





Intravenous leiomyomatosis is a histologically benign, rare disease in which smooth muscle cells proliferate intravascularly without invading other structures. They reach the intrauterine veins and, occasionally, can reach the retroperitoneal vessels and even the right cardiac chambers. It usually affects women aged 40–50.
Few case reports have been reported. We present an uncommon case and briefly comment on a review of the literature.
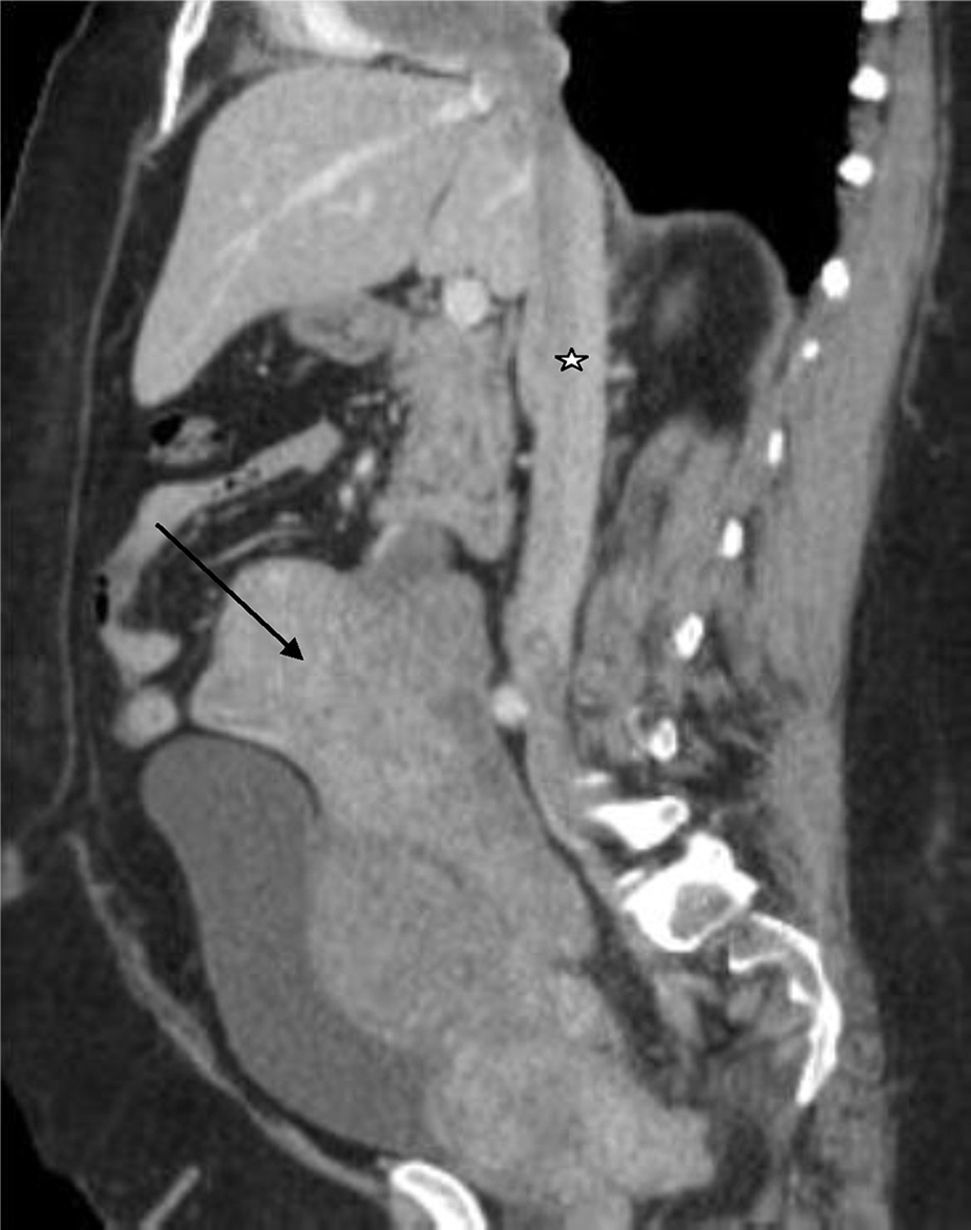
The patient is a 53-year-old woman who was in follow-up by cardiology due to episodes of syncope. Upon physical examination, a pelvic mass was palpated that reached the navel region, which was hard in consistency and painful to the touch. Thoracoabdominal-pelvic CT scan with intravenous contrast (Fig. 1) showed evidence of a multilobulated mass with heterogenous densitometry corresponding with a myomatous/sarcomatous uterus, thrombosis of the right ovarian vein and involvement of the inferior vena cava up to the right atrium. Echocardiogram demonstrated a dilated right ventricle; the right atrium presented a mobile homogeneous mass measuring 26mm×35mm that prolapsed towards the right ventricle; the inferior vena cava was also occupied. Biopsy results defined the lesion as a leiomyoma. The patient study was completed with PET/CT, which showed a mildly hypermetabolic tumour, suggesting uterine leiomyoma, and hypometabolism in the inferior vena cava and right atrium, not suggestive of tumour thrombosis.
 and tumour growth in the iliac, ovarian and caval veins (star), up to the right atrium.")
On 6 May 2015, surgery was performed by 2 surgical teams (General and Digestive Tract Surgery together with Cardiac Surgery) in 1 single operation (410min), which included: resection of the uterine leiomyoma by hysterectomy with bilateral adnexectomy; excision of the intercaval and right interatrial tumour expansion, requiring cardiopulmonary bypass without cardiac arrest. The surgical specimens were sent for pathology study, which confirmed intravenous leiomyomatosis (Fig. 2).

The patient was admitted to the Recovery Unit for 5 days and was later transferred to the Abdominal Transplantation Unit, where the patient's condition improved satisfactorily. She was discharged 23 days after surgery.
Intravenous leiomyomatosis affects women, mainly after hysterectomy due to uterine leiomyomata.1 In this condition, these benign smooth muscle tumours demonstrate intravascular expansion and can even reach the heart chambers through the inferior vena cava, obstructing venous return. In 2013, fewer than 300 cases were registered in the English-speaking medical literature.2
Some theories for the origin and growth mechanisms of these tumours include3:
- •
Intravenous local extension of leiomyomata
- •
Direct carcinogenesis from the vascular walls within the myometrium; the tumour can float freely within the lumen of the vessel or adhere to it.
The diagnosis should be considered in cases of deep vein thrombosis, mass within the inferior vena cava or atrium, or non-specific symptoms associated with a history of pelvic surgery, such as hysterectomy.4
Symptoms are variable, including: pelvic pain and vaginal bleeding; respiratory and cardiac symptoms (dyspnoea, cough, right heart failure). On certain occasions, the intracardiac extension of these tumours can lead to sudden cardiac death.5
Diagnostic studies involve:
- •
Tomography: provides evaluation of the tumour extension.
- •
Magnetic resonance: shows low to intermediate signal intensity in T1.
- •
Pelvic ultrasound: studies the uterine adnexa and the presence of intravascular thrombus; also assesses intracardiac involvement.6
The treatment of choice is surgery with complete tumour excision to avoid recurrences. This can be done in two operations (less risk for haemorrhage due to anticoagulation during cardiopulmonary bypass) or in one (good results have been observed).7 There have been reports of cases in which cardiac arrest was necessary for correct tumour excision.
In cases of incomplete resection or tumour recurrence, the use of anti-oestrogen drugs such as tamoxifen is controversial. Recurrence rates of up to 30% have been reported in incomplete resections, and recurring intravenous leiomyomatosis may appear 6 months to 15 years later; therefore, long-term follow-up is essential.8
Please cite this article as: Calvo-Rodríguez D, Narváez Muñoz A, Fernández Pérez A, Durán D, Varo Pérez E. Leiomiomatosis intravascular con extensión intracardiaca: cirugía abdominal y cardíaca en un solo tiempo. Cir Esp. 2016;94:306–307.
