



The use of reusable semi-critical devices has been extended in current medical practice for both diagnostic and therapeutic purposes. However, reuse of these instruments carries the risk of cross-transmission of microorganisms from one patient to another. The process of cleaning and disinfecting these devices is complex, long, expensive and very error-prone. This paper analyses the epidemiological aspects of infections associated with the reuse of semi-critical devices and the role of the Microbiology laboratory in monitoring the cleaning and disinfecting process through microbiological controls. The recommendations of different scientific societies on the relevance of such controls are reviewed and specific recommendations are proposed for the taking and processing of the samples, interpretation of the results and measures to be taken depending on the results obtained.
El uso de los dispositivos semicríticos reutilizables se ha extendido en la práctica médica actual tanto con fines diagnósticos como terapéuticos. Sin embargo, la reutilización de estos instrumentos conlleva el riesgo de una transmisión cruzada de microorganismos de un paciente a otro. El proceso de limpieza y desinfección de estos dispositivos es complejo, largo, caro y muy sensible a que se produzcan fallos. En el presente documento se analizan los aspectos epidemiológicos de las infecciones asociadas a la reutilización de los dispositivos semicríticos, y el papel del laboratorio de Microbiología en la monitorización del proceso de limpieza y desinfección de los mismos a través de los controles microbiológicos. Se revisan las recomendaciones de diferentes sociedades científicas sobre la pertinencia de dichos controles y se establecen recomendaciones específicas para la toma y el procesamiento de las muestras, la interpretación de los resultados y las medidas a tomar en función de los resultados obtenidos.
In current medical practice, a very wide variety of medical devices are used for both diagnostic and therapeutic purposes. In some cases, these devices may act as vehicles for transmission of infectious agents to a susceptible host, resulting in the development of a nosocomial or healthcare-associated infection.1–4 Not all medical devices behave the same way with respect to risk of infection, since this depends on the use for which they are designed.
Reusable devices classified by Spaulding5 as semi-critical are those that have most often been associated with the development of healthcare-associated infections. This category would include flexible endoscopes in general, defined as devices that access the inside of the body through natural orifices (gastroscopes, colonoscopes, fibrobronchoscopes and cystoscopes), endotracheal tubes, laryngoscopes and rectal thermometers.
For these devices to be reused, they must, between one patient and another, undergo a high-level disinfection process. In many cases, this process proves complicated, not only due to the structural complexity of the devices (long and narrow lumina, valves, etc.), but also because it is an inherently laborious process with different steps (mechanical cleaning, leak management, cleaning with enzymatic detergents, rinses, disinfection, drying and storage) that depend heavily on the proper training of the healthcare staff responsible for the reprocessing of the devices. This means that the process is vulnerable to not always being done correctly.2,6–8 In this context, regular microbiological controls may serve as a quality indicator ensuring that all the steps of the cleaning and disinfection process have been properly followed.8–11
Non-critical materials usually do not represent a risk of infection for patients and do not require microbiological controls. However, sometimes, in the context of epidemic outbreaks, sampling of these devices may be needed to locate the source and/or determine the presence of contaminated fomites representing a potential link in the chain of transmission of a particular microorganism. An example of this situation is the recently reported international outbreak of infection with Mycobacterium chimaera associated with the use of hot/cold devices to regulate the temperature of the blood and the cardioplegia solution during extracorporeal circulation in heart surgery procedures. In this regard, the European Centre for Disease Prevention and Control has published a technical document for laboratory detection of M. chimaera in these devices and in the environment.12
Clinical considerationsInfection associated with a diagnostic or therapeutic procedure in which any semicritical instrument has been used is infection detected after said procedure has been performed and related to it. In some cases, infection is a complication associated with the procedure itself as a result of dragging or transferring microorganisms from the patient from one place to another (endogenous source of infection). In other cases, a contaminated instrument acts as a vehicle for microorganism transmission (exogenous source of infection).
There are few well-designed prospective studies on the incidence of transmission of pathogens associated with the use of this type of device. In most of the cases documented in the literature, this transmission has occurred in relation to deficiencies in at least one of the steps of the cleaning and disinfection process. This highlights not only the high frequency with which these procedures are not performed properly, but also the limited surveillance that they undergo1,4,6 and, most worryingly, the persistent colonisation of some of these instruments despite their having been processed strictly in accordance with the recommendations.13
Most published cases have been in the context of outbreaks or pseudo-outbreaks caused by unusual or multidrug-resistant microorganisms that are easily detected as they are subject to surveillance in many cases.6,13,14 It seems likely that the problem is being underestimated and that cross-contamination with another, more common, type of microorganism may go unnoticed.2–4,7,8 In general, the microorganisms that in the medical literature have most often been associated with transmission through these devices are multidrug-resistant Gram-negative bacilli (Escherichia coli, Klebsiella pneumoniae, Pseudomonas aeruginosa, Serratia marcescens, etc.), mycobacteria and hepatitis B and C viruses.2,4,6
Clinical syndromesIn many cases, cross-transmission of microorganisms from one patient to another is not associated with the development of a clinical infection; instead, asymptomatic host colonisation occurs. In cases in which a symptomatic infection takes place, signs and symptoms vary widely. When cystoscopes are used, urinary infections tend to develop. These may or may not be associated with bacteraemia. When gastrointestinal endoscopes are used, bacteraemia, cholangitis, cholecystitis or hepatitis may be seen. Finally, when fibrobronchoscopes and ventilation equipment are used, pneumonia or bacteraemia may arise.
Pathogenic mechanismsThe mechanism by which cross-transmission of a microorganism occurs is instrument contamination. This may happen either through the microbiota of a patient who has previously undergone a procedure or through the inanimate environment (irrigation solutions, automatic washing devices, etc.). Contamination may persist in this type of instrument for different reasons: errors in the cleaning/disinfection process of the device, formation of biofilms or presence of structural abnormalities in the device (leaks) that make eradication of bacteria impossible even when cleaning protocols are properly applied.2,6
Role of microbiological controlsMicrobiological controls of reusable semi-critical devices are tools to detect failures in the cleaning and disinfection process and abnormalities in the surface of the device that promote the persistence of microorganisms.11 There is no unanimous consensus on either the need for controls or the methodology to be employed. However, different scientific associations recommend periodic cultures as part of the quality control of the disinfection process and give instructions on the process of sampling, processing of samples and interpretation of results.9,13,15–20 There is also no unanimous consensus with respect to the regularity of culturing. Different guidelines have recommended cultures on a monthly, quarterly or even annual basis.9,16,19,20
Collection of samples for microbiological cultureSampling requires sterile equipment (gloves, syringes, brushes and vessels). Samples must always be collected under conditions of maximum asepsis. The ideal time for sampling is after the process of disinfection and storage to assess whether contamination occurred during that process.
Channels of the endoscope: using sterile syringes, 10–20ml of sterile normal saline (0.9% NaCl) or sterile distilled water are instilled through each channel individually and collected from the distal part of the endoscope in a sterile vessel. Sample collection may include inserting a sterile brush into the channel, brushing the inside and then mixing it with 10ml of sterile normal saline (0.9% NaCl) or sterile distilled water in a sterile vessel.9
Outer surfaces of the endoscope: a sterile swab soaked in sterile normal saline (0.9% NaCl) is used to swab the different outer surfaces of the endoscope (distal end, channel opening points and elevator bridge). Each swab is collected in a sterile vessel with tryptic soy broth (TSB).
Bottle of water connected to the endoscope: 2 samples of 100ml of water are collected using a sterile syringe through the usual connector between the bottle and the endoscope and transferred to a sterile vessel.
Automatic washer disinfectors: 2 samples of 100ml of final rinse water should be collected in a sterile vessel (UNE EN-ISO 15883 standards).
Final rinse water: if automatic washer disinfectors are not used, 2 samples of 100ml of water should be taken with a sterile syringe.
Transport and storage of samplesSamples must be sent in sealed sterile vessels and labelled to indicate the sampling point and the ID of the endoscope or washer disinfector.
They should be processed immediately to prevent potential bacterial overgrowth altering the count in the quantitative culture. If processing is to be delayed, then samples must be stored refrigerated at 2–5°C for no more than 24h. In some cases, depending on the disinfectant product used, a neutralising agent may be added to remove potential traces of chemical agents which may limit detection of microorganisms.
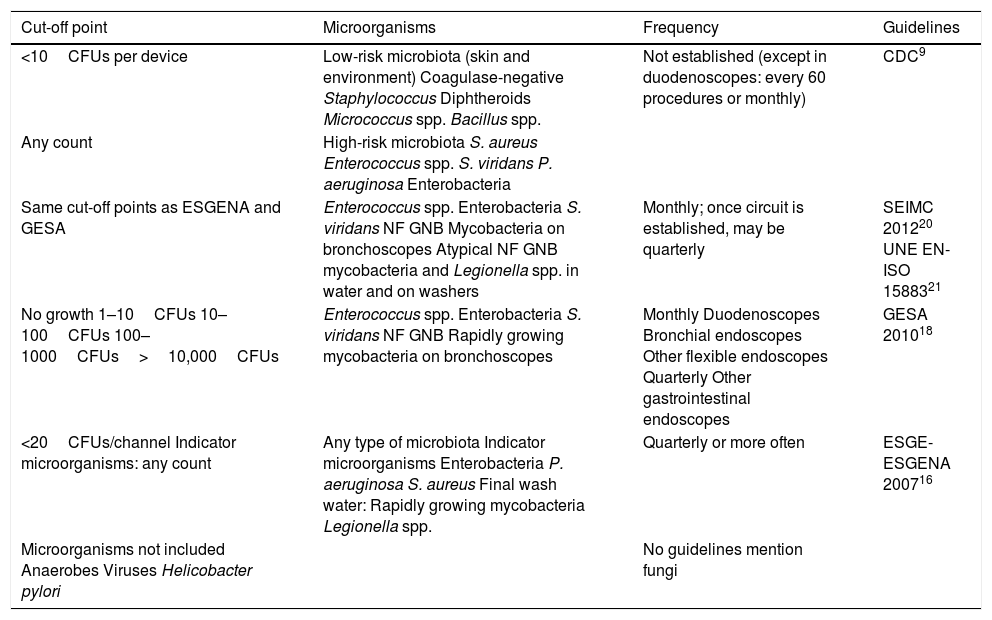
Handling and processing of samplesDifferent national and international associations9,16–21 have determined that microbiological culture of endoscopes in general (gastrointestinal endoscopes, cystoscopes and fibrobronchoscopes) should be aimed at finding microorganisms in the oral and enteric microbiota. Table 1 provides a detailed description of the microorganisms that act as indicators of an unsuitable cleaning and disinfection process. It is not advisable to attempt to detect viruses since detection of intact viruses with infectious capacity is a complex, high-cost process.
Recommendations for microbiological study of endoscopes.
| Cut-off point | Microorganisms | Frequency | Guidelines |
|---|---|---|---|
| <10CFUs per device | Low-risk microbiota (skin and environment) Coagulase-negative Staphylococcus Diphtheroids Micrococcus spp. Bacillus spp. | Not established (except in duodenoscopes: every 60 procedures or monthly) | CDC9 |
| Any count | High-risk microbiota S. aureus Enterococcus spp. S. viridans P. aeruginosa Enterobacteria | ||
| Same cut-off points as ESGENA and GESA | Enterococcus spp. Enterobacteria S. viridans NF GNB Mycobacteria on bronchoscopes Atypical NF GNB mycobacteria and Legionella spp. in water and on washers | Monthly; once circuit is established, may be quarterly | SEIMC 201220 UNE EN-ISO 1588321 |
| No growth 1–10CFUs 10–100CFUs 100–1000CFUs>10,000CFUs | Enterococcus spp. Enterobacteria S. viridans NF GNB Rapidly growing mycobacteria on bronchoscopes | Monthly Duodenoscopes Bronchial endoscopes Other flexible endoscopes Quarterly Other gastrointestinal endoscopes | GESA 201018 |
| <20CFUs/channel Indicator microorganisms: any count | Any type of microbiota Indicator microorganisms Enterobacteria P. aeruginosa S. aureus Final wash water: Rapidly growing mycobacteria Legionella spp. | Quarterly or more often | ESGE-ESGENA 200716 |
| Microorganisms not included Anaerobes Viruses Helicobacter pylori | No guidelines mention fungi |
CDC: Centres for Disease Control and Prevention; CFUs: colony-forming units; ESGE-ESGENA: European Society of Gastrointestinal Endoscopy-European Society of Gastroenterology and Endoscopy Nurses and Associates; GESA: Gastroenterological Society of Australia; NF GNB: non-fermenting Gram-negative bacilli; SEIMC: Spanish Association of Infectious Diseases and Clinical Microbiology.
Usually, it is not necessary to prepare antibiograms for all microorganisms isolated; however, in certain situations (potential outbreaks and repeated isolations of enterobacteria or P. aeruginosa), they may be useful to detect multidrug-resistant bacteria.
Selection of culture media and sample incubation conditionsSamples collected from the channels of the endoscope: this usually involves mixing or pooling all samples collected by washing and brushing the different channels of the endoscope and processing them as a single entity. However, if microbiological cultures are repeatedly positive for a particular endoscope, it may be necessary to process samples from different channels individually.
The recommended culture media9,16–20 are:
- -
Aerobic microorganisms: blood agar, tryptic soy agar (TSA), Reasoner's 2A-agar and TSB.
- -
Mycobacteria: Middlebrook 7H10 agar.
Samples may be processed using 2 techniques9,16–20:
- -
Direct inoculation: 1ml of sample is seeded in a blood agar or TSA plate.
- -
Concentration is done by means of centrifugation or filtration. Centrifugation is done for 15min at 3000rpm, the supernatant is decanted, the sediment is resuspended and 0.1ml is seeded in blood agar. For filtration, 10ml of sample are collected and passed through a filter with a pore diameter of no more than 0.45μm. The filter is incubated in TSA.
In both techniques, plates may be incubated at 30°C or 37°C for 48h or 7 days (check at 48h). For mycobacterial culture, plates are incubated at 37°C for 21 days.
Samples obtained from the outer surfaces of the endoscope: the swab is stirred in 10ml of TSB, stirred again using a vortex and incubated for 48h at 37°C. At 48h, subcultures are performed on selective media.
Rinse water from the automatic washer and water from the bottle connected to the endoscope: 100–200ml of sample are filtered using filters with a pore diameter of no more than 0.45μm and the filter is incubated in blood agar or Reasoner's 2A-agar at 30°C for 3–5 days or at 37°C for 2 days.9,10,16,18 If there are no filters available, it is possible to add 100ml of rinse water to 100ml of TSB and incubate at 37°C for 48h, then do a subculture on selective media; however, this methodology has not been validated. For mycobacterial culture, a specific medium such as Middlebrook 7H10 agar should be used and incubation should be done at 37°C for 21 days.
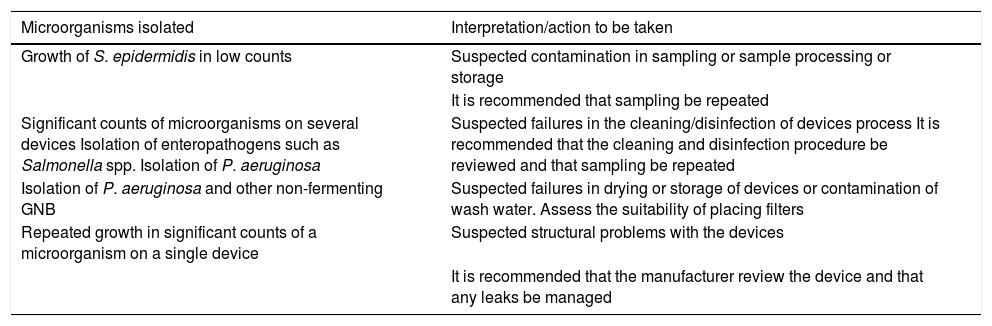
Criteria for interpretation of resultsTable 1 lists the types of microorganism to be sought and the minimum counts of colony-forming units to be considered significant. Table 2 describes the general interpretation of culture results and the recommended actions depending on them.
General interpretation of microbiological results.
| Microorganisms isolated | Interpretation/action to be taken |
|---|---|
| Growth of S. epidermidis in low counts | Suspected contamination in sampling or sample processing or storage |
| It is recommended that sampling be repeated | |
| Significant counts of microorganisms on several devices Isolation of enteropathogens such as Salmonella spp. Isolation of P. aeruginosa | Suspected failures in the cleaning/disinfection of devices process It is recommended that the cleaning and disinfection procedure be reviewed and that sampling be repeated |
| Isolation of P. aeruginosa and other non-fermenting GNB | Suspected failures in drying or storage of devices or contamination of wash water. Assess the suitability of placing filters |
| Repeated growth in significant counts of a microorganism on a single device | Suspected structural problems with the devices |
| It is recommended that the manufacturer review the device and that any leaks be managed |
The relevant department should be contacted and informed, and the team responsible for preventing and managing infections at the healthcare centre should be provided with a report. In addition, depending on the microorganism(s) detected and the inoculum, it must be recommended that suitable measures be carried out (resampling, review of the device and review of cleaning and disinfection procedures).
Any contaminated material should be removed from use until its microbiological controls yield the proper results. Should certain microorganisms such as P. aeruginosa, other non-fermenting Gram-negative bacilli, Salmonella spp. and Shigella spp. be isolated, a targeted follow-up of exposed patients must be done. This follow-up is also needed if Mycobacterium tuberculosis or Mycobacterium chelonae is isolated from bronchoscope samples. In recent years, cases of invasive cardiovascular disease due to M. chimaera associated with the use of hot/cold systems during extracorporeal circulation have been reported.22
The Microbiology laboratory should prepare a written statement with the results of the cultures as well as a report to the Commission for Infections/Patient Safety on the incident, the measures adopted and the resolution of the problem.
Other procedures to detect organic wasteOne of the main drawbacks of microbiological cultures as a tool to monitor the disinfection process of semi-critical devices is the delay in getting the results. Therefore, other techniques to detect organic waste quickly have been developed. The techniques currently available include measurement of ATP and waste from proteins, haemoglobin and carbohydrates.
ATP is a good marker to evaluate the presence of organic waste as this molecule is present in all live cells. Its presence is measured by bioluminescence. This involves using luciferase, an enzyme that makes use of ATP, and luciferin, a protein that generates a light signal that is measured in relative light units using a light metre. As there is a linear relationship between the amount of ATP and the amount of light, the more organic waste is present, the more ATP is present and the more light is produced. This technique may be used to measure contamination in real time of both surfaces and channels of endoscopes. Most published studies have evaluated this technique to measure the efficacy of the manual cleaning process prior to disinfection.11,17 High bioluminescence values following manual cleaning indicate that too much organic waste is present for the disinfection process to be effective.23 A benchmark value of 200 relative light units has been set under which an endoscope channel and surface may be deemed suitable following the manual cleaning process.23
Different commercial kits are available to detect proteins, haemoglobin and carbohydrates. These kits are based on easy-to-manage colorimetric reactions that provide results quickly. The cut-off points for acceptance after suitable cleaning and before disinfection are <6.4 for proteins, <1.2 for carbohydrates and <2.2mg/cm for haemoglobin, respectively.11,17
At present, no guidelines recommend using these biomarkers rather than microbiological cultures, since more studies are needed to validate them.9
Conflicts of interestThe authors declare that they have no conflicts of interest.
Please cite this article as: Blázquez-Garrido RM, Cuchí-Burgos E, Martín-Salas C, Ruiz-Garbajosa P. Métodos microbiológicos para la monitorización de la limpieza, desinfección y esterilización de dispositivos médicos. Enferm Infecc Microbiol Clin. 2018;36:657–661.
