



Female stress urinary incontinence (SUI) is being treated successfully with placement of tension-free vaginal tape.1 The use of synthetic mesh in renal transplant patients is rarely reported. No case of surgical treatment of SUI in a renal transplant patient using transobturator suburethral tape is listed on MEDLINE. The transobturator tape technique is a minimally invasive procedure that avoids the retropubic space by inserting a tension-free synthetic mesh underneath the middle of the urethra between the obturator foramens.2
DESCRIPTION OF THE CASEA 56-year-old female presented with stress urinary incontinence for 2 months. She complained about episodes of urinary leaks during coughing or physical exercise requiring the use of 1 to 3 pads per day with a severe impact on her quality of life. No dysuria, urgency, nocturia, or sensation of postvoid residual urine was reported. She had 3 vaginal deliveries, an appendectomy 40 years previously, and a renal transplantation in left iliac fossa 6 years previously to treat end-stage renal disease due to hypertension. At presentation, she was taking the following medications: mycophenolate mofetil 1500 mg/d, cyclosporin 150 mg/d, prednisone 7.5 mg/d, atenolol 100 mg/d, captopril 50 mg/d, and simvastatin 10 mg/d. The physical examination revealed a renal graft in left iliac fossa, trophic vaginal mucosa, and no pelvic organ prolapse. Urethral hypermobility was demonstrated with a positive Crystle test3, and urine loss was 40 g/24-hour measured using a pad weighing test. The urine culture was negative, and plasma creatinine was 0.9 mg/dL. Urodynamic evaluation showed a bladder capacity of 480 mL, normal compliance and sensation, absence of detrusor overactivity, Valsalva leak point pressure of 80 cm H2O, maximal flow rate of 9.3 mL/s, and detrusor pressure at maximal flow of 12.3 cm H2O.
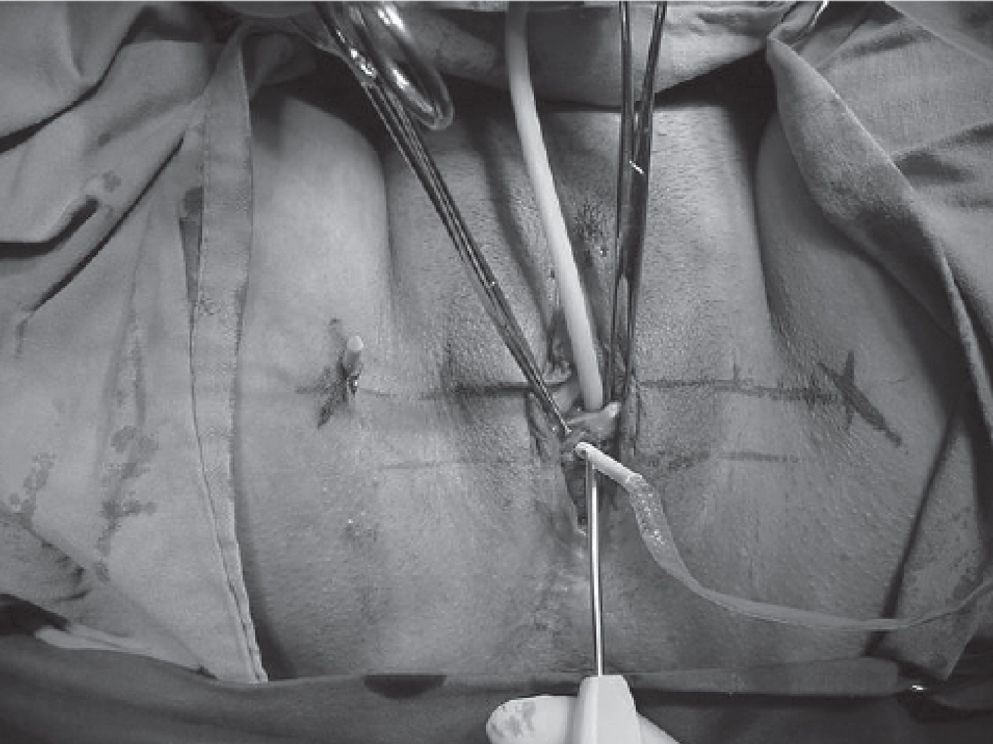
A tension-free polypropylene tape was inserted under regional anesthesia, and antibiotic prophylaxis with cefazolin at induction was used. The tape was inserted in a horizontal plane underneath the middle of the urethra between the obturator foramens via an inside-out technique4 (Figure 1) and was followed by cystoscopy to confirm absence of bladder injury. The procedure was uneventful and lasted 25 minutes, with an estimated blood loss of 20 mL. The patient was discharged the next day after spontaneous micturition. At a 30-day follow-up, no stress urinary incontinence, pads uses, or voiding difficulty was reported.

Transobturator needle insertion: inside-out technique4
The transobturator suburethral tape is a novel technique that is being applied for surgical treatment of SUI.2,5 There are no listed MEDLINE reports on this technique for a transplant patient. This approach prevents the risk of bladder, bowel, or vascular injuries because it avoids the retropubic space. Although we performed an endoscopic evaluation, there is no need for cystoscopy, which reduces operative time.2,5 Renal transplant patients particularly benefit from these advantages because the procedure avoids the theoretical risk of graft injury. No urinary or surgical site infection occurred in this case, despite the use of synthetic mesh in this immunosuppressed patient. Previous data on the use of synthetic material in transplant patients revealed low rates of infection.6 The inside-out transobturator technique for insertion of a suburethral tape is a good option for the treatment of SUI in renal transplant patients because of its minimally invasive character and low rates of complications.