortality rate.1 The most frequent causes are complications after endoscopic explorations,2 followed by foreign body ingestions, Boerhaave’ syndrome and chemical trauma. Treatment of these patients depends on their general state and the clinical situation, and in some cases requires surgery.
We present 3 cases of patients with oesophageal perforation treated conservatively in our centre during the past two years.
Case 1A 58-year-old man presented cardiac arrhythmia, chest pain and a sensation of a tear in the epigastric area after eating meat. He was found to be clinically stable, without dyspnea or tachycardia and a normal abdominal examination. No electrocardiological or blood test anomalies were found. Chest X-ray and CT scan revealed a left pleural effusion and pneumomediastinum. A water-soluble (Gastrografin®) contrast study did not reveal any extravasation of contrast, and an upper endoscopy revealed a fragment of meat and bone glued to the oesophageal wall; after mobilization, a 1.5cm perforation was found. Conservative treatment was started with antibiotics (Tigecyclin), NPO, enteral feeding through a nasojejunal tube and drainage of the pleural effusion. In the extracted fluid high levels of amylase and leukocytes were found. A self-expanding covered metallic stent was placed, which migrated to the gastric cavity in two occasions, provoking a limited haemorrhage and needed to be removed. After 4 sessions of endoscopic sealing with fibrin glue (Tissucol®) and a new contrast study without evidence of the perforation, the patient began an oral diet and was discharged after 54 days, and remained asymptomatic at one-month follow-up.
Case 2A 43-year-old man with alcoholic liver disease and oesophageal varices consulted for upper gastrointestinal bleeding. He was treated by sclerosis and banding, but a Sengstaken–Blackemore tube was finally needed to control the bleeding. After it was removed 72h later, the patient presented fever and a CT scan revealed a 6cm collection in the left posterolateral hemithorax. A contrast study revealed a small contained oesophageal leak, and upper endoscopy revealed a 1cm oesophageal perforation on the posterior wall of the mid-oesophagus. The patient remained stable and a chest drain was placed, the patient was kept on NPO and enteral nutrition through a nasojejunal tube and antibiotics (Tigecyclin). Subsequently, a TIPS (transjugular intrahepatic portosystemic shunt) was performed. After 3 sessions of endoscopic sealing with Tissucol®, the patient presented a favourable clinical course, and complete closure of the fistula was found after new radiological and endoscopic tests. Subsequently oral intake was started and the patient was discharged 69 days after admission. He has remained asymptomatic at three-month follow-up.
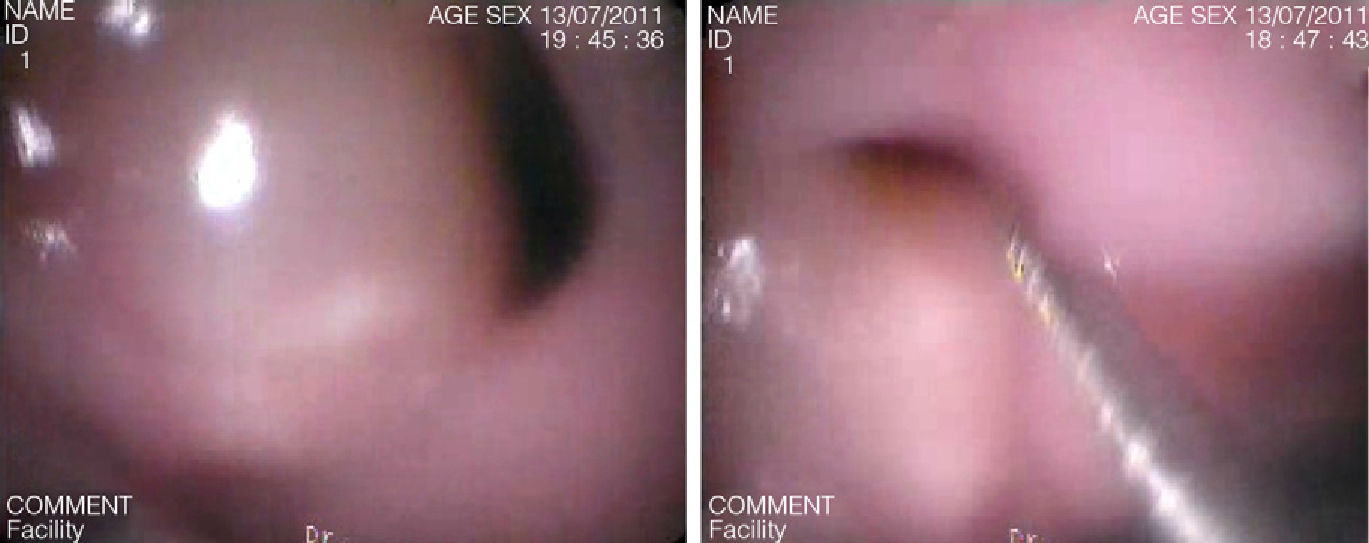
Case 3A 44 year-old man with a history of schizophrenia was admitted for vomiting and foreign body ingestion. The patient was clinically stable, with no dyspnea, sepsis or signs of peritoneal irritation. Endoscopy revealed a fistulous opening of approximately 1cm at the oesophageal-gastric junction and a plastic foreign body in the stomach, which was fragmented and extracted (Fig. 1). An upper gastrointestinal contrast study revealed a lineal leak in the distal oesophagus, and CT scan revealed a small right pleural condensation that did not require drainage. Antibiotic treatment was started (piperacillin–tazobactam), parenteral nutrition, bowel rest and 4 endoscopic sealing sessions with Tissucol®. He presented a favourable progression, and was discharged 45 days after admission, after a normal radiological study. Since then (6 months later) he has remained asymptomatic and endoscopy found an incomplete stenosis with no fistulous opening.

Surgical treatment of oesophageal perforations by laparotomy and/or thoracotomy, debridement, drainage, stomas and enteral or parenteral nutrition is associated with high morbidity and mortality rates,1 although it is the only alternative in patients with important clinical repercussion or in septic shock. However, in clinically stable patients, that usually present all the clinical criteria described by Cameron3 and Altorjay4 with contained leaks without sepsis, obstruction or tumours, an “aggressive” conservative treatment based on NPO, drainage of the pleura and mediastinum, enteral or parenteral nutrition and the use of broad-spectrum antibiotics is a valid and less aggressive5 alternative, with a cure rate of around 90% and a mortality rate lower than 5%.6 In these cases, it is essential to maintain a strict control of the patient, and if any sign of deterioration is seen, or signs of severe sepsis appear, surgical treatment would be necessary.
The diagnosis if usually confirmed by contrast radiology or CT scan, and the use of endoscopy are controversial, because it could, hypothetically, increase the size of the perforation and contamination of the mediastinum. However, with the advance in safety and experience of endoscopists, this technique is a safe option that has a high sensitivity and specificity for the diagnosis, location and determination of the size of the perforation, and also allows detection non-suspected lesions,7 removal of foreign objects and placement of enteral feeding tubes, sealing substances or stents.
The use of covered stents seems promising, although complications have been described (bleeding, increase in the size of the perforation, fistulisation to adjacent structures, etc.),8 and in some cases new tests, re-placement of the stent, or removal are needed, as in one of our cases. Other options, such as the application of clips, have been published as case reports, with cure rates over 90% and a decrease in hospital stay compared to surgical treatment.9
The use of fibrin glue is a safe technique with acceptable results and less morbidity; the fistulous opening must be identified, cleaned and debridement for an adequate application (Fig. 2). Several sessions are usually necessary to obtain closure of the fistula, and some series have presented good results in smaller fistulous orifices than our cases.10 In tracheoesophageal fistulas, it has been shown that approximately 50% remain sealed after endoscopic treatment, and recurrences are common in the first year of follow-up.11

Therefore, “aggressive” conservative treatment of patients with oesophageal perforations and clinical stability is a therapeutic option that obtains high survival rates and healing in many cases.
Please cite this article as: Bruna M, Sempere J, Cantos M, García Del Olmo E, Dávila D. Tratamiento conservador y empleo de pegamento de fibrina en perforaciones esofágicas. Cir Esp. 2013;91:336–338.
