




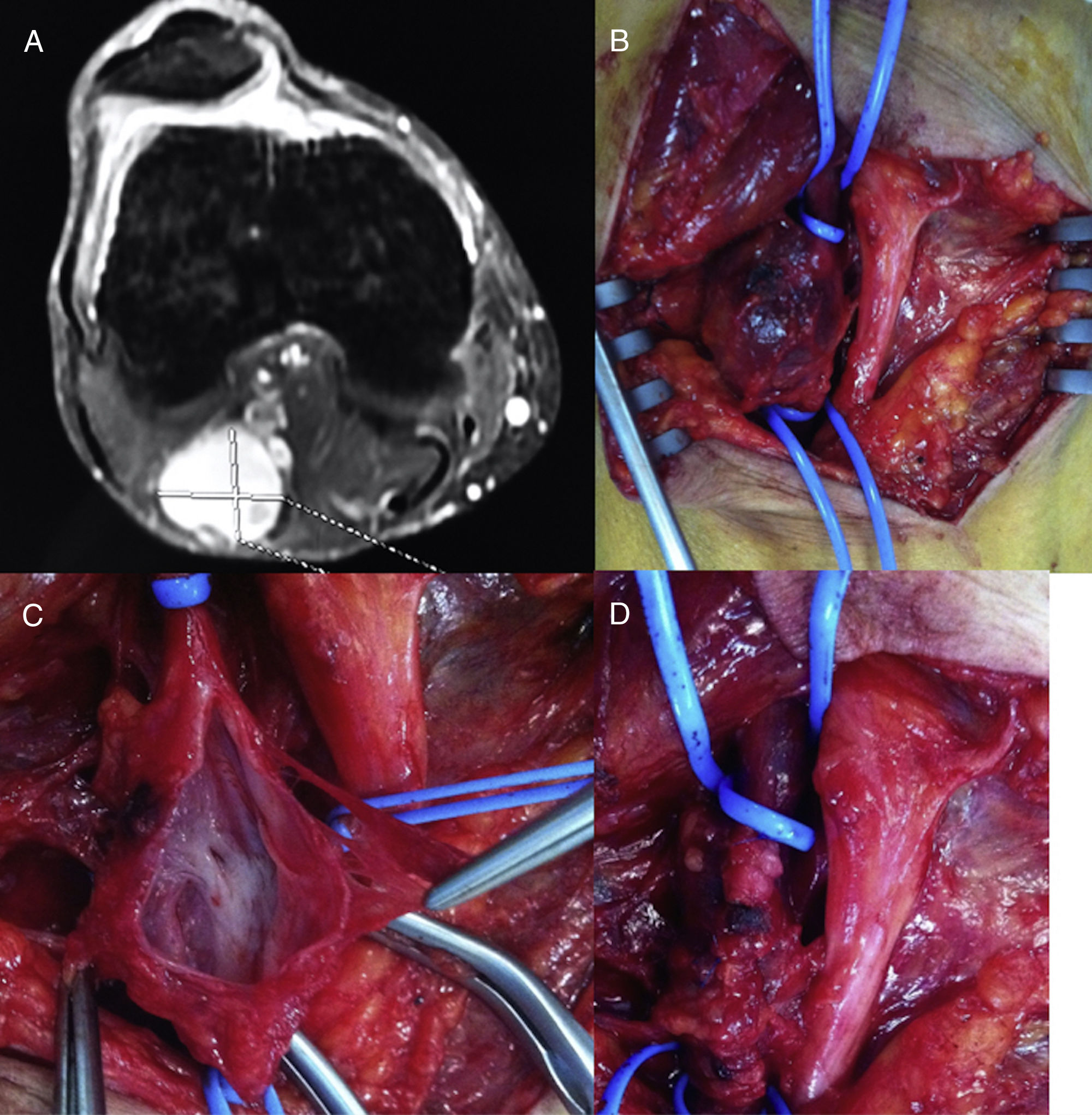
Popliteal venous aneurysms are a rare disease of uncertain etiology that can present with serious complications, such as deep vein thrombosis and pulmonary embolism. We present the case of a 42-year-old man who worked on a truck trailer assembly line placing screws while in a squatting position, involving repeated flexion and extension of the knees (greater force and load on the right side as he was right-handed) for 8h/day. The patient consulted with our department due to a painful tumor in the right popliteal fossa. On physical examination, a soft, non-pulsatile mass was observed; the remaining vascular examination was normal. Doppler ultrasound and venous MR angiography revealed a saccular popliteal venous aneurysm measuring 2.7×3.4cm, with no signs of thrombosis (Fig. 1A). No muscle, ligament or tendon anomalies were observed in the popliteal fossa or in the adductor canal. We indicated surgery, which was performed with the patient in prone decubitus, using a bayonet incision and under systemic heparinization, dissection of the aneurysm, tangential aneurysmectomy and lateral venorrhaphy of the popliteal vein (Fig. 1B–D). The patient was discharged 48h later with no complications and prescribed treatment with low molecular weight heparin for 3 months and elastic compression, as well as a subsequent dose of 100mg of ASA. The pathology study reported hypertrophy and generalized fibrosis of the vessel wall. After 18 months of follow-up, the patient presented no complications, with permeability of the vascular reconstruction and no recurrence of the venous dilatation on the ultrasound study.
 Popliteal venous aneurysm on magnetic resonance angiography; (B) intra-operative image of the venous aneurysm; (C) detail of open venous aneurysm; (D) result after tangential aneurysmectomy with lateral venorrhaphy.")
Popliteal venous aneurysms are a rare disease of uncertain etiology, which can present with serious complications such as deep vein thrombosis and pulmonary embolism. A popliteal venous aneurysm is defined by a popliteal vein>20mm in diameter. In the majority of published cases, the most frequent type is saccular. Most cases present with symptoms of pulmonary embolism or are discovered incidentally; very rarely is there a painful popliteal mass, as in the case of our patient. Since pulmonary embolisms and death have been reported even in patients without thrombi, surgical excision is also recommended in asymptomatic patients.1–3 In addition, in patients with pulmonary embolism with no risk factors or a clear source of emboli, popliteal venous aneurysm should be ruled out.3 The recommended and most frequently performed technique is tangential aneurysmectomy with lateral venorrhaphy because it has fewer associated complications.2 Currently, endovascular treatment is not recommended.3 The etiopathogenesis of popliteal venous aneurysms is uncertain, with the possible intervention of a combination of mechanical, trauma, inflammatory, hemodynamic or congenital disease factors.4 We cannot confirm that repeated trauma to the right popliteal vein due to the position and movements of our patient while at work were the cause of his popliteal venous aneurysm, but, along with genetic predisposition, this may have been a contributing factor.
We have found no reports in the literature of popliteal venous aneurysms in patients performing repeated and continuous movements and positions in the workplace that may cause compressive trauma to the popliteal vein.
Please cite this article as: Cano-Trigueros E, Díaz-Serrano R. Tratamiento quirúrgico de aneurisma venoso poplíteo en paciente joven. Cir Esp. 2018;96:517–518.
