





Chest wall deformities/defects and chest wall resections, as well as complex rib fractures require reconstruction with various prosthetic materials to ensure the basic functions of the chest wall. Titanium provides many features that make it an ideal material for this surgery.
The aim is to present our initial results with this material in several diseases.
Material and methodsFrom 2008 to 2012, 14 patients were operated on and titanium was used for reconstruction of the chest wall. A total of 7 patients had chest wall tumours, 2 with sternal resection, 4 patients with chest wall deformities/defects and 3 patients with severe rib injury due to traffic accident.
ResultsThe reconstruction was successful in all cases, with early extubation without detecting problems in the functionality of the chest wall at a respiratory level. Patients with chest wall tumours including sternal resections and with chest wall deformities were extubated in the operating room. Chest trauma cases were extubated within 24h from internal rib fixation. There were no complications related to the material used and the method of implementation.
ConclusionsTitanium is an ideal material for reconstruction of the chest wall in several clinical situations allowing for great versatility and adaptability in different chest wall reconstructions.
La resección y las deformidades/defectos de la pared torácica así como las fracturas costales complejas requieren de reconstrucción con diversos materiales protésicos para garantizar las funciones básicas de dicha pared. El titanio aporta múltiples características que lo hacen un material idóneo para esta cirugía.
El objetivo es presentar nuestros resultados iniciales con este material en diversas afecciones.
Material y métodosDe 2008 a 2012 se ha intervenido a 14 pacientes en los que se ha empleado el titanio para la reconstrucción de la pared torácica. Un total de 7 pacientes presentaban tumores de pared torácica, 2 de ellos con resección esternal, 4 con deformidades/defectos de la pared torácica y 3 pacientes con traumatismo costal severo por accidente de tráfico.
ResultadosLa reconstrucción fue satisfactoria en todos los casos, con extubación temprana y sin detectar problemas en la funcionalidad de la pared torácica a nivel respiratorio. Los pacientes con tumores de pared torácica, incluyendo las resecciones esternales, se extubaron en quirófano, así como las deformidades de pared torácica. Los casos de traumatismo torácico se extubaron en menos de 24h desde la fijación costal interna. No hubo complicaciones en relación con el material utilizado ni con el método de implantación.
ConclusionesEl titanio es un material ideal para la reconstrucción de la pared torácica en diversas situaciones clínicas, al permitir una gran versatilidad y adaptabilidad en las diferentes reconstrucciones de pared torácica en que se quiera emplear.
Chest wall resections or deformities sometimes require complicated reconstruction for which several prosthetic1 materials are used with the necessary traits to ensure maintenance of the basic functions of the chest1,2 (protection of thoracic organs, mechanical ventilation). Titanium prostheses3,4 are highly advantageous compared with traditional rigid prostheses due to the characteristics of the material (malleability, ductility, toughness, tensile strength, shape memory capacity, hypoallergenic properties). This results in relatively simple insertion and excellent final results.4
Its versatility promotes use in many different interventions including chest wall resection, repair of chest wall deformities and surgical rib fracture repair.5
Material and MethodsFrom September 2008 to August 2012 a prospective record of consecutive patients was made for whom the Strasbourg Thoracic Osteosyntheses System ([STRATOS] MedXpert, Heitersheim, Germany) titanium connecting bar system and the Strasbourg Costal Osteosyntehsis System ([STRACOS] MedXpert, Hitersheim, Germany) titanium clip system were used for chest wall reconstruction or repair. The database included clinical data, daily follow-up, a record of complications and, in the case of oncology patients, long-term outpatient neoplasia follow-up.
14 patients were operated on (8 men and 6 women, with an age range from 17 to 78 and mean age of 58) for diverse disorders which were divided into 3 groups: chest wall tumours, chest wall defects/deformities and rib fractures with unstable thorax (Table 1).
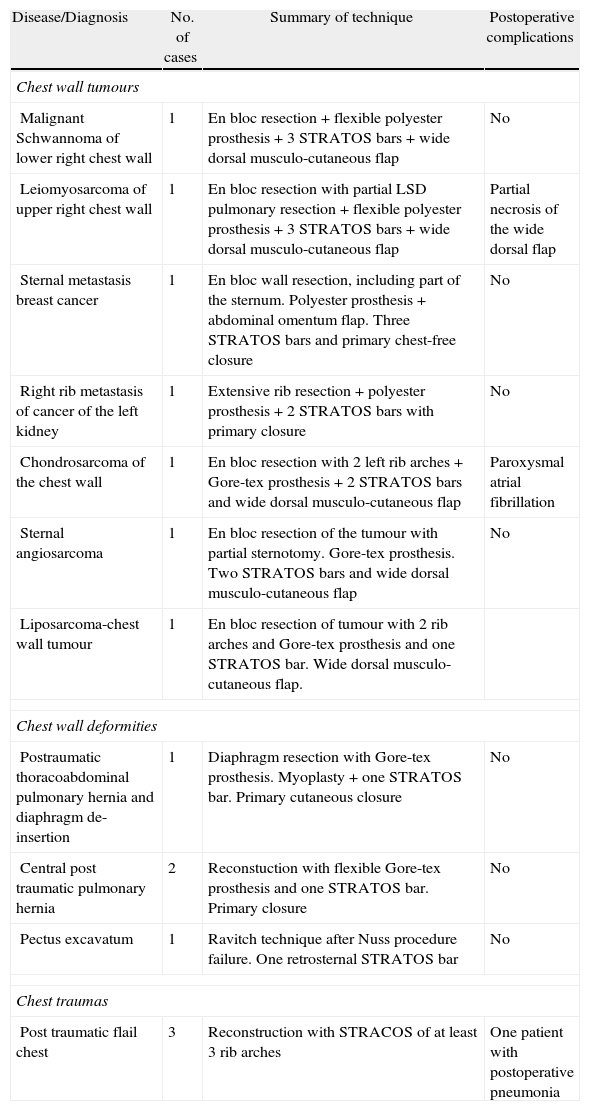
Summary of Clinical Cases and Surgical Techniques.
| Disease/Diagnosis | No. of cases | Summary of technique | Postoperative complications |
| Chest wall tumours | |||
| Malignant Schwannoma of lower right chest wall | 1 | En bloc resection+flexible polyester prosthesis+3 STRATOS bars+wide dorsal musculo-cutaneous flap | No |
| Leiomyosarcoma of upper right chest wall | 1 | En bloc resection with partial LSD pulmonary resection+flexible polyester prosthesis+3 STRATOS bars+wide dorsal musculo-cutaneous flap | Partial necrosis of the wide dorsal flap |
| Sternal metastasis breast cancer | 1 | En bloc wall resection, including part of the sternum. Polyester prosthesis+abdominal omentum flap. Three STRATOS bars and primary chest-free closure | No |
| Right rib metastasis of cancer of the left kidney | 1 | Extensive rib resection+polyester prosthesis+2 STRATOS bars with primary closure | No |
| Chondrosarcoma of the chest wall | 1 | En bloc resection with 2 left rib arches+Gore-tex prosthesis+2 STRATOS bars and wide dorsal musculo-cutaneous flap | Paroxysmal atrial fibrillation |
| Sternal angiosarcoma | 1 | En bloc resection of the tumour with partial sternotomy. Gore-tex prosthesis. Two STRATOS bars and wide dorsal musculo-cutaneous flap | No |
| Liposarcoma-chest wall tumour | 1 | En bloc resection of tumour with 2 rib arches and Gore-tex prosthesis and one STRATOS bar. Wide dorsal musculo-cutaneous flap. | |
| Chest wall deformities | |||
| Postraumatic thoracoabdominal pulmonary hernia and diaphragm de-insertion | 1 | Diaphragm resection with Gore-tex prosthesis. Myoplasty+one STRATOS bar. Primary cutaneous closure | No |
| Central post traumatic pulmonary hernia | 2 | Reconstuction with flexible Gore-tex prosthesis and one STRATOS bar. Primary closure | No |
| Pectus excavatum | 1 | Ravitch technique after Nuss procedure failure. One retrosternal STRATOS bar | No |
| Chest traumas | |||
| Post traumatic flail chest | 3 | Reconstruction with STRACOS of at least 3 rib arches | One patient with postoperative pneumonia |
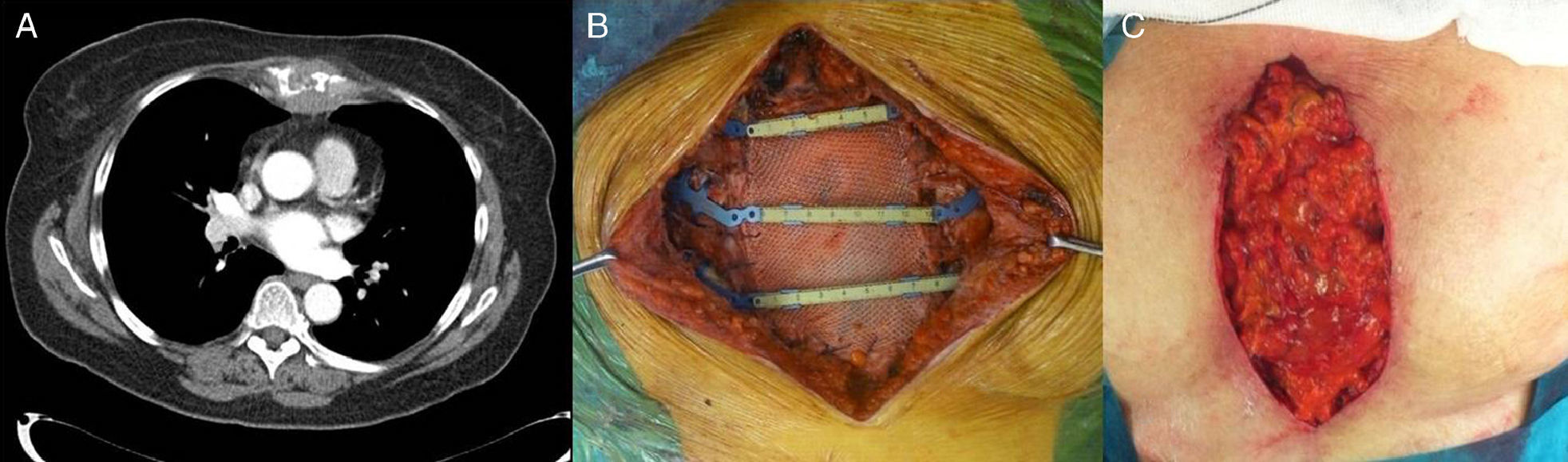
The criteria for STRATOS usage in patients with chest wall tumours (7) were: extended resection which included several anterolateral ribs or sternal resection. Reconstruction in the case of chest tumours was always accompanied by a flexible prosthesis to protect the intrathoracic content from the titanium connecting bar system (4 polyester prosthesis covered with resorbable collagen and 3 Gore-tex prostheses), depending on the size of the overall defect. Muscle flap closure was used for the defects (in 5 cases latissimus dorsi flaps and in 1 case chest flap), with the exception of one case of primary closure. In one of the sternal resection cases with previous radiotherapy (Fig. 1), the greater omentum was used to protect the organs and provide better adaptation of the prosthetic material. Only in the case of one patient (with upper thoracic wall leiomyosarcoma) was en bloc resection combined with an atypical resection of the upper right pulmonary lobe due to tumour infiltration.
 Chest CT where sternal metastasis may be observed. (B) STRATOS connecting bars and flexible prosthesis. (C) Greater omentum covering the defect below and above the bars.")
One bar was used in one patient, 2 in 3 patients and 3 in 3 patients. Chest drainage insertion was used for the soft tissues between the bars and the muscle flap.
Choice of type and number of bars was always made in the operating theatre following surgical extraction, after taking the measurements of the defect and discovering the position of the rib tips and their spatial orientation, with an anatomical (parallel) or crossed over positioning (2 patients).
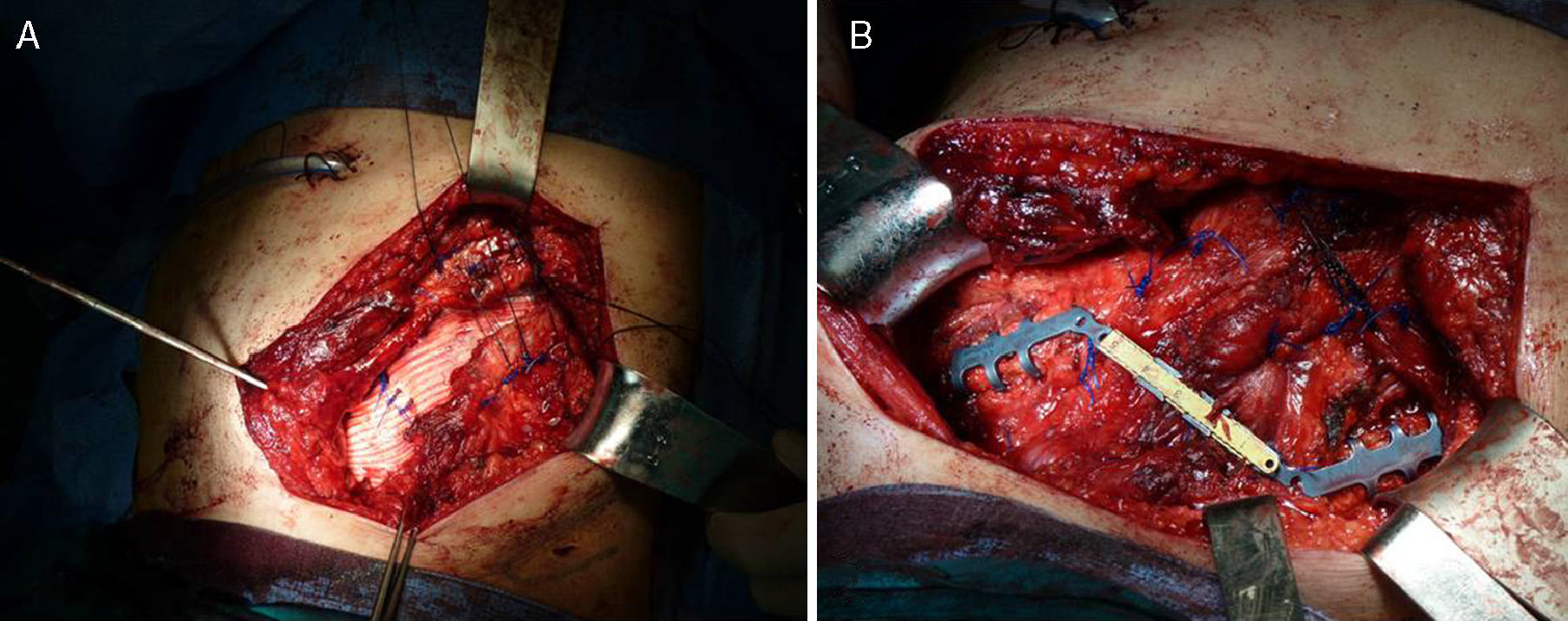
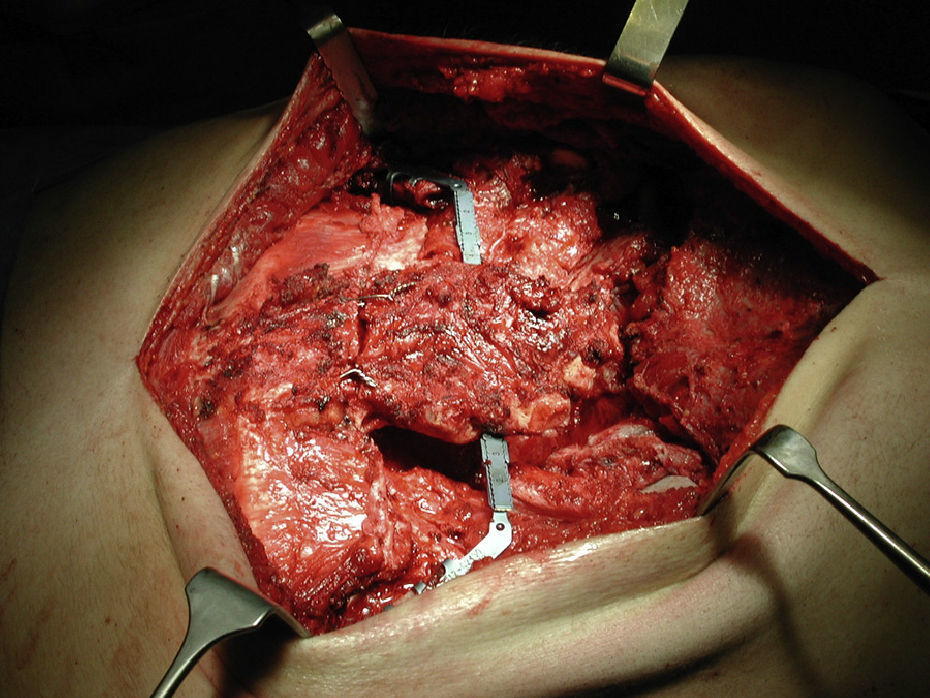
Chest Wall Deformities and Defect PatientsIn this patient group of 4 patients, 3 had deformities from previous trauma and presented with pulmonary hernia (Fig. 2) and 1 patient presented with pectus excavatum for whom the Nuss procedure had failed and who was reoperated by sternochondroplasty (Ravitch technique) with support from a retrosternal titanium bar (Fig. 3) which was placed after osteotomy and sternal anatomical replacement. Indications were to prevent recurrence in all cases, prevent collapse of the sternum in the pectus excavatum and restore normal anatomy. In the 3 pulmonary hernia cases a flexible prosthesis was inserted (Gore-tex in all cases).
 Detail of the diaphragmatic resection supported by Gore-tex prosthesis. (B) STATOS connecting bar above themyoplasty.")

Surgery was performed on 3 patients with severe rib injury (Fig. 4). Indication in all cases was the impossibility of mechanical ventilation extubation (over 7 days of mechanical ventilation). None of the 3 patients had intrathoracic lesions which required emergency surgery. Titanium clips were attached to at least 3 rib arches. In cases where there was double fracture a clip was attached to each rib fragment (Fig. 4). Open pleura chest drainage and subcutaneous drainage for prevention of postoperative seroma were performed in all 3 cases.
ResultsPatients With Chest Wall Tumours
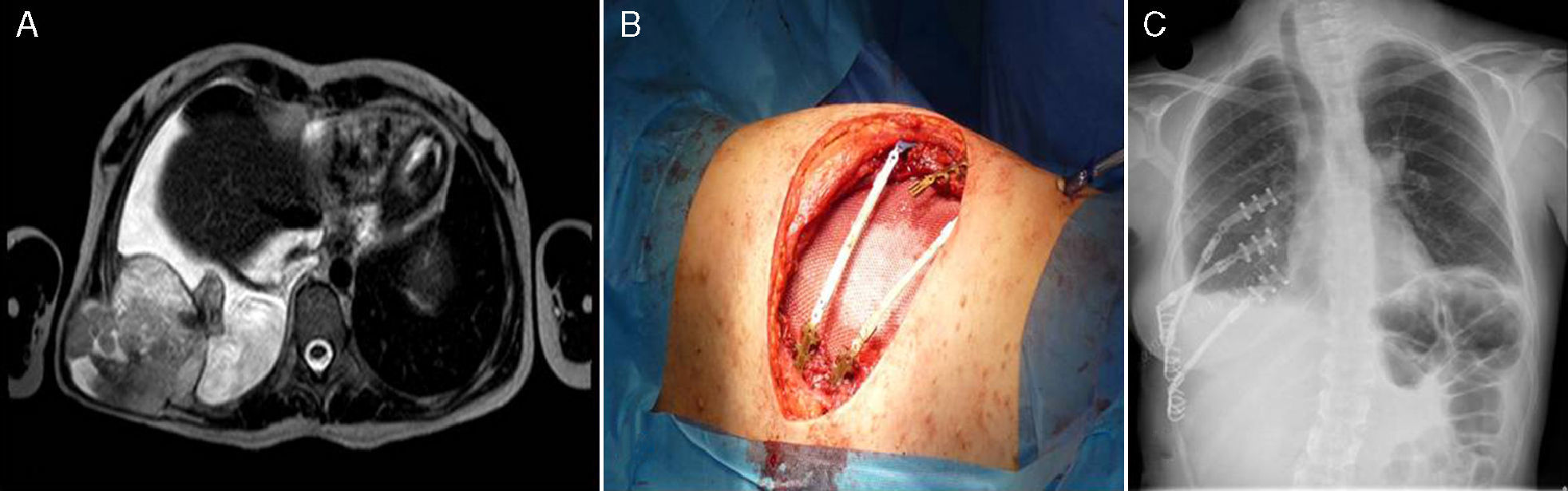
Anatomopathological results were heterogeneous in the 7 patients (5 women and 2 men): 5 cases of primary chest wall tumours (1 chondrosarcoma, 1 malignant Schwannoma in the context of neurofibromatosis (Fig. 5), 1 leiomyosarcoma, 1 angiosarcoma and 1 liposarcoma) plus 2 metastatic cases (1 sternal metastasis from breast cancer and 1 rib metastasis from renal cancer). In all cases complete en bloc resections with tumour free borders were achieved, from disorders confirmed by anatomopathological analysis. All patients were extubated at the end of surgery with no complications. Average postoperative hospital stay was 6.2±2 days. Only 2 complications were recorded (Table 1): partial flap necrosis (patient with leiomyosarcoma) where single use negative pressure wound therapy system [PICO]) was performed and primary closure was performed 20 days after the initial surgery; and a paroxysmal atrial fibrillation which was treated pharmacologically.
 Preoperative thoracic MRI where an extensive lesion is observed. (B) View of flexible prosthesis and 2 STRATOS bars in place. (C) Radiography of thorax for postoperative control. Observe how in this case we inserted 2 of the bars in a crossed-over position.")
Thirty days after surgery none of the patients needed pharmacological analgesia because of pain related to surgery.
In all cases oncological follow-up continued for over a year. 18 months after surgery only 1 death (patient with malignant schwannoma) was recorded. One leiomyosarcoma patient presented a single contralateral lung metastasis treated with atypical resection by videothorascopy 10 months after the initial surgery. One patient with sternal metastasis after breast cancer presented cerebral metastasis 5 months after surgery which required oncological treatment. Twelve months after the above mentioned chest wall surgery, the patient with rib metastasis from cancer of the kidney was diagnosed with lumbar and sternal bone metastasis. None of the patients presented local recurrence of their disease. The other (3) patients presented a mean follow-up of 16±3 disease-free months.
Patients With Chest Wall Deformities or DefectsThe 4 patients were 3 men and 1 woman aged between 17 and 26. Average hospital stay was 4 days (3–6 days). At 30 days no postoperative complications had been recorded. None of the patients took analgesics one month after surgery. Both functional and cosmetic results were satisfactory. Follow-up was at least 12 months (12–19 months) in the 3 patients with no evidence of recurrence.
Patients With Severe Rib InjuryThe 3 patients were men with an average age of 56 years (range: 45–63). All cases were due to traffic accidents. Mean rib fractures were 9 rib arches (7–12 rib arches). All patients were admitted to the Intensive Care Unit (ICU). None presented brain injury, verified by CT scan. There were no intrathoracic injuries which required emergency surgery. One patient presented an open tibia fracture which required surgery on admittance and another had needed a chest drain which had already been positioned for pneumothorax. Two patients were admitted to hospital with intubation (one was the patient with the tibia fracture) and the third patient was intubated 6h after admittance suffering from respiratory failure. Extubation was attempted in all 3 patients without success. They received mechanical ventilation for at least 7 days. All patients were extubated 24h after surgery and left the ICU in less than 48h. No intraoperative complications were recorded. One patient presented an ipsilateral pneumonia in the hemithorax on which surgery had been performed. The patient responded to antibiotherapy. No other postoperative complications were recorded. Overall average stay was 18 days (15–23 days). The patients were monitored at 1 month and 3 months following discharge, with satisfactory radiological and clinical condition.
DiscussionExtended wall resections, chest deformities and multiple rib fractures leading to chest wall failure present a challenge to the surgeon.1 Several materials have been used in chest wall reconstruction. All aim to preserve mechanical ventilation and its rigidity with a satisfactory cosmetic result, as indicated by Weyant et al.2 Traditional materials such as methylmethacrylate6 or steel elements7 have disadvantages such as longer surgery times, lack of material flexibility and even toxicity in the case of methylmethacrylate. Our case sample and several publications3–5,7–11 have shown that, due to its intrinsic characteristics, titanium aids reconstruction and repair of the rib cage and the STRATOS and STRACOS systems, in particular, offer great versatility, regardless of resection size (very large resections can be performed and reconstructed with titanium4) and type of disease to be treated. Furthermore, in both CT and MRI scans, titanium produces more precise images with fewer artefacts than steel. This is of extreme importance in cancer patient follow-up care.5,9 The learning curve is short and insertion is simple and safe, as indicated by Berthet et al.4
One of the main concerns after chest wall reconstruction or internal rib fixation is mechanical ventilation and pulmonary function disorder after surgery.2,8 All our patients could be extubated after surgery in the operating theatre and the patients with internal rib fixation were extubated less than 24h after surgery. As stated by Weyant et al.2 the importance of this is that both local and general postoperative complications are reduced. This is the main aim of reconstruction. In our series there were no cases of postoperative mortality, which was probably due to the lower number of complications.
Another major factor is postoperative pain, as indicated by both Moreno de la Santa et al.5 and Fabre et al.9 In our series, none of the patients needed analgesics 30 days after surgery. Although rupture of material has been described7 no cases were observed in our series, not even in patients with longer follow-up periods. Furthermore, as previously stated, titanium rarely deteriorates, does not corrode, is biocompatible and chemically inert.9
The pectus excavatum was an isolated case, but turned out to be a good option to reinforce the Ravitch technique and all the more so, bearing in mind that the patient had relapsed following removal of the Nuss bar. Furthermore, another case with similar characteristics and an identical result has been reported.12
Our experience with internal rib fracture fixation was positive. Early extubation following surgery (in less than 24h) was achieved and postoperative evolution was favourable, even in the patient treated for pneumonia. Analysis of greater sample sizes13 and our experience favours early rib fixation rather than pneumatic stabilization, since there will be fewer complications, reduced hospital stay and lower cost by reducing ICU stay (the 3 patients were in ICU for less than 48h). Cost analysis of titanium implants is lower than that of a higher hospital stay with prolonged pneumatic stabilization.2
We conclude, therefore, that at present titanium and specifically the STRATOS and STRACOS systems are the best options for chest wall reconstruction and repair: easy to insert, versatile and with all the necessary characteristics for the chest wall to continue functioning in the short and long term.
Conflict of InterestsThe authors have no conflict of interests to declare.
Please cite this article as: Córcoles Padilla JM, Bolufer Nadal S, Kurowski K, Gálvez Muñoz C, Rodriguez Paniagua JM. Utilidad y versatilidad del titanio para la reconstrucción de la pared torácica. Cir Esp. 2014;92:89–94.
