



Ophthalmoscopic scrutiny of the nerve fiber layer was first advocated by Hoyt,1 over 30 years ago. In the following years, the importance of localized defects of the retinal nerve fiber layer (NFL) for the diagnosis of glaucoma has been demonstrated in many studies. The evaluation of the NFL, though relatively difficult and subjective, has become routine in the common ophthalmic examination.2 We present a case of an isolated NFL defect with different possible etiologies.
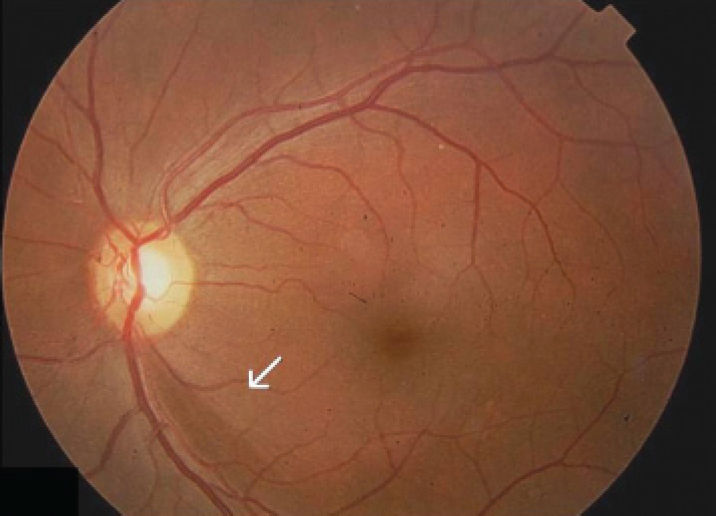
DESCRIPTION OF THE CASEA 45-year-old white man with diabetes mellitus and systemic arterial hypertension was referred for routine consultation. Ophthalmological examination revealed a best corrected visual acuity of 20/20 in both eyes (OU). Slitlamp biomicroscopy and gonioscopy were unremarkable. The patient presented with intraocular pressures (IOP) that ranged from 13 to 16 mmHg OU, which was confirmed on modified diurnal curve monitoring. Cup-disk ratios were 0.6 OU, with healthy neural rims, without evidence of thinning, notching, or localized pallor. However, there was an evident inferior-temporal wedge-shaped defect of the NFL on the left eye (Figure 1). There were no signs of diabetic retinopathy OU. The patient had an unremarkable family history.
")
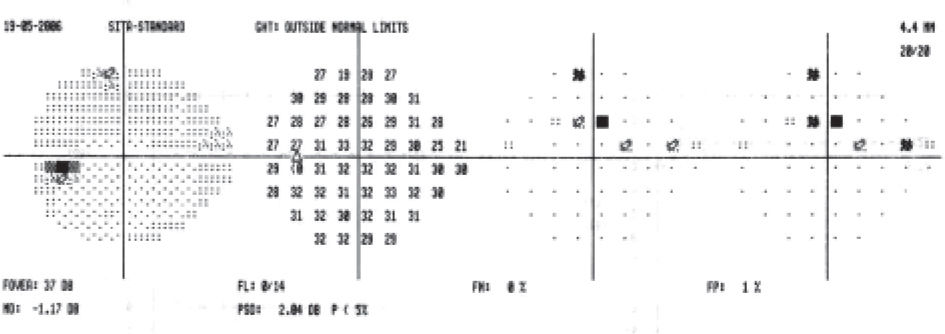
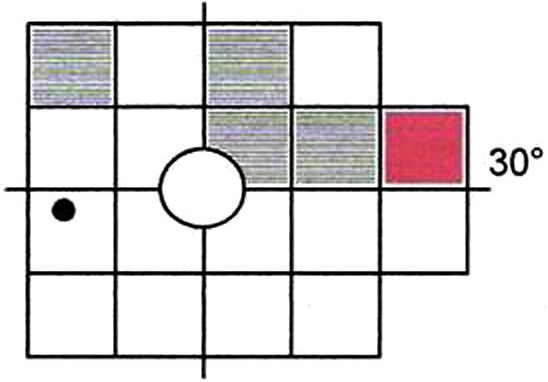
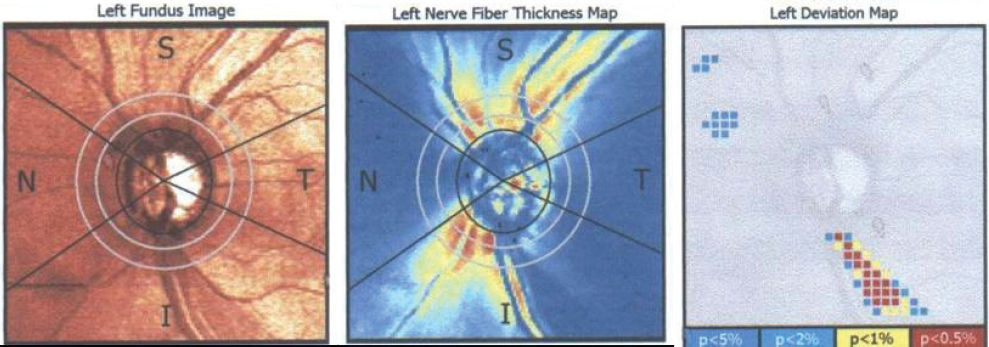
Subsequent psychophysical testing confirmed a superior initial defect on the visual field of this eye with conventional achromatic perimetry (SITA Standard 24-2) (Figure 2) and frequency doubling perimetry (Figure 3). Short-wavelength perimetry was normal OU. The nerve fiber analysis with scanning laser polarimetry (GDx VCC – Laser Diagnostic Technologies, San Diego, CA) showed nerve fiber layer regional inferior defects OU, which were more evident in the left eye (Figure 4), both on the reflectance image and on the retardation image. Confocal scanning laser ophthalmoscopy (HRT - Heidelberg Retina Tomograph, Heidelberg Engineering GmbH, Germany) was borderline in the left eye, and optical coherence tomography (Stratus OCT – Carl Zeiss Meditec) was unremarkable. Except for the GDx, all tests were normal for the right eye.
DISCUSSION


At times when pre-perimetric diagnosis of glaucoma is the goal, the search for the subtle signs of damage in the NFL is of utmost importance. Retinal nerve fiber layer defects have been shown to be among the earliest signs of glaucomatous damage, and they can indeed precede visual field defects.3,4 They are especially helpful for early glaucoma diagnosis and in eyes with small optic disks. The localized wedge-shaped defect of the NFL is usually seen in association with notching of the neuroretinal rim, vertical enlargement of the cup, or following disk hemorrhages. Nevertheless, in early glaucoma, bundle defects in the NFL may not be associated with neuroretinal rim thinning because the initial damaged NFL is located in the deep retinal layers. Hence, typical wedge-shaped defects can be found in disks with normal appearance.5–7
Since NFL defects are not present in normal eyes, they always indicate an abnormality. Although typically occurring in about 20% of all eyes with glaucoma, they are not pathognomonic and can also be found in other ocular diseases, such as optic disk drusen, ischemic retinopathies with cotton-wool spots, toxoplasmotic retinochoroidal scars, long-standing papilledema, or optic neuritis due to multiple sclerosis. The incidence is higher in normal-tension glaucoma than in the other forms, which makes the differential diagnosis somewhat difficult.
Some authors have shown that NFL defects may be a common finding in diabetic patients with early diabetic retinopathy, and one of the risk factors is concomitant high blood pressure.8 Retinal nerve fiber layer thickness has been found to decrease with the development of diabetic retinopathy and with impairment of metabolic regulation.9 Cotton-wool spots are frequently a feature of systemic arteriolar disease, most commonly hypertension, diabetes, and collagen vascular disease; they represent infarcts at the nerve fiber layer. Cotton-wool spots have been described to be followed in some patients by localized NFL defects, with and without associated visual field defect.10,11
This case report describes a middle-aged patient with an isolated arcuate defect within the nerve fiber layer and visual field, without recognizable abnormality of the optic disk or cup. Although NFL raises suspicion for glaucoma and prompts a careful follow-up, other possible systemic reasons for localized retinal ischemia must also be considered.