




The thyroid gland develops from 2 embryonic origins: one medial endodermal, which produces most of the thyroid parenchyma, and 2 lateral (branchial bodies), formed by the 4th pharyngeal pouch that give rise to C cells.
In its embryonic development, the thyroid descends through the thyroglossal duct from the base of the tongue towards the anterior tracheal wall. Incorrect descent can lead to an ectopic thyroid. This anomaly appears in 7% of the population.1,2 The most frequent locations are in the area of the descent on the midline and are classified as lingual, sublingual, thyroglossal and intralaryngotracheal. The lingual location is the most frequent and represents around 90% of cases.3 Other less frequent locations are: cervical lymphatic nodules, pericardium or cervical oesophagus.
Traditionally, the thyroid tissue located in the lateral cervical compartments was known as lateral aberrant thyroid tissue and was believed to be an embryological variation. Currently, this is not clear, and many authors defend its origin as metastatic deposits of well-differentiated thyroid carcinoma.
We present 2 clinical cases of ectopic thyroid tumours located in the lateral cervical region that address these hypotheses about the origin of this tumour type.
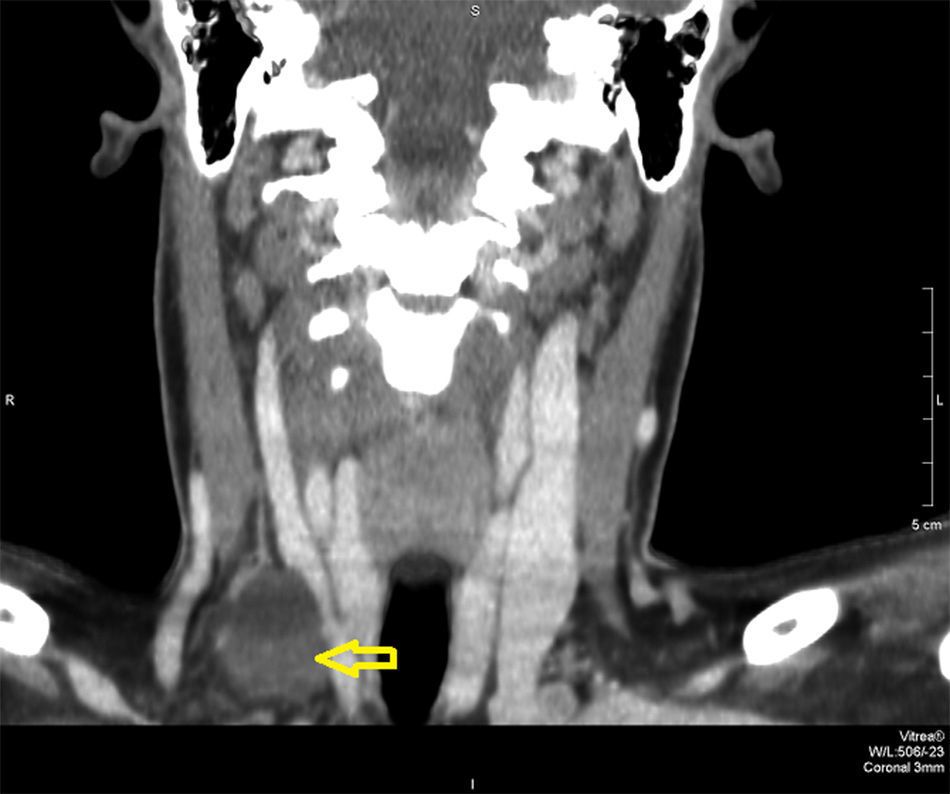
Case 1: A 35-year-old woman reported a right lateral cervical mass that had been progressing over the previous 2 months. Ultrasound revealed an ovoid right lateral neck lesión measuring 3.5cm, indicative of lymphadenopathy or cystic neoformation. Fine needle aspiration (FNA) confirmed papillary thyroid carcinoma. Thyroid function tests showed: TSH 0.98mIU/mL; T3 3.04pg/mL; and T4 0.77ng/dL. Cervical computed tomography demonstrated a hypodense nodule measuring 2.2cm behind the sternocleidomastoid muscle, indicative of metastatic lymphadenopathy (Fig. 1), and the thyroid gland with no alterations.

Intraoperative biopsy detected ectopic thyroid tissue with cystic colloid nodule and carcinoma. Given this finding, we performed total thyroidectomy as well as central cervical and homolateral functional lymph node dissection.
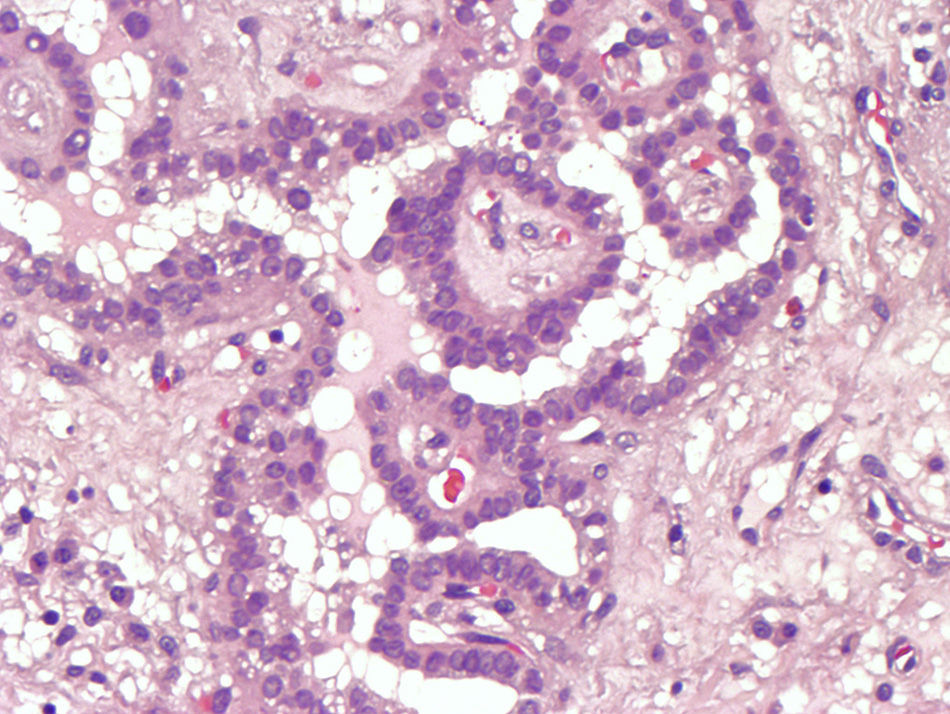
The pathology results reported a cystic formation with liquid colloid material and solid excrescent mass that was papillary in appearance and compatible with ectopic thyroid nodule with papillary carcinoma (Fig. 2). The thyroid gland presented colloid goitre, with no signs of malignancy. Nonspecific chronic lymphadenitis was detected in the 9 lymph nodes that were analysed. After 11 months of follow-up, the patient has had no local or distant recurrence.
.")
Case 2: The patient is a 58-year-old male with a large goitre of the right lobe that extended towards the lateral cervical region. Cervical ultrasound detected a 6-cm nodule in the right thyroid lobe. The thyroid function study revealed: TSH 1.30mIU/mL; T3 2.98pg/mL; and T4 0.66ng/dL. FNA diagnosed a follicular lesion (Bethesda III).
After arriving at the diagnosis of multinodular goitre with a dominant right nodule and follicular proliferation, surgical treatment was indicated. Right hemithyroidectomy and isthmectomy were performed. After extending the cervical access, the procedure was completed with the resection of the nodule, which was completely extrathyroidal and located behind the sternocleidomastoid muscle, but the macroscopic appearance was thyroidal. The histology study determined the surgical specimen was a right hemithyroid with adenoma follicular and ectopic thyroid nodule with follicular thyroid adenoma.
Ectopic thyroid glands are defined as thyroid tissue situated outside its usual location. The lateral location is least frequent and limited to 1%–3% of all cases.1,3 This ectopic tissue can represent metastasis of a thyroid carcinoma and, very rarely, can include a primary thyroid carcinoma.2
The appearance of thyroid tissue along the midline descent pathway of the gland during the embryonic period is easily demonstrable, but not so its appearance in other locations. Traditionally, it has been suggested that lateral cervical thyroid tumours would have originated from lateral thyroid remains that were deposited outside the gland as it descended from the base of the tongue to the triangular cervical muscles and, therefore, were considered ectopic thyroid tissue.4
For years, several authors have questioned this hypothesis.4,5 Currently, most would be willing to consider that the thyroid tissue in this area are lymph node metastases of a differentiated thyroid carcinoma that remains clinically occult due to its small size.5,6 The fact that the pathology study of the lesion showed no lymph tissue would only reflect that the differentiated thyroid carcinoma had completely replaced the lymph node tissue.7
Although this second hypothesis has a clear oncologic explanation and could justify the appearance of many thyroid gland ectopias, there are cases, such as those we have presented, that cannot be demonstrated.
In the first case, the mass was compatible with thyroid papillary carcinoma. This thyroid tissue could represent a metastasis, but after a detailed pathology study of the thyroid gland, no primary tumour was detected that could have been the origin of the metastasis.
In the second case, the resected nodular lesion from the posterior margin of the sternocleidomastoid muscle was diagnosed as follicular adenoma of the thyroid. Thyroid adenomas are benign tumours, so oncologic dissemination would also not explain the existence of tissue in this region.
These findings would raise questions about the oncologic hypothesis in favour of the classical premise of migration during the embryonic period.
In the literature, there is no consensus about the best treatment of lateral cervical ectopic thyroid due to the rarity of this clinical condition and the limited number and short time periods of the published series. We propose that the best treatment is exeresis of the lesion in association with total thyroidectomy plus central and homolateral lymph node dissection for differentiated carcinomas since, even if no primary lesion were found, treatment would be similar to that of lymph node metastasis.8
Please cite this article as: Sánchez Fuentes MN, Miguelena Bobadilla JM, Casamayor Franco MC, Barranco Domínguez JI, Dobón Rascón MÁ. Tumor laterocervical de cuello: tiroides ectópico vs. metástasis de carcinoma tiroideo diferenciado. Cir Esp. 2015;93:e115–e117.
