




Brazil is one of the countries with the highest incidence and mortality rates from COVID-19 worldwide. In 2022, the country faced a third wave of the disease associated with community transmission of the Omicron variant. During the first 10 epidemiological weeks (January 2–March 12, 2022), 7,058,717 cases and 35,840 deaths from COVID-19 were recorded. In addition, Brazil has faced an out-of-season outbreak of influenza A virus (A/Darwin/6/2021(H3N2)), first detected in Rio de Janeiro in November 2021, and widely spread in the country in the first weeks of 2022. In most Brazilian states, the flu season usually occurs from May to July, starting in the Northeast region and spreading to the South.1 The simultaneous transmission of COVID-19 and influenza in 2022 resulted in a significant increase in demand for hospital beds, but the country's case-fatality rates associated with the most severe forms of these diseases during this period are unknown.
In this nationwide ecological study, we estimated the case-fatality rates and risk of death from COVID-19 and influenza A/H3N2. Brazil has a geographic area of ∼8.5 million square kilometers and a population of circa 213 million people. In addition, the country comprises 26 states and one federal administrative district and is divided into five regions: North (seven states), Northeast (nine states), Midwest (three states and one federal district), Southeast (four states), and South (three states). The human development index (HDI) is 0.765 and the poorest regions of the country are the North (HDI 0.730) and Northeast (HDI 0.715) regions.
We included all hospitalized patients with laboratory-confirmed SARS-CoV-2 or influenza A/H3N2 infection from January 2 to March 12, 2022. The number of cases and deaths by COVID-19 and influenza was obtained from the SIVEP-Gripe dataset (https://opendatasus.saude.gov.br/dataset/srag-2021-e-2022), which is a deidentified public domain database established by the Brazilian Ministry of Health for the surveillance of severe acute respiratory syndrome. Data on sex, age, race, and distribution by geographic region were described. Case-fatality rates were calculated based on the number of deaths divided by the total number of confirmed cases for each disease. Differences in case-fatality rates between diseases as age increased were analyzed by using the Cochran-Armitage test for trend. We also estimated the relative risk (RR) of death by comparing hospitalized patients with COVID-19 to those with influenza according to the variables of interest. The significance level was set as 0.05. Data were analyzed by using JASP software version 0.13 (JASP Team, Amsterdam, Netherlands).
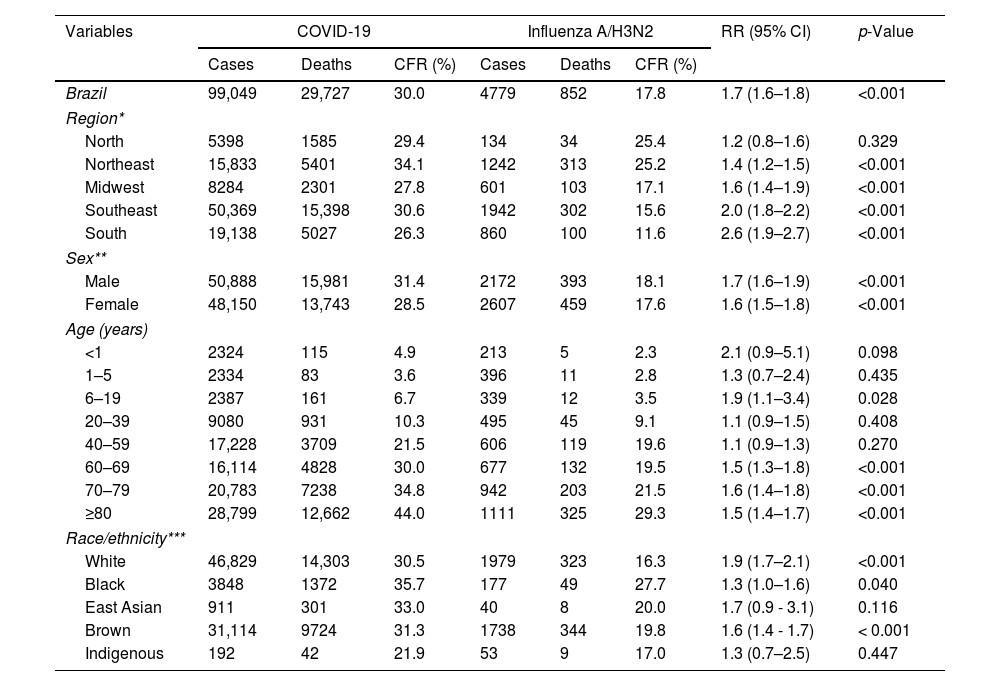
During the first 10 epidemiological weeks of 2022, 99,049 patients with COVID-19 and 4779 patients with influenza were hospitalized in Brazil. A total of 29,727 deaths associated with COVID-19 and 852 deaths from influenza were registered and the case-fatality rates were 30% and 17.8%, respectively. The highest lethality rates for both diseases were observed among men, Blacks, and people over 80 years of age. The Northeast and Southeast regions had the highest case-fatality rates for COVID-19, while the North and Northeast had the highest lethality for influenza (Table 1; Fig. 1 – Supplementary file). Furthermore, we found that differences in case-fatality rates between COVID-19 and influenza tend to increase with increasing age (p<0.001) (Fig. 2 – Supplementary file). The results of this study showed that hospitalized patients with COVID-19 had approximately two-fold increased risk of death compared to those hospitalized with influenza infection (RR=1.7; 95% CI 1.6–1.8; p<0.001). The risk of death from COVID-19 was higher than from influenza in all geographic regions of the country (except for the North region); in both sexes; white, black, or mixed race; and among those aged 6 to 19 years and over 60 years old (Table 1).
Case-fatality rates and risk of death among hospitalized patients with COVID-19 compared to hospitalized patients with influenza A/H3N2 infection in Brazil.
| Variables | COVID-19 | Influenza A/H3N2 | RR (95% CI) | p-Value | ||||
|---|---|---|---|---|---|---|---|---|
| Cases | Deaths | CFR (%) | Cases | Deaths | CFR (%) | |||
| Brazil | 99,049 | 29,727 | 30.0 | 4779 | 852 | 17.8 | 1.7 (1.6–1.8) | <0.001 |
| Region* | ||||||||
| North | 5398 | 1585 | 29.4 | 134 | 34 | 25.4 | 1.2 (0.8–1.6) | 0.329 |
| Northeast | 15,833 | 5401 | 34.1 | 1242 | 313 | 25.2 | 1.4 (1.2–1.5) | <0.001 |
| Midwest | 8284 | 2301 | 27.8 | 601 | 103 | 17.1 | 1.6 (1.4–1.9) | <0.001 |
| Southeast | 50,369 | 15,398 | 30.6 | 1942 | 302 | 15.6 | 2.0 (1.8–2.2) | <0.001 |
| South | 19,138 | 5027 | 26.3 | 860 | 100 | 11.6 | 2.6 (1.9–2.7) | <0.001 |
| Sex** | ||||||||
| Male | 50,888 | 15,981 | 31.4 | 2172 | 393 | 18.1 | 1.7 (1.6–1.9) | <0.001 |
| Female | 48,150 | 13,743 | 28.5 | 2607 | 459 | 17.6 | 1.6 (1.5–1.8) | <0.001 |
| Age (years) | ||||||||
| <1 | 2324 | 115 | 4.9 | 213 | 5 | 2.3 | 2.1 (0.9–5.1) | 0.098 |
| 1–5 | 2334 | 83 | 3.6 | 396 | 11 | 2.8 | 1.3 (0.7–2.4) | 0.435 |
| 6–19 | 2387 | 161 | 6.7 | 339 | 12 | 3.5 | 1.9 (1.1–3.4) | 0.028 |
| 20–39 | 9080 | 931 | 10.3 | 495 | 45 | 9.1 | 1.1 (0.9–1.5) | 0.408 |
| 40–59 | 17,228 | 3709 | 21.5 | 606 | 119 | 19.6 | 1.1 (0.9–1.3) | 0.270 |
| 60–69 | 16,114 | 4828 | 30.0 | 677 | 132 | 19.5 | 1.5 (1.3–1.8) | <0.001 |
| 70–79 | 20,783 | 7238 | 34.8 | 942 | 203 | 21.5 | 1.6 (1.4–1.8) | <0.001 |
| ≥80 | 28,799 | 12,662 | 44.0 | 1111 | 325 | 29.3 | 1.5 (1.4–1.7) | <0.001 |
| Race/ethnicity*** | ||||||||
| White | 46,829 | 14,303 | 30.5 | 1979 | 323 | 16.3 | 1.9 (1.7–2.1) | <0.001 |
| Black | 3848 | 1372 | 35.7 | 177 | 49 | 27.7 | 1.3 (1.0–1.6) | 0.040 |
| East Asian | 911 | 301 | 33.0 | 40 | 8 | 20.0 | 1.7 (0.9 - 3.1) | 0.116 |
| Brown | 31,114 | 9724 | 31.3 | 1738 | 344 | 19.8 | 1.6 (1.4 - 1.7) | < 0.001 |
| Indigenous | 192 | 42 | 21.9 | 53 | 9 | 17.0 | 1.3 (0.7–2.5) | 0.447 |
Asterisks refer to missing data for cases / deaths associated with COVID-19 or influenza according to each variable: *region, **sex, and ***race/ethinicity.
Region*: COVID-19: 27 cases and 15 deaths.
Sex**: COVID-19: 11 cases and 3 deaths.
Race/ethnicity***: COVID-19: 16,155 cases and 3985 deaths; Influenza: 792 cases and 119 deaths.
CFR, case-fatality rate; RR, relative risk; CI, confidence interval.
The overall results of this population-based study showed that case-fatality rates for COVID-19 and influenza were higher in the poorest regions of the country, among Blacks, and older individuals. Brazil has large social and economic disparities, which may explain the higher occurrence of deaths from these diseases in individuals living in more deprived areas. In addition, there is evidence that mortality from viral respiratory diseases is higher among older adults2,3 and is associated with the presence of inherent frailties and multiple morbidities, immunosenescence, and a lower immune response to vaccines.4 Our findings also strengthen the evidence that individuals with COVID-19 have an increased risk of death compared to those with influenza infection.5 It has been suggested that disease severity, prolonged hospital stay, and insufficient therapeutic options are possible contributing factors to the increased risk for mortality among hospitalized patients with COVID-19.6 Furthermore, there is emerging evidence that SARS-CoV-2 infection can lead to a higher inflammatory state associated with dysregulation of the type-I interferon (IFN) response and its downstream cytokine signatures than other respiratory viruses, including influenza.7
Although the influenza H3N2 (Darwin) first circulated in Brazil from the end of 2021, it is possible that a cross reactivity antibody response from past exposure to other types of influenza virus provided a certain grade of protection against the disease.8 A “cross-protection” against the Darwin strain may also have been achieved through the flu vaccine available in 2021 in the country, which may have influenced lethality rates for the out-of-season influenza. It is important to highlight that vaccine coverage for the Brazilian population against COVID-19 at the beginning of 2022 was approximately 67%, and although the Omicron variant was associated with less severe outcomes than Delta and the original SARS-CoV-2 strain9, it has been shown that this emerging variant of concern is characterized by evading vaccine-induced immunity and high levels of transmission.10 Therefore, the third wave driven by Omicron in Brazil may have led to significant morbidity especially in older people, unvaccinated or partially vaccinated individuals and vulnerable populations, with a high case-fatality rate among those with the most severe forms of COVID-19 requiring hospitalization.11
The results of this study showed that the case-fatality rates and risk of death from COVID-19 and influenza A/H3N2 in Brazil were influenced by socioeconomic factors and age. Furthermore, we found evidence from population-based data that the risk of death from COVID-19 is higher than that from influenza virus infection.
Authors’ contributionsAll authors contributed equally to the manuscript.
FundingThe authors declare no financial support.
Conflict of interestThe authors have no competing interests to declare.
The following are the supplementary data to this article:
