


Physical activity and fitness play a significant role in prevention of overweight and obesity in children and adolescents. Current understanding and evidence from epidemiologic studies provide useful insights to better understand how they relate to each other and how to develop future intervention strategies. This paper summarizes the most relevant information from cross-sectional and longitudinal studies on the relationships between physical activity, physical fitness, and overweight in early life. According to current scientific evidence: (i) high levels of physical activity during childhood and adolescence, particularly vigorous physical activity, are associated to lower total and central adiposity at this age and later in life; (ii) the level of physical fitness, especially aerobic fitness, is inversely related to current and future adiposity levels; (iii) overweight children and adolescents with a high fitness level have a healthier cardiovascular profile than their overweight, low fit peers and a similar profile to their normal weight, low fit peers. This suggests that high fitness levels may counteract the negative consequences attributed to body fat. These findings suggest that increasing physical fitness in overweight children and adolescents may have many positive effects on health, including lower body fat levels.
Los niveles de actividad física y condición física desempeñan un papel fundamental en la prevención del sobrepeso y la obesidad durante la infancia y la adolescencia. De cara a un adecuado diseño de programas de prevención del sobrepeso y la obesidad, es necesario analizar la evidencia científica actualmente disponible, en particular la procedente de estudios epidemiológicos. El presente trabajo sintetiza la información científica más relevante procedente tanto de estudios transversales como longitudinales con relación a la actividad física, la condición física y el sobrepeso u obesidad durante las primeras etapas de la vida. La evidencia científica actual sostiene que: (i) niveles elevados de actividad física en la infancia o la adolescencia, especialmente de actividad física de alta intensidad, se asocian con una menor cantidad de grasa corporal total y troncular, y no solo durante estas etapas de la vida sino también en el futuro; (ii) el nivel de condición física en niños y adolescentes, especialmente la capacidad aeróbica, se relaciona inversamente con los niveles de grasa corporal que presentan en ese momento y también con los que presentan años después en la vida adulta; (iii) además, los niños y adolescentes con sobrepeso, pero que poseen un buen nivel de condición física, presentan un perfil de riesgo cardiovascular más saludable que sus compañeros con sobrepeso pero con mala condición física, y similar al que tienen sus compañeros de peso normal y baja condición física. Estos resultados sugieren que incrementar el nivel de forma física en niños y adolescentes con sobrepeso podría tener efectos beneficiosos presentes y futuros en diferentes indicadores del estado de salud, incluida la cantidad de grasa corporal.
Childhood and adolescence are very important life periods where multiple physiological changes occur. During adolescence, and in a relatively short time period, children almost double their body weight and reach complete sexual development, both of which affect body composition. In addition, this stage is also characterized by significant psychological changes. Both physiological and psychological changes influence behavior and lifestyle in the short and long term. Habits starting in adolescence like smoking, drinking alcohol, eating fruit and vegetables or doing exercise usually persist for a long time and are difficult to change in any case. Thus, if the acquired habit is unhealthy, a high level of awareness and motivation is required to modify it at a later time.
In contemporary society, overweight and obesity represent health problems of prime importance which affect not only adults, but also children and adolescents. Increased calorie intake combined with decreased calorie expenditure unavoidably leads to body fat accumulation in the mid or long term. The consequences for health of excess body fat are well known. Overweight or obesity in childhood or adolescence is strongly associated with overweight or obesity in adulthood. Specifically, overweight children/adolescents have a fivefold greater risk of being overweight in adulthood as compared to their normal-weight peers.1,2 It has also been shown that being overweight at an early age increases the risk of suffering cardiovascular disease in the future.3
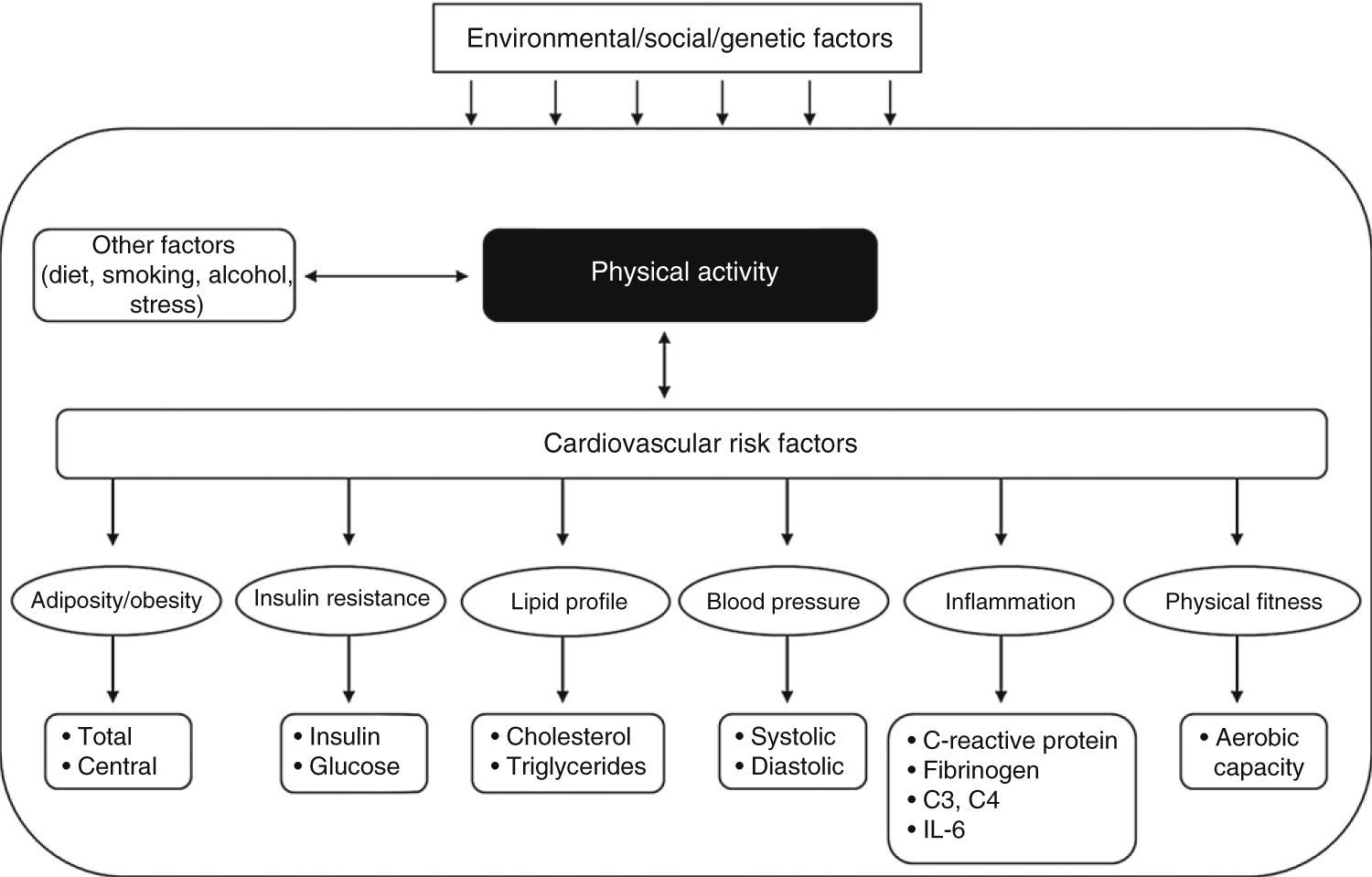
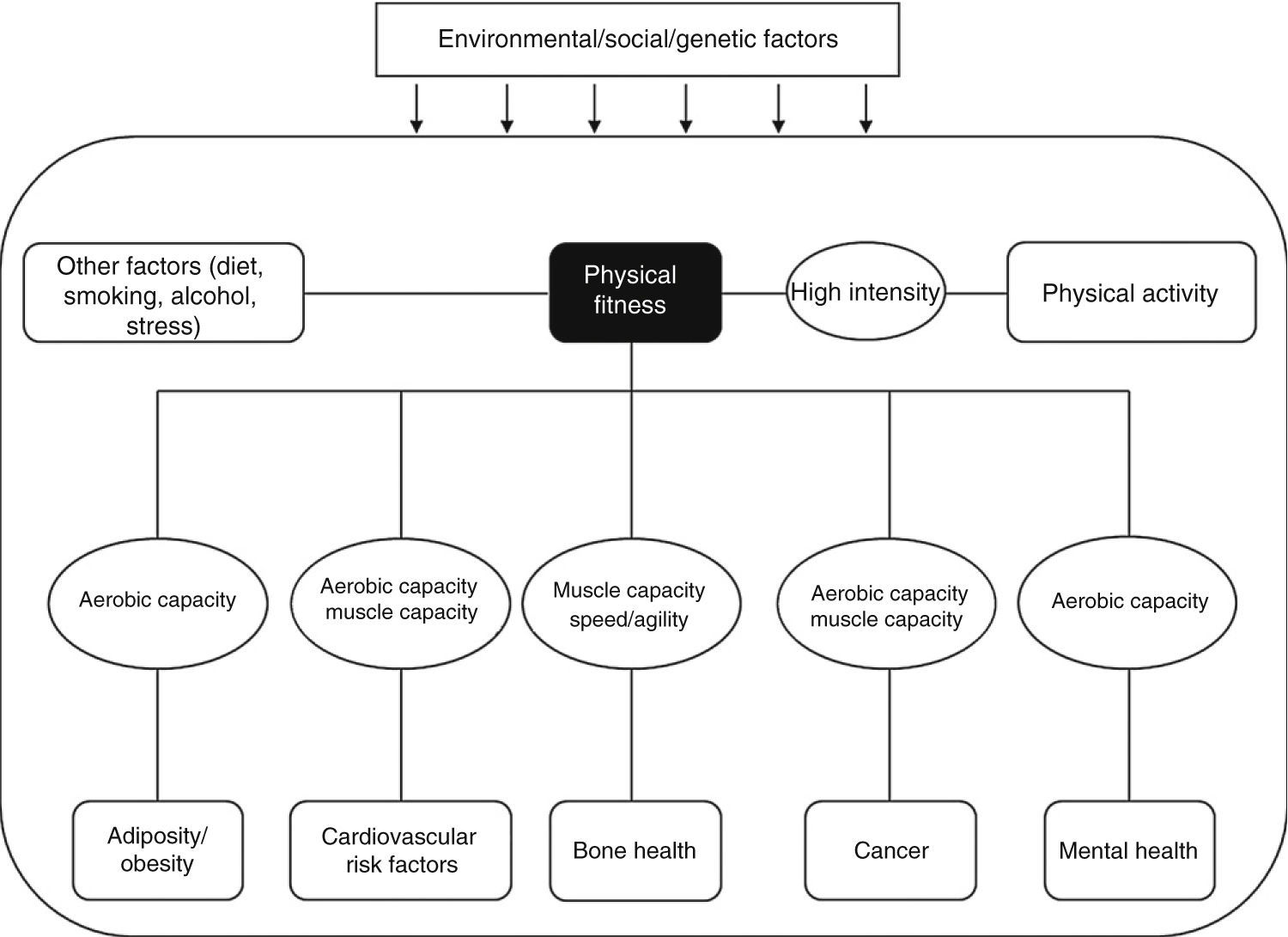
Physical activity (Fig. 1)4 and physical fitness (Fig. 2)5 levels are related to many parameters indicating the state of health, including body fat. The promotion and increase of physical activity levels, on the one hand, and/or improvement in physical fitness, on the other hand, may play an essential role in the prevention of overweight and obesity not only during childhood and adolescence, but also years later. Critical analysis of the current state of knowledge and of the available evidence from epidemiological studies is therefore required in order to adequately design prevention programs which can be implemented. This paper intends to summarize the scientific information available from cross-sectional and longitudinal studies about the relationship between physical activity, physical fitness, and overweight or obesity during early life stages.
 about the relationship between physical activity and various health parameters. C3: complement C3; C4: complement C4; IL-6: interleukin 6.")
Graphical representation of the information reviewed by Ruiz and Ortega 20094 (adapted and translated) about the relationship between physical activity and various health parameters. C3: complement C3; C4: complement C4; IL-6: interleukin 6.
 about the relationship between physical activity and various health parameters.")
Graphical representation of the information reviewed by Ortega et al., 20085 (adapted and translated) about the relationship between physical activity and various health parameters.
The term physical activity refers to any bodily motion that requires greater than basal energy expenditure. Assessment of the physical activity performed by a person under natural and real conditions is extremely difficult, particularly in children/adolescents. More than 30 different methods of assessing the physical activity of a person have been reported in the literature, and they may be summarized under three categories: (i) reference methods (direct observation, doubly labeled water, etc.); (ii) objective methods (heart rate monitoring, accelerometry, etc.); and (iii) subjective methods (surveys, questionnaires, etc.).4
Reference methods provide a very accurate measure of physical activity, but are very expensive and complicated, and it is therefore unfeasible to use them in population studies. Subjective methods are most commonly used in population studies because of their low cost; however, they are known to be poorly accurate for assessing physical activity levels, especially in young children (<12 years). Finally, among the objective methods available, motion sensors, also known as accelerometers, have been shown to be a feasible and valid method of obtaining helpful information about the duration, frequency, and intensity of physical activity performed by children and adolescents.
This review mainly focuses on studies which have objectively assessed physical activity using accelerometers. Most of the information available on the subject comes from cross-sectional studies using simple markers of body fat such as the body mass index (BMI).6 However, we will focus here on studies including more accurate total or central fat markers.
Cross-sectional studiesMost cross-sectional studies exploring the association between physical activity and body fat have shown an inverse association between them. Thus, a multicenter study conducted on 1292 European children7 (aged 9–10 years) and another study conducted on 251 Canadian children (aged 8–11 years)8 noted that the time devoted to moderate or vigorous physical activity was inversely related to the amount of total body fat (measured as the sum of skinfolds).
Various studies suggest that vigorous physical activity may play a leading role in the prevention of obesity in children and adolescents.4 Gutin et al.9 noted that only vigorous physical activity was associated with a lower amount of body fat in North American adolescents (16 years), which agrees with the results reported in younger individuals.10–12 Dencker et al.11 in a sample of Swedish children (aged 8–11 years), and Butte et al.13 in a sample of Hispanic children/adolescents living in the USA (aged 4–19 years), also noted a negative association between vigorous physical activity and body fat. The results recorded by our group in Estonian and Swedish children aged 9–10 years participating in the European Youth Heart Study (EYHS) support the previously discussed results.12 This latter study showed that children who performed vigorous activity for 40min or longer had less body fat than those performing vigorous activity for a total of 10 to 18min daily. One of the most relevant studies conducted to date on this subject was the Avon Longitudinal Study of Parents and Children, where 5500 children aged 12 years were assessed using dual X-ray absorptiometry (DXA).14 The authors found an inverse relationship between physical activity and adiposity, which became even more noticeable in boys as compared to girls. They similarly showed that the amount of body fat was more strongly associated with vigorous physical activity than with total physical activity accumulated during the day. Our group recently studied the relationship between objectively measured physical activity (using accelerometers) and total body fat measured by reference (DXA and BodPod) and anthropometric methods in Spanish adolescents aged 12.5–17.5 years who participated in the Healthy Lifestyle in Europe by Nutrition in Adolescence study (HELENA, www.helenastudy.com).15 The results showed that vigorous physical activity appears to have a greater effect on total and central fat than less intense physical activity, which agrees with the results of the previously discussed studies.
Based on a joint assessment of the above reported studies, it may be concluded that adequate scientific evidence is available to state that an inverse relationship exists between physical activity level and body fat, and that this association is more consistent when vigorous (as compared to less intense, i.e. moderate) physical activity is performed. It should however be noted that assuming the same duration, high intensity physical exercise involves a greater calorie expenditure than moderate exercise. It is currently unknown whether the effect on fat seen with high intensity as compared to moderate intensity activities is due to effort intensity itself or simply to the greater calorie expenditure associated with such activity. Strictly speaking, this issue can only be solved by duly controlled and designed intervention studies which measure the effects of two types of activity of different intensity and duration but similar calorie expenditure.
Regardless of the total amount of fat mass of a person, its distribution in the body is also relevant for health. Several studies have shown that abdominal fat, measured by waist circumference, is associated with a significant number of cardiovascular disease risk factors in adolescents,16 even for a given weight category (normal weight, overweight, or obesity).17 Although accurate and sophisticated methods are now available for assessing central or abdominal fat (e.g. magnetic resonance imaging, computed tomography, DXA, etc.), waist perimeter has been shown to be a good marker of truncal fat and has been widely used in many epidemiological studies because of it low cost and easy measurement.18
Our group studied a sample of Swedish children (9 years) and adolescents (15 years) and noted that those showing low levels (first tertile) of vigorous physical activity had a greater risk of having a waist circumference suggesting higher cardiovascular risk as compared to those showing high levels of vigorous physical activity (third tertile).19 These results agree with data from more recent studies showing a negative association between physical activity, especially vigorous physical activity, and central fat.20–22 By contrast, conflicting results were found when physical activity was assessed using questionnaires. In Spanish adolescents (aged 13–18.5 years) participating in the study Alimentación y Valoración del Estado Nutricional en Adolescentes (AVENA), no association was seen between physical activity and waist circumference,23 while another study reported an inverse association in 12-year-old French children.24
It has been suggested that the level of physical fitness of a child, adolescent, or adult may influence the potential effect of physical activity on various health parameters. This hypothesis was initially analyzed by us in relation to truncal fat, measured using waist circumference, in 1075 Swedish children and adolescents.25 The results suggest that the association between physical activity and truncal fat varies depending on aerobic capacity (a marker of physical fitness level). In subjects with poor physical fitness, an inverse relationship was seen between physical activity and truncal fat. Moreover, the relationship became positive when analyzed in subjects with a good level of physical fitness. We are currently replicating this study in a cohort of European adolescents who participated in the HELENA study in order to confirm or refute these results and thus better understand the role played by this relationship in the achieving of physical fitness.
Longitudinal studiesInformation from longitudinal studies using objective measures of physical activity in children/adolescents is scarce but consistent. A recent systematic review on this subject suggested that an inverse relationship exists between physical activity levels at a given time in childhood and fat contents in the future (follow-up time ranging from ∼2 to 15 years).6 The BMI was the anthropometric variable used in most studies, and only two of them included the measurement of total body fat based on skinfold measurements and/or bioelectric impedanciometry.
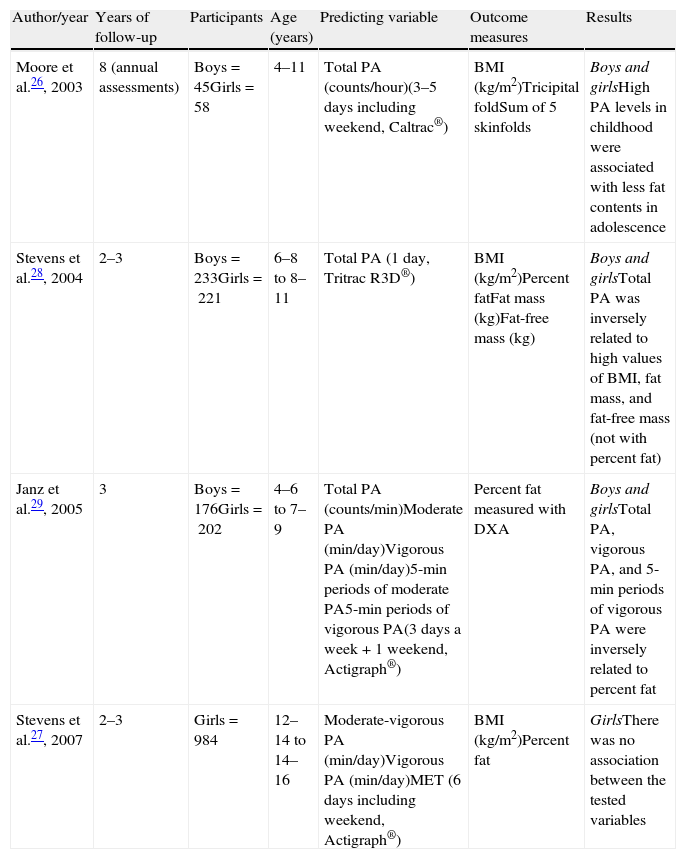
Four studies explored longitudinal relations between physical activity measured by accelerometry and total body fat (Table 1).26–29 Three of the four studies mentioned noted an inverse relation between physical activity level and future body fat. Special mention should be made of the Janz et al. study, which assessed the time devoted to physical activities of different intensities and percent fat, measured by DXA, in 378 children (aged 4–6 years).29 The results supported those found in cross-sectional studies, i.e. that vigorous, but not moderate, physical activity was associated with lower body fat levels three years later.
Longitudinal studies analyzing the relationship between physical activity in childhood/adolescence and future adiposity.
| Author/year | Years of follow-up | Participants | Age (years) | Predicting variable | Outcome measures | Results |
| Moore et al.26, 2003 | 8 (annual assessments) | Boys=45Girls=58 | 4–11 | Total PA (counts/hour)(3–5 days including weekend, Caltrac®) | BMI (kg/m2)Tricipital foldSum of 5 skinfolds | Boys and girlsHigh PA levels in childhood were associated with less fat contents in adolescence |
| Stevens et al.28, 2004 | 2–3 | Boys=233Girls=221 | 6–8 to 8–11 | Total PA (1 day, Tritrac R3D®) | BMI (kg/m2)Percent fatFat mass (kg)Fat-free mass (kg) | Boys and girlsTotal PA was inversely related to high values of BMI, fat mass, and fat-free mass (not with percent fat) |
| Janz et al.29, 2005 | 3 | Boys=176Girls=202 | 4–6 to 7–9 | Total PA (counts/min)Moderate PA (min/day)Vigorous PA (min/day)5-min periods of moderate PA5-min periods of vigorous PA(3 days a week+1 weekend, Actigraph®) | Percent fat measured with DXA | Boys and girlsTotal PA, vigorous PA, and 5-min periods of vigorous PA were inversely related to percent fat |
| Stevens et al.27, 2007 | 2–3 | Girls=984 | 12–14 to 14–16 | Moderate-vigorous PA (min/day)Vigorous PA (min/day)MET (6 days including weekend, Actigraph®) | BMI (kg/m2)Percent fat | GirlsThere was no association between the tested variables |
PA: physical activity; DXA: dual X-ray absorptiometry; BMI, body mass index; MET: metabolic equivalents.
No longitudinal studies have been found exploring the long-term effect of objectively measured physical activity on central fat in children and adolescents. Future research to study this subject in greater depth is needed.
Physical fitness and adiposityThe physical fitness of a person is a factor closely linked to the level of physical activity and/or exercise performed. Physical fitness is defined as the ability of a person to perform physical activity and/or exercise, and represents an integrated measure of all the functions and structures involved in the practice of physical activity or exercise. These include the musculoskeletal, cardiorespiratory, hematocirculatory, endocrinometabolic, and psychoneurological functions. A high physical fitness level implies a good coordinated and physiological response of all of these functions. By contrast, a poor level of physical fitness may suggest the malfunctioning of one or more of them.
Physical fitness comprises a set of physical qualities such as aerobic capacity, muscle strength and resistance, joint mobility, speed of movement, agility, coordination, and balance. Some authors also include body composition as an additional component of physical fitness. The measurement of these physical qualities in epidemiological studies is relatively recent, and its use in the field of health has been termed health-related fitness. Among all the qualities forming physical fitness, aerobic capacity and muscle strength have acquired the greatest scientific relevance in this field.
Physical fitness may be evaluated by different tests depending on the quality to be assessed. The standard test that best allows for measuring maximal aerobic capacity (also known as maximal oxygen consumption) of a person is a maximum effort test. In young people, the field test most widely used to estimate aerobic capacity is the 20-m shuttle run test, also known as the Course Navette or multi-stage fitness test.30 Muscle strength has traditionally been assessed using the hand grip strength test (upper body) and the standing broad jump test (lower body).31 Our group performed several methodological studies in young people and systematic reviews suggesting that these tests: (i) are indicative of the state of health in adulthood32; (ii) measure what they are intended to measure (are valid)33; (iii) are reliable, i.e. the result is consistent when evaluation is made several times34; and (iv) are simple to perform, inexpensive, and practical for use in population studies and in the school setting.31
Cross-sectional studiesRecent research has demonstrated the amount of interest there now is in knowing the physical fitness of children and/or adolescents.5,32 The results of the EYHS study showed that even in healthy children aged 9–10 years, those who had greater aerobic capacity also had lower levels of total adiposity as measured based on skinfolds.5,32 Our group also showed an inverse relationship between aerobic capacity and waist circumference in Swedish children and adolescents participating in the same study.25 Data from the AVENA study also suggested that aerobic capacity was associated with waist circumference in Spanish adolescents.25
These data agree with those from other studies where body fat was assessed using more sophisticated techniques.5 In line with this, we examined the relationship between physical fitness (i.e. aerobic capacity and muscle strength) and total and central body fat measured by DXA in Spanish adolescents participating in the HELENA study. The results showed that both aerobic capacity and muscle strength in the upper body were inversely associated with all body fat parameters after adjusting for different confounding variables, including objectively measured physical fitness.35 In this regard, Ara et al.36 reported very similar results in a sample of prepubertal Spanish children (∼9 years). Winsley et al.37 measured central fat by magnetic resonance imaging and noted that children with greater physical fitness levels also had lower truncal fat levels.
The role of muscle strength in the practice of exercise and the activities of daily life, and in the prevention of various diseases, has been paid increasing attention in recent years.31,32 The inverse relationship between the muscle strength of the lower body and body fat seen in the HELENA study agrees with the results obtained in the AVENA38 and other studies.39,40
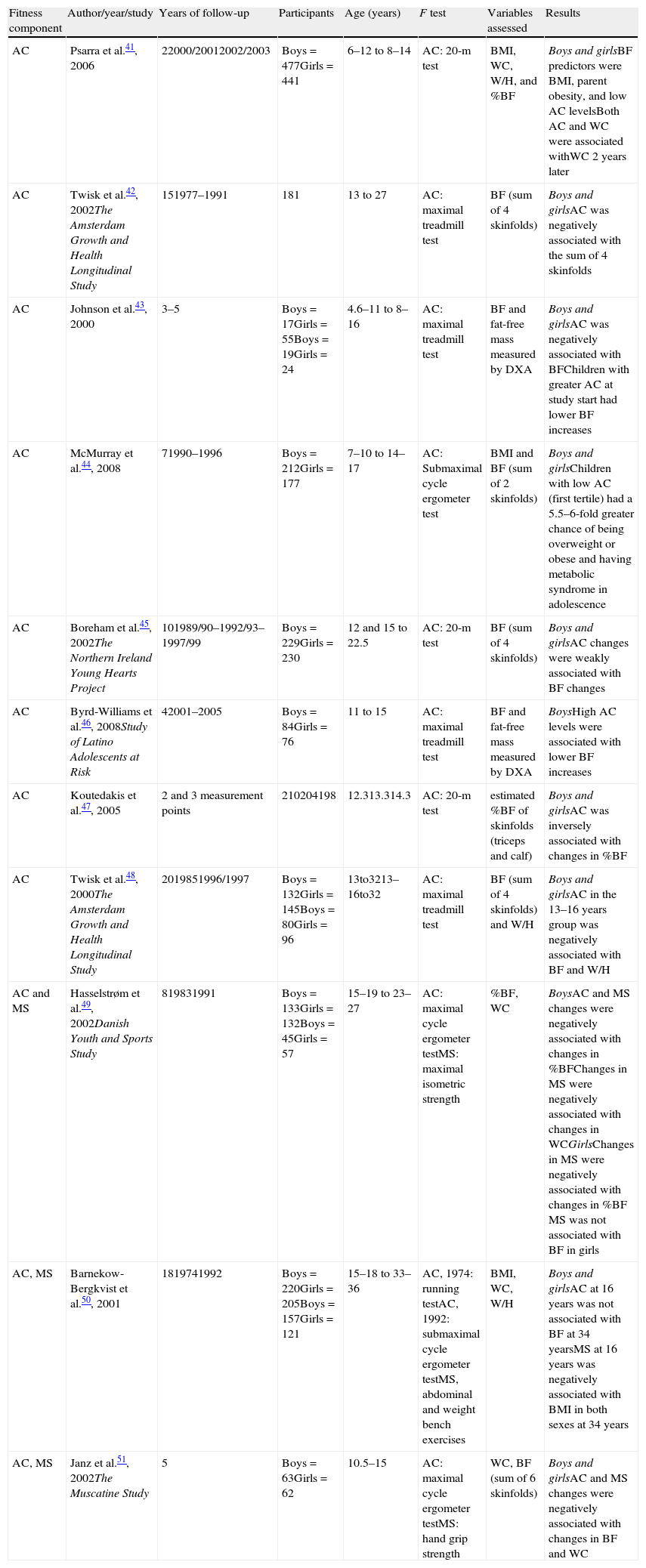
Longitudinal studiesSeveral studies have shown that aerobic capacity in childhood and adolescence predicts for total and central adiposity of a person years later, and also in adulthood (Table 2).41–51 The Amsterdam Growth and Health Longitudinal Study was one of the pioneering studies providing additional information concerning the longitudinal associations between physical fitness in childhood/adolescence and health parameters in adulthood. In this regard, Twisk et al.48 analyzed the association between the aerobic capacity of adolescents aged 13–16 years and their body fat at the age of 32 years. The results showed that adolescents with higher aerobic capacity levels also had lower levels of total body fat (the sum of four skinfolds) and truncal fat (waist to hip ratio) at 32 years of age.
Longitudinal studies analyzing the relationship between physical fitness in childhood/adolescence and future adiposity.
| Fitness component | Author/year/study | Years of follow-up | Participants | Age (years) | F test | Variables assessed | Results |
| AC | Psarra et al.41, 2006 | 22000/20012002/2003 | Boys=477Girls=441 | 6–12 to 8–14 | AC: 20-m test | BMI, WC, W/H, and %BF | Boys and girlsBF predictors were BMI, parent obesity, and low AC levelsBoth AC and WC were associated withWC 2 years later |
| AC | Twisk et al.42, 2002The Amsterdam Growth and Health Longitudinal Study | 151977–1991 | 181 | 13 to 27 | AC: maximal treadmill test | BF (sum of 4 skinfolds) | Boys and girlsAC was negatively associated with the sum of 4 skinfolds |
| AC | Johnson et al.43, 2000 | 3–5 | Boys=17Girls=55Boys=19Girls=24 | 4.6–11 to 8–16 | AC: maximal treadmill test | BF and fat-free mass measured by DXA | Boys and girlsAC was negatively associated with BFChildren with greater AC at study start had lower BF increases |
| AC | McMurray et al.44, 2008 | 71990–1996 | Boys=212Girls=177 | 7–10 to 14–17 | AC: Submaximal cycle ergometer test | BMI and BF (sum of 2 skinfolds) | Boys and girlsChildren with low AC (first tertile) had a 5.5–6-fold greater chance of being overweight or obese and having metabolic syndrome in adolescence |
| AC | Boreham et al.45, 2002The Northern Ireland Young Hearts Project | 101989/90–1992/93–1997/99 | Boys=229Girls=230 | 12 and 15 to 22.5 | AC: 20-m test | BF (sum of 4 skinfolds) | Boys and girlsAC changes were weakly associated with BF changes |
| AC | Byrd-Williams et al.46, 2008Study of Latino Adolescents at Risk | 42001–2005 | Boys=84Girls=76 | 11 to 15 | AC: maximal treadmill test | BF and fat-free mass measured by DXA | BoysHigh AC levels were associated with lower BF increases |
| AC | Koutedakis et al.47, 2005 | 2 and 3 measurement points | 210204198 | 12.313.314.3 | AC: 20-m test | estimated %BF of skinfolds (triceps and calf) | Boys and girlsAC was inversely associated with changes in %BF |
| AC | Twisk et al.48, 2000The Amsterdam Growth and Health Longitudinal Study | 2019851996/1997 | Boys=132Girls=145Boys=80Girls=96 | 13to3213–16to32 | AC: maximal treadmill test | BF (sum of 4 skinfolds) and W/H | Boys and girlsAC in the 13–16 years group was negatively associated with BF and W/H |
| AC and MS | Hasselstrøm et al.49, 2002Danish Youth and Sports Study | 819831991 | Boys=133Girls=132Boys=45Girls=57 | 15–19 to 23–27 | AC: maximal cycle ergometer testMS: maximal isometric strength | %BF, WC | BoysAC and MS changes were negatively associated with changes in %BFChanges in MS were negatively associated with changes in WCGirlsChanges in MS were negatively associated with changes in %BF MS was not associated with BF in girls |
| AC, MS | Barnekow-Bergkvist et al.50, 2001 | 1819741992 | Boys=220Girls=205Boys=157Girls=121 | 15–18 to 33–36 | AC, 1974: running testAC, 1992: submaximal cycle ergometer testMS, abdominal and weight bench exercises | BMI, WC, W/H | Boys and girlsAC at 16 years was not associated with BF at 34 yearsMS at 16 years was negatively associated with BMI in both sexes at 34 years |
| AC, MS | Janz et al.51, 2002The Muscatine Study | 5 | Boys=63Girls=62 | 10.5–15 | AC: maximal cycle ergometer testMS: hand grip strength | WC, BF (sum of 6 skinfolds) | Boys and girlsAC and MS changes were negatively associated with changes in BF and WC |
W/H: waist/hip ratio; AC: aerobic capacity; WC: waist circumference; F: fitness; DXA: dual X-ray absorptiometry; MS: muscle strength; BF: body fat; BMI: body mass index.
Data from longitudinal studies with less years of follow-up show very similar results. McMurray et al.44 conducted a seven-year longitudinal study and noted that children (aged 7–10 years) with low aerobic capacity (first tertile) had a 5.5–6-fold greater chance of having overweight and obesity, as well as metabolic syndrome, at adolescence (14–17 years) as compared to the group having better physical fitness levels. Byrd-Williams et al.46 similarly found in a four-year longitudinal study (Study of Latino Adolescents at Risk) that children aged 11 years with greater physical fitness levels had a lower increase in total body fat measured by DXA at 15 years.
Three longitudinal studies analyzed the relationship between muscle strength and total and central body fat.49–51 Barnekow-Bergkvist et al.50 measured muscle strength in adolescents aged 15–18 years and the BMI, waist circumference, and waist-hip ratio 18 years later. The results suggested that muscle strength predicted BMI in males and females at 34 years, so that those who had greater muscle strength levels in adolescence had lower BMI values at 34 years. However, the results for the central fat markers were not so clear. Janz et al.51 (The Muscatine Study) and Hasselstrøm et al.49 (Danish Youth and Sports Study) analyzed the relationship between changes in muscle strength and body fat parameters over several years. Both studies concluded that changes in muscle strength from childhood to adolescence (10–15 years)51 or from adolescence to adulthood (15–19 to 23–27 years)49 were negatively related to total body fat levels (measured by skinfolds) and waist circumference. Twisk et al.48 calculated a physical fitness index including measurements of muscle strength, flexibility, speed, and coordination. The results showed a negative relationship between the physical fitness index and mean total body fat measured by the sum of four subcutaneous skinfolds.
Children with overweight/obesity but fit (“fat but fit”)The prestigious group of Professor Blair was the first to note that people overweight or obese who had acceptably high physical fitness levels could have a better state of health than those who had the same level of overweight but poorer physical fitness. In fact, people rated as “fat but fit” (with excess fat but fit) had a similar cardiovascular risk profile as those with a normal weight for their age and sex but who had low physical fitness levels.
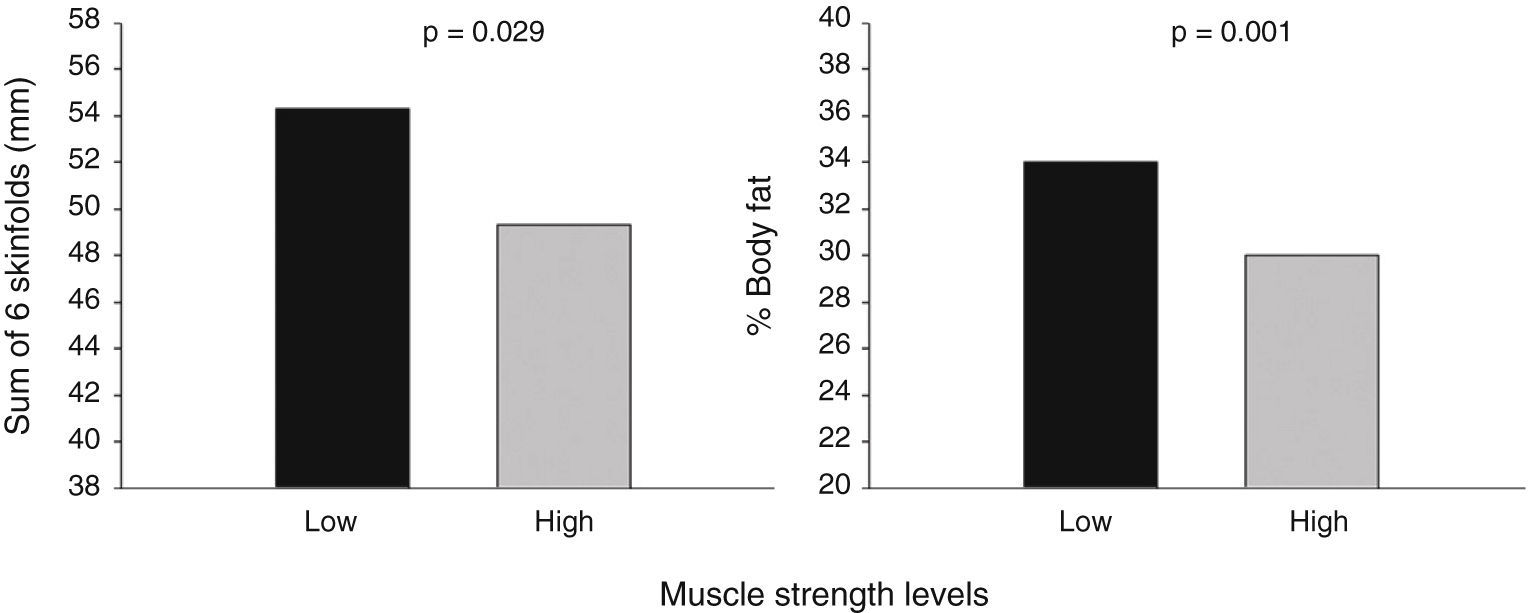
Our group conducted several studies in children and adolescents using data derived from the AVENA and EYHS cohorts and noted that adolescents with overweight and high muscle strength levels (third tertile) had lower body mass levels (the sum of six skinfolds) as compared to the group with overweight and low muscle strength levels (first tertile) (Fig. 3).52 Similarly, children with high body fat levels were found, as expected, to have a poorer lipid profile,53 higher blood pressure levels,54 and insulin resistance.55 However, these cardiovascular health parameters were attenuated in the group also having high aerobic capacity. This suggests that an improved aerobic capacity may counteract the negative effects of body fat on cardiovascular health parameters. Physical exercise programs aimed at improving physical fitness in children and adolescents with overweight and/or obesity may therefore be of great social, economic, and health interest.
 or high (third tertile) muscle strength levels (hand grip strength index and the standing broad jump test). Adapted from Ruiz et al.52")
Body fat in adolescents with overweight-obesity and low (first tertile) or high (third tertile) muscle strength levels (hand grip strength index and the standing broad jump test). Adapted from Ruiz et al.52
Our group recently investigated the minimal physical activity level associated with a lower risk of overweight or obesity in adolescents.56 After testing different physical activity levels in terms of duration and intensity, the results suggested that the currently recommended physical activity levels, at least 60min daily of moderate to vigorous activity, appear to be sufficient to prevent overweight or obesity. However, the results showed that accumulating a minimum of vigorous physical activity, i.e. 15min daily, has additional benefits for the prevention of overweight or obesity.56
As regards physical fitness, it has been noted that having an aerobic capacity, expressed as maximal oxygen consumption, greater than 42mL/kg/min in boys and 35–37mL/kg/min in girls is associated with a lower risk of overweight/obesity and metabolic risk.23,57–59 In this setting, our group studied a cohort of Swedish and Estonian children from 9 to 15 years of age (six years of follow-up).60 Only children with normal baseline weight were selected, and the factors causing these children to develop overweight and obesity six years later were analyzed. It was noted that, regardless of the BMI or physical fitness at baseline, those adolescents who improved their aerobic capacity (estimated maximal oxygen consumption) significantly decreased the risk of developing overweight or obesity.60 These data suggest that the promotion of physical activity and improvements in physical fitness are important tools for the prevention of overweight and obesity in children.
ConclusionsThe scientific evidence from cross-sectional and longitudinal studies suggests that:
- (i)
High physical activity levels in childhood or adolescence, particularly vigorous physical activity, are associated with a lower amount of both total and truncal body fat both at that time and in the future.
- (ii)
The level of physical fitness in children and adolescents, especially aerobic capacity, is inversely related to current and future body fat levels.
- (iii)
Overweight children and adolescents with a good level of physical fitness have a healthier metabolic and cardiovascular profile than their overweight, low fit peers and a similar profile to their normal weight, low fit peers.
These results demonstrate the urgent need for promoting a more active lifestyle in all subjects, regardless of their age and condition. The objective is not only to fight sedentary lifestyles and increase calorie expenditure by increasing physical activity, but also to ensure that such physical activity is vigorous enough to improve physical fitness. Such vigorous activity not only improves the calorie expenditure associated with exercise, but also increases, or at least preserves, muscle mass, thus increasing basal calorie expenditure also. On the other hand, improved physical fitness, apart from its effect on energy metabolism, also has various effects on promoting health and decreasing the risk of suffering from various diseases, many of them associated with obesity, and which are currently among the most prevalent in the population.
The effort required for such an improvement goes beyond the patients themselves to involve also their family and school, which should provide a favorable setting for performing vigorous physical activity. The healthcare system is also involved, since it can make use of the various currently available technologies, which allow for the simple and reliable assessment of the physical activity performed by a subject, regarding not only its type, but also its intensity and duration, and for ascertaining the physical fitness of the subject and how this correlates with other health parameters and markers, including body composition, and how one and the other evolve over time. All of this will undoubtedly have a positive impact on the current and future health and well-being of the patient him/herself and, by extension, on the whole population.
Conflicts of interestThe authors state that they have no conflicts of interest.
Please cite this article as: Ortega FB, Ruiz JR, Castillo MJ. Actividad física, condición física y sobrepeso en niños y adolescentes: evidencia procedente de estudios epidemiológicos. Endocrinol Nutr. 2013;60:458–469.
