




Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection has been described in all age groups with children representing only about 2–5% of all cases worldwide.1–4 Such low percentages could be explained by a higher number of asymptomatic coronavirus disease 2019 (COVID-19) in children, along with milder symptoms,5 so they are less likely to be studied. Moreover, data from countries that have performed universal screening at the community level suggest that children have low overall prevalence, as showed in an Icelandic study where children under 10 years of age tested all negative for the SARS-CoV-2 real-time polymerase chain reaction (RT-PCR).6
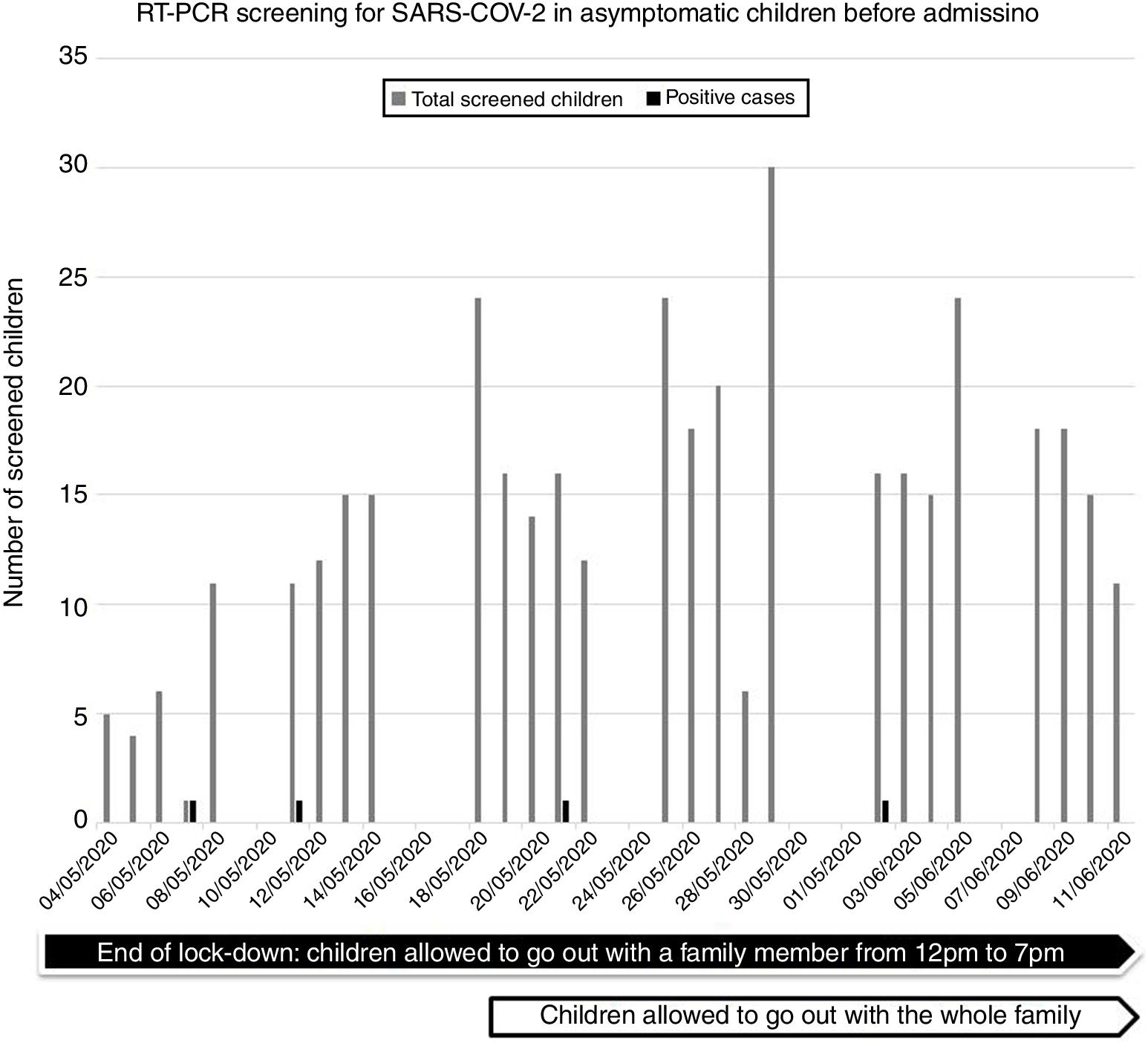
Otherwise, we yet know that children might be much less important spreaders for SARS-CoV-2 transmission than adults.7–9 However, these studies were performed before or during lock-down measures were implemented, and their results should be taken with caution. Detailed epidemiological studies including childhood data will be very useful to guide public health decisions regarding school reopening. We report on cases of asymptomatic SARS-CoV-2 infection among children screened before admission at a reference children's hospital in Barcelona (Catalonia, Spain). We screened asymptomatic adults and children for SARS-CoV-2 by RT-PCR in respiratory samples who had to be admitted for any cause or subjected to a procedure over the airway, from May 4th to June 11th, 2020, once lock-down measures were partially released and children were allowed to go out with their relatives (Fig. 1). Those cases previously confirmed of SARS-CoV-2 were excluded from testing. Patients, or parents or legal tutors of children were asked for symptoms or recent contact with a person with suspected or confirmed COVID-19 disease within the last 14 days.

Nasopharyngeal aspirate specimens were tested for SARS-CoV-2 by using several real-time RT-PCR assays (Allplex™ 2019-nCoV, Seegene, Korea, or Cobas® SARS-CoV-2, Roche Diagnostics, USA) at our Microbiology laboratory. We recorded the demographic features, exposure history, and RT-PCR results.
During the study-period, 3777 RT-PCR tests were performed for universal screening. Among those, 3380 were adults and 397 were children. Infection prevalence rates of SARS-CoV-2 infection were 0.27% (9/3380) among adults, and 1.0% (4/397) among children, significantly higher than adult rate (p=0.017).
Among the 397 asymptomatic children the median [IQR] age was 9 [4–13] years, 58% (230/397) were male. No significant differences were observed for testing positive SARS-CoV-2 by sex (p=0.74) or by age (p=0.18). The four asymptomatic case-patients had an epidemiological link (household contact) with a confirmed adult COVID-19 case.
These findings suggest a very low (1%) prevalence of positive SARS-CoV-2 test results among asymptomatic children under 18 years of age during the post-peak period of the epidemic in Spain, when children have been allowed to enjoy their playing time in the street but not to attend school. As strength, this study shows the prevalence of SARS-CoV-2 infection during a low-incidence period among this population, when restriction of testing was not a dairy challenge due to the limited availability of tests, and hence, no selection bias occurred by focusing laboratory confirmation mainly on those cases with clear symptomatology.
In contrast, asymptomatic children were more likely to have a positive result for SARS-CoV-2 RT-PCR than adults (p=0.017) reinforcing the fact that children have at least the same probability to be infected than adults, as suggested by other authors.1–4 SARS-CoV-2 infection children has significantly less probability to present with clinical manifestations, as recently demonstrated in an age-structured mathematical model, were authors stated that interventions aimed at children might have a smaller impact on reducing COVID-19 transmission.10 Aligned with this, in our data we found that all the positive children had an adult as an epidemiological link.
Our report has some limitations, firstly the sample size of asymptomatic positive cases is relatively small, and secondly the study is limited to a single healthcare center.
In conclusion, despite the low prevalence found in the universal screening, it allowed us to implement preventive and control measures for the new diagnosed cases. These results should be interpreted with caution, as data was collected right after the end of confinement measures, and the epidemiology situation changes over time. However, as children are returning to the new “normality”, screening of asymptomatic SARS-CoV-2–infected cases among this population seems reasonable to monitor COVID-19 prevalence in children.
We thank the nursing team involved in the sample collection.
