





Renal cell carcinoma (RCC) represents approximately 3% of all cancers in the adult population and has shown the potential to metastasize to practically any part of the body.1 It most frequently affects the lungs, bones, brain, suprarenal glands, contralateral kidney and liver.2 Approximately 30% of patients have metastasis at the time of diagnosis and another 30% develop them after nephrectomy.3 The gallbladder is a very unusual place for this type of metastasis.
We present the case of a 55-year-old woman who had undergone right nephrectomy 6 years earlier due to clear-cell renal carcinoma. During radiological follow-up, on the last abdominal tomography we had observed a hypervascular polypoid lesion of the gallbladder that measured approximately 2cm in diameter. It was highly suggestive of a neoplastic process because of its behavior. In addition, hypervascular nodular lesions were also seen in the left kidney, which were a new finding and suggested metastasis of the renal carcinoma (Fig. 1).

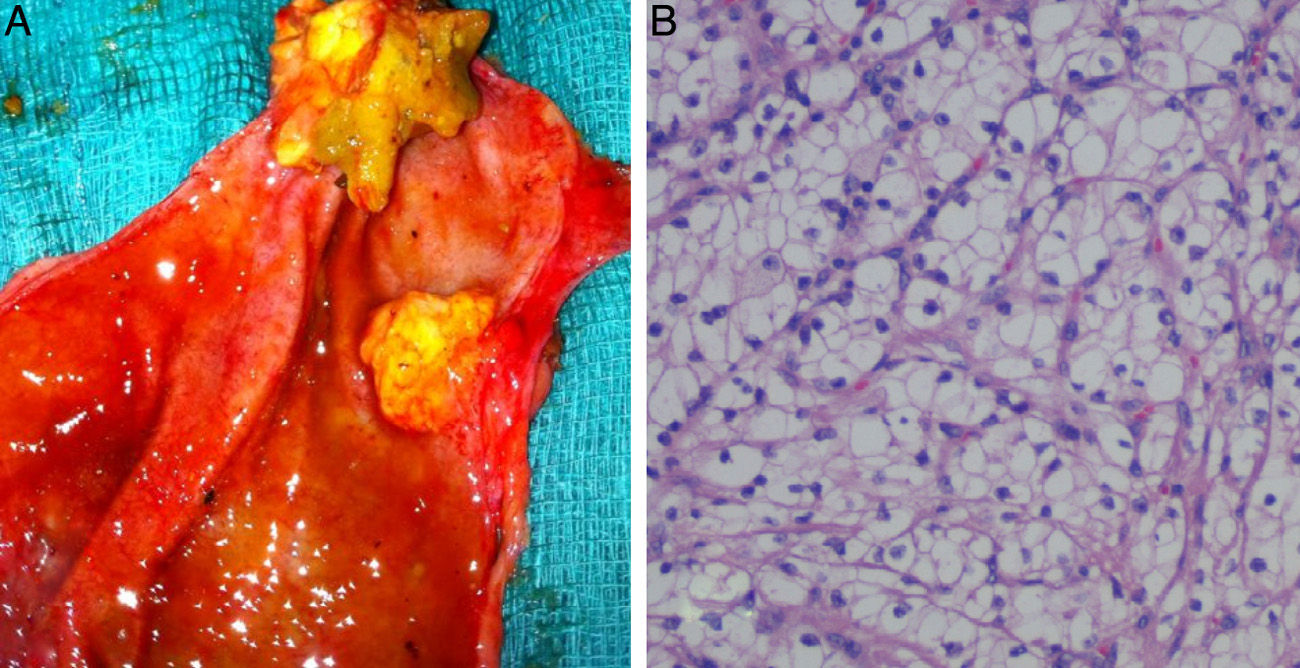
The decision was made to treat the patient surgically. During the procedure, the lesion was observed to be confined to the infundibulum of the gallbladder, and a cholecystectomy was performed. In the pathology study, macroscopically the lesion presented a solid nodule on the internal side of the infundibulum that was greenish-yellow and measured 3.5cm×1.8cm; microscopically, this lesion was morphologically and immunohistochemically consistent with metastasis of clear-cell carcinoma (Fig. 2, A: macroscopic image; B: microscopic image of the pieced that confirmed the diagnosis).
 Photograph of the open surgical specimen where the gallbladder tumor is observed; (B) pathology study of the specimen showing round tumor cells and abundant clear non-papillary cytoplasm, typical of clear-cell carcinomas.")
After the radical treatment of the gallbladder metastasis, the patient underwent oncologic surgery of the contralateral kidney metastasis by the urology department.
In a search of the literature until 2011 we found 39 published cases, 33 of which were described by Chung et al. in 20093 and another 6 cases published afterwards.1,2,4 From all these reports, we have noted some interesting data. For instance, the predominant histologic type in all these cases was clear-cell carcinoma, probably because it is the most common histologic type of RCC. Out of the 39 cases published, in five the histological type was not defined and the rest were all clear-cell.
As in our case, the majority of the patients were asymptomatic at the time of diagnosis, and the lesions were radiological findings made during either follow-up or an extension study of RCC.
Metastasis in the gallbladder is a result of systemic dissemination and not by direct involvement of the renal tumor since in all cases these metastases affect the gallbladder lumen instead of the serosa. Furthermore, as in our case, the majority are metachronous metastases with an average latency period of 4 years.3
As in the case of our patient, among the cases published there is contralateral kidney involvement in about 30% (11 out of 39 patients), compared with 5% involvement of the contralateral kidney in the remaining cases of RCC.3
Finally, in spite of the small series of cases, it seems that the survival of patients with solitary metastasis in the gallbladder who undergo cholecystectomy is similar to the survival of patients with a single metastasis in other locations who have had the metastasis removed.2,3
Please cite this article as: Zevallos Quiroz JC, Lizarazu Pérez A, Guisasola Gorrochategui E, Medrano Gomez MÁ, Jiménez Agüero R. Metástasis a vesícula biliar de un carcinoma de células renales, un sitio extremadamente raro de diseminacioń neoplásica. Cir Esp. 2014;92:295–296.
