



COVID-19 pandemic increased medical services demand aside from interrupting daily clinical practice for other diseases such as inflammatory bowel disease (IBD). Here we present the results of a survey to gain the perception of IBD specialists in their patient-management using telemedicine in their daily practice.
MethodsThis was an observational survey study among physicians focused on IBD (gastroenterologist, surgeons, and pediatricians) members of the Spanish Working Group on Crohn's Disease and Ulcerative Colitis (GETECCU), the Spanish Association of Gastroenterology (AEG), and the Spanish Association of Coloproctology (AECP), regarding changes of management of IBD patients.
ResultsWe received a total of 269 responses to the survey (from May to June 2020). Before the pandemic, nearly all the respondents reported performing very frequently their visits face-to-face (n=251, 93.3%) while, during the pandemic, the telephone visits were the most frequent visits performed (n=138, 51.3%). Regarding communication difficulties, 157 (58.4%) respondents reported the impossibility of performing a proper examination as the most relevant issue. Also, 114 (42.4%) respondents considered remote visits more time-consuming than face-to-face visits. Most gastroenterologists (n=188, 83.2%) considered patients with active perianal disease in special need of face-to-face consultation and more than half of the surgeons (n=35, 50.7%) reported having performed an immediate postoperative follow-up remotely.
ConclusionsMost IBD units have implemented remote visits during the pandemic, but most professionals found them more time-consuming and unsuitable for some disease profiles. Therefore, there is a need for the development of better telemedicine systems that can meet professionals’ and patients’ requirements.
La pandemia por COVID-19ha supuesto un incremento en la demanda de atención sanitaria y ha modificado el modelo asistencial de algunas patologías como la enfermedad inflamatoria intestinal (EII). Presentamos los resultados de una encuesta sobre el papel de la telemedicina en el manejo de pacientes con EII.
Material y métodosEstudio observacional mediante encuesta dirigida a gastroenterólogos, cirujanos y pediatras especializados en EII, miembros del Grupo Español de Trabajo en Enfermedad de Crohn y Colitis Ulcerosa, la Asociación Española de Gastroenterología y/o la Asociación Española de Coloproctología.
ResultadosRecibimos un total de 269 respuestas (mayo a junio de 2020). Antes de la pandemia, el 93,3% de los participantes afirmó llevar a cabo la mayor parte de sus consultas de manera presencial. Durante la pandemia, la consulta telefónica se ha convertido en la modalidad preferida por el 51,3%. El principal inconveniente de la asistencia telemática fue la imposibilidad de llevar a cabo una exploración física según el 58,4%. Además, el 42,4% aseguró emplear más tiempo en este tipo de consultas. Entre gastroenterólogos, el 83,2% consideró que el paciente que más puede beneficiarse de la visita presencial es aquel con enfermedad perianal activa. Y, por último, el 50,7% de los cirujanos afirmó haber realizado controles remotos en el postoperatorio inmediato.
ConclusionesSi bien las unidades de EII han implementado durante la pandemia herramientas de telemedicina, muchos de los encuestados encontraron dificultades en su implementación. Es necesario adecuar y mejorar estos nuevos canales de asistencia remota para satisfacer las necesidades de profesionales y pacientes.
Coronavirus disease 2019 (COVID-19), caused by the new severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), was declared a pandemic by the WHO in March 2020. By the end of July 2021, nearly 190 million cases of COVID-19 had been reported worldwide,1 dramatically increasing the demand for medical services and directly and indirectly collapsing healthcare systems at all levels of care. Very few cases of COVID-19 have been reported to date in patients with inflammatory bowel disease (IBD).2,3 However, the precise extent of the clinical manifestations of COVID-19 in individuals with immune-inflammatory diseases is still unknown,2 and the appropriate and follow-up of IBD patients have become a challenge.
One of the main concerns of patients with IBD during the pandemic has been the interruption of face-to-face medical visits, due to mobility restrictions and lockdowns imposed in most countries during the months of maximum spread of the virus. Moreover, the decrease in endoscopic explorations and scheduled surgeries, the interruption of some clinical trials, as well as usual daily practice, have generated considerable concern among both patients and health professionals.4,5 In Spain, because of the pandemic restrictions, many health centers activated telephone and email helplines to answer patients’ queries on the risk of infection by SARS-CoV-2, their prescribed treatment, or IBD itself.
For all these reasons, remote consultation has become an essential tool to minimize face-to-face visits in the hospitals, while ensuring adequate monitoring and control of the disease in these patients. In other countries, some preexisting remote monitoring platforms, such as TELE-IBD, myIBDcoach, and HealthPROMISE, have proven to be safe and effective in ensuring the appropriate follow-up of IBD patients.6–9
In Spain, our study group developed the web platform TECCU, which proved to be a safe, cost-effective strategy to improve health outcomes, especially in complex IBD patients.10,11 Besides providing remote healthcare, telemedicine is extremely useful during a pandemic for minimizing exposure to the virus. Moreover, telemedicine enhances education and telemonitoring that can promote patients’ empowerment and self-management12,13 and could also alleviate the pressure on healthcare system in routine practice. However, its forced implementation as a response to the current situation may raise some concerns about its use in some settings. Therefore, the main aim of this study was to gather information on the changes and challenges perceived by IBD specialists, including general gastroenterologists, pediatricians, and surgeons in the management of IBD patients using remote systems in their daily practice, to understand the advantages and disadvantages of telemedicine during the COVID-19 pandemic.
Materials and methodsStudy design and respondentsThis was an observational survey study conducted to assess changes in the management of IBD patients due to the COVID-19 pandemic and the satisfaction of health professionals with the available remote visit systems.
We designed an 18-question survey using the SurveyMonkey platform. Questions included demographic characteristics and questions related to medical practice before and after the onset of the pandemic. Five specific questions addressing specialists on their practice were also included. Answers were collected anonymously, and all the information was processed following Organic Law 3/2018 on the Protection of Personal Data and guarantee of digital rights (LOPDGDD).
The survey was revised and approved by the Spanish Working Group on Crohn's Disease and Ulcerative Colitis (GETECCU), the Spanish Association of Gastroenterology (AEG), and the Spanish Association of Coloproctology (AECP), and sent on their behalf to their members (IBD specialists including general gastroenterologists, pediatrists, and surgeons) by email on May 25th, 2020. Two additional reminders were made later before the deadline for submission (June 28th, 2020).
Statistical analysisA descriptive analysis of the survey responses was made, with continuous variables reported as medians and interquartile range, and categorical variables reported as percentages (%) with 95% confidence intervals.
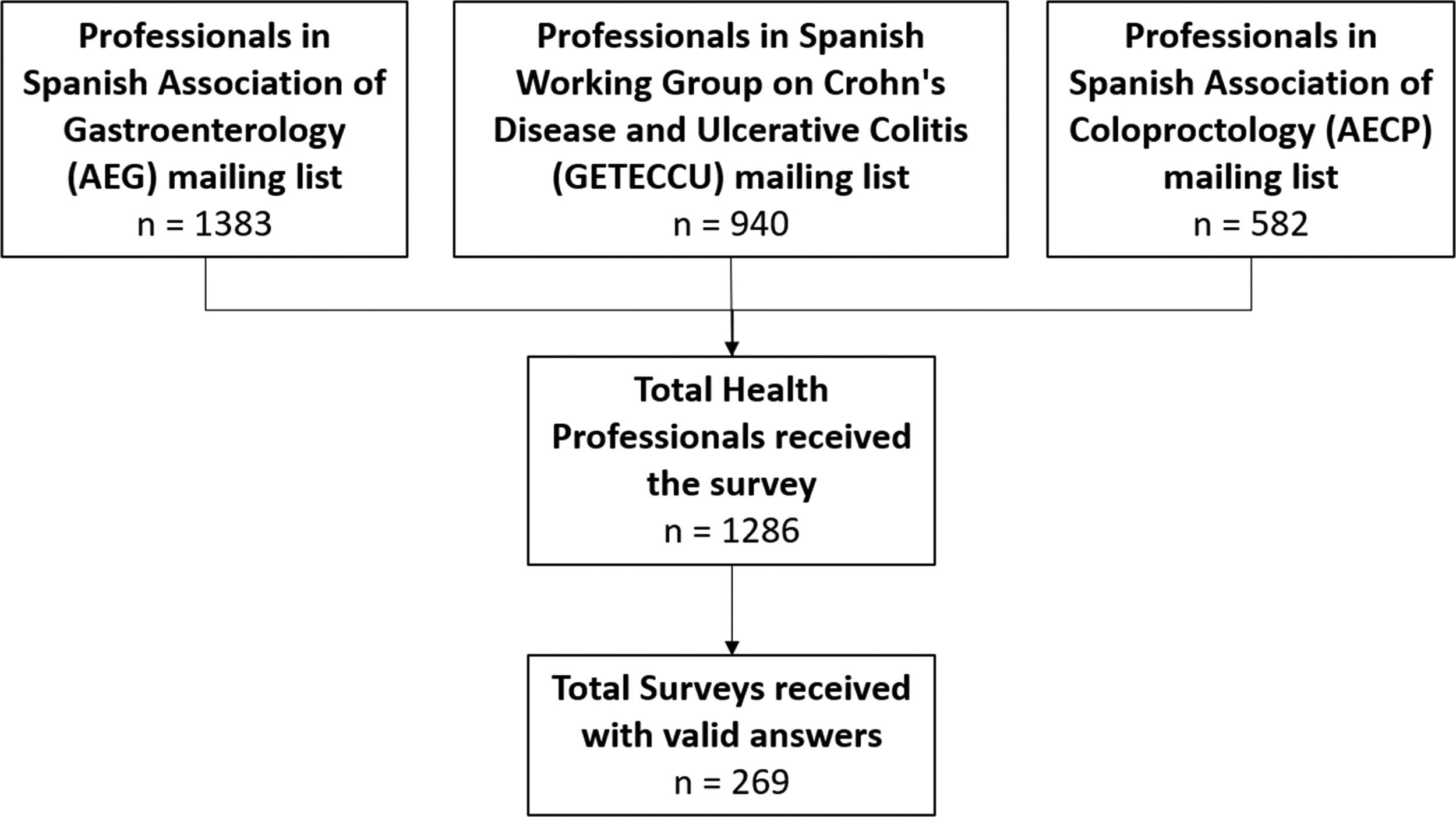
ResultsRespondents and participationSurveys were sent to the mailing lists of the members of the Spanish scientific societies AEG, GETECCU, and AECP (n=1383, n=940, and n=582, respectively). However, some of the professionals are members of more than one society, so the total number of surveys received by professionals, taking into account possible redundancies, was 1286. The total number of valid responses received between May 25th and June 28th of 2020 was 269 (Fig. 1).

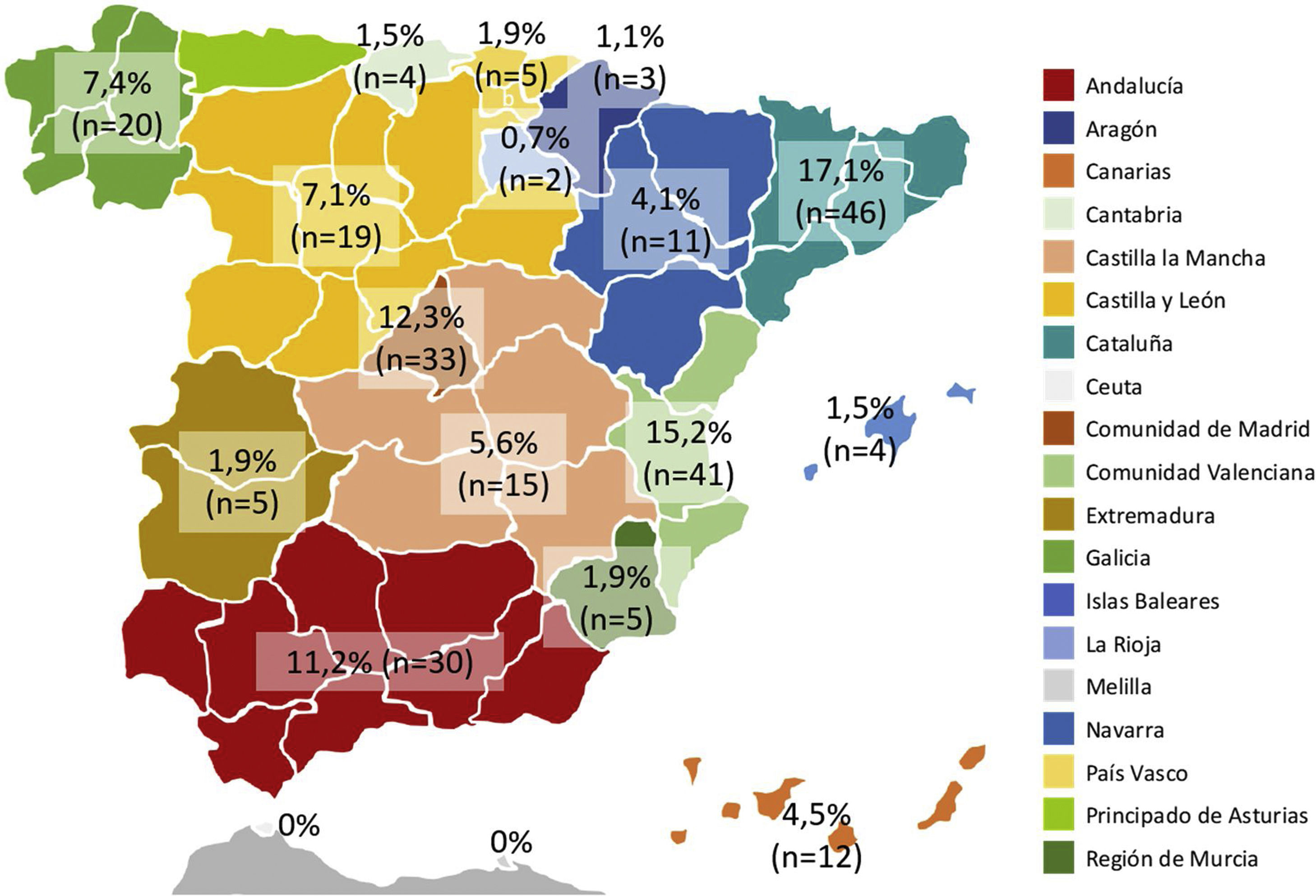
Catalonia and the Valencian Community were the regions with most respondents, followed by Madrid Community and Andalusia (Fig. 2). Most respondents were gastroenterologists, followed by surgeons and pediatricians (80.7%, 217/269; 16.4%, 44/269; and 3.0%, 8/269; respectively), and younger than 40 or between 40 and 50 years old (39.4%, 106/269 and 34.6%, 93/269, respectively). Three out of four health professionals worked in a public university hospital and very few worked in private centers (75.1%, 202/269 and 2.2%, 6/269, respectively). Almost all respondents used electronic medical records in their daily practice (97.8%, 263/269).
Routine practice visits before COVID-19
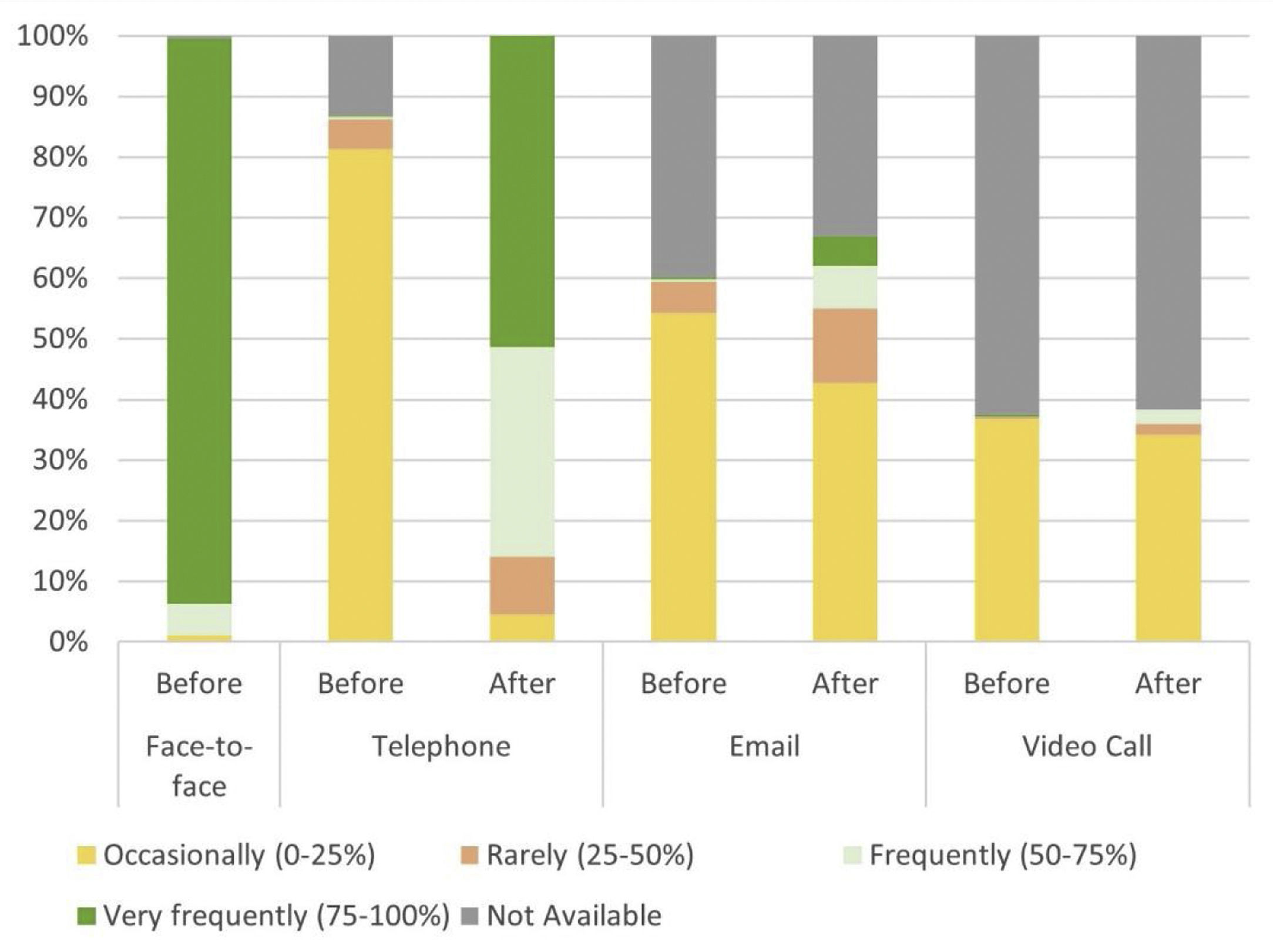
Regarding the routine practice of respondents before the onset of the pandemic, nearly all reported conducting most of their patient visits face-to-face (75–100%) (Table 1, Fig. 3). Most respondents reported offering medical care by telephone occasionally (0–25% of visits). More than half of the respondents acknowledged occasionally following up patients via email (0–25% of visits), or while one fifth did this slightly more frequently (25–50%). Notably, more than half of the respondents reported that contacting patients by video calls was not an option in their routine practice (Table 1, Fig. 3).
Questions included in the questionnaire on medical practice before and after the onset of the COVID-19 pandemic.
| N (%) | |
|---|---|
| Visits | |
| What type of consultation was more frequent in your daily practice BEFORE the COVID-19 pandemic? | |
| Face-to-face | |
| Occasionally (0–25%) | 3 (1.1) |
| Rarely (25–50%) | 0 (0.0) |
| Frequently (50–75%) | 14 (5.2) |
| Very frequently (75–100%) | 251 (93.3) |
| Not available | 1 (0.4) |
| Telephone visits | |
| Occasionally (0–25%) | 219 (81.4) |
| Rarely (25–50%) | 13 (4.8) |
| Frequently (50–75%) | 1 (0.4) |
| Very frequently (75–100%) | 1 (0.4) |
| Not available | 35 (13.0) |
| Occasionally (0–25%) | 146 (54.3) |
| Rarely (25–50%) | 14 (5.2) |
| Frequently (50–75%) | 1 (0.4) |
| Very frequently (75–100%) | 1 (0.4) |
| Not available | 107 (39.8) |
| Video calls | |
| Occasionally (0–25%) | 99 (36.8) |
| Rarely (25–50%) | 1 (0.4) |
| Frequently (50–75%) | 0 (0.0) |
| Very frequently (75–100%) | 1 (0.4) |
| Not available | 168 (62.5) |
| How did you manage your patients DURING the COVID-19 pandemic? | |
| By telephone | |
| Occasionally (0–25%) | 12 (4.5) |
| Rarely (25–50%) | 26 (9.7) |
| Frequently (50–75%) | 93 (34.6) |
| Very frequently (75–100%) | 138 (51.3) |
| Not available | 0 (0.0) |
| By email | |
| Occasionally (0–25%) | 115 (42.8) |
| Rarely (25–50%) | 33 (12.3) |
| Frequently (50–75%) | 19 (7.1) |
| Very frequently (75–100%) | 13 (4.8) |
| Not available | 89 (33.1) |
| Video call | |
| Occasionally (0–25%) | 92 (34.2) |
| Rarely (25–50%) | 5 (1.9) |
| Frequently (50–75%) | 6 (2.2) |
| Very frequently (75–100%) | 0 (0.0) |
| Not available | 166 (61.7) |
| What kind of visits could be made DURING the COVID-19 pandemic? | |
| All (first and successive visits) | 121 (45.0) |
| Only successive visits | 41 (15.3) |
| Only first visits | 4 (1.5) |
| Some first and some successive visits | 103 (38.3) |
| Difficulties during remote visits | |
| Have you had any communication difficulties with your patients during remote visits? | |
| Yes | 157 (58.4) |
| No | 112 (41.6) |
| What is the most relevant difficulty encountered during remote visits | |
| Impossibility of performing an examination | |
| Slightly relevant | 20 (7.4) |
| Somehow relevant | 64 (23.8) |
| Fairly relevant | 90 (33.5) |
| Very relevant | 95 (33.3) |
| Patients do not report their health status properly | |
| Slightly relevant | 69 (25.7) |
| Somehow relevant | 105 (39.0) |
| Fairly relevant | 77 (28.6) |
| Very relevant | 18 (6.7) |
| Impossibility of completing some visits (missing visits or lack of tests results) | |
| Slightly relevant | 59 (21.9) |
| Somehow relevant | 71 (26.4) |
| Fairly relevant | 87 (32.3) |
| Very relevant | 52 (19.3) |
| Physician-patient emotional relationship becomes difficult | |
| Slightly relevant | 61 (22.7) |
| Somehow relevant | 93 (34.6) |
| Fairly relevant | 77 (28.6) |
| Very relevant | 38 (14.1) |
| Compared to face-to-face visits, remote visits last… | |
| More time | 114 (42.4) |
| Less time | 76 (28.3) |
| Same amount of time | 79 (29.4) |

Since the onset of the pandemic, all respondents reported using telephone medical care for some of their patients (Table 1, Fig. 3). Half of the respondents conducted visits by telephone in almost all cases (75–100% of the visits), and a further third conducted half or more of their visits by telephone. Remarkably, since the onset of the pandemic, the number of respondents using email to assist their patients increased. Before the pandemic, only 1 participant out of 269 reported using email frequently (i.e., more than 50% of the visits), whereas after the onset of the pandemic, this proportion increased to 32 out of 269 respondents (Table 1, Fig. 3).
Notably, the use of video call consultations was not an option for more than half of the respondents (61.7%, 166/269) and nearly one out of three respondents (34.2%, 92/269) reported using video call consultation very occasionally (0–25% of the visits) (Table 1, Fig. 3).
Email availability and useNearly half of the respondents (46.1%, 124/269) reported that they did not have an email account for medical consultations. Of the respondents who did have an email account for medical consultations with their patients (53.9%, 145/269), more than half (27.9%, 75/269) reported that they controlled the account themselves while nearly one-third (17.5%, 47/269) reported that the specialist nurse maintained control of the email account.
Just over half of the respondents (51.7%, 139/269) reported using email for medical consultations with patients. Of these, more than half (64%, 89/139) were consultations related to the disease, while the remaining consultations (36%, 50/139) were related to administrative aspects (change of appointments, medical reports, prescriptions, etc.).
Challenges perceived during remote visitsMore than half of the respondents reported some disadvantages associated with remote visits compared to face-to-face visits (Table 1). The inconvenience reported most frequently as very relevant was the impossibility of examining patients. Respondents also considered it very relevant that some consultations are not completed properly (e.g., missing visits or tests). Furthermore, 38 out of 269 respondents indicated that the physician-patient emotional relationship is more difficult in remote visits, and 18 out of 269 respondents noted that the patients’ difficulties in communicating their current health status prevents a correct assessment (Table 1).
Most respondents reported that remote visits take longer than face-to-face visits or at least the same amount of time. Less than a third of respondents reported spending less time in remote visits than in face-to-face visits (Table 1).
Specific questions for the specialistsSome of the last questions of the questionnaire specifically addressed gastroenterologists and others to surgeons.
Most gastroenterologists believe that face-to-face visits are essential for patients with active perianal disease and cases of clinical exacerbation (Table 2).
Specific questions for gastroenterologists regarding medical practice before and after the onset of the pandemic of COVID-19.
| N (%) | |
|---|---|
| What is the average proportion of these pathologies among your patients before the onset of the pandemic? | |
| Colorectal diseases | |
| None | 26 (11.9) |
| Low (0–25%) | 130 (59.4) |
| Moderate (25–50%) | 47 (21.5) |
| High (50–75%) | 14 (6.4) |
| Very high (75–100%) | 2 (0.9) |
| Inflammatory bowel disease | |
| None | 12 (5.3) |
| Low (0–25%) | 65 (28.6) |
| Moderate (25–50%) | 47 (20.7) |
| High (50–75%) | 42 (18.5) |
| Very high (75–100%) | 61 (26.9) |
| Pancreatic disease | |
| None | 50 (23.2) |
| Low (0–25%) | 146 (67.6) |
| Moderate (25–50%) | 17 (7.9) |
| High (50–75%) | 3 (1.4) |
| Very high (75–100%) | 12 (5.5) |
| Functional disease | |
| None | 10 (4.6) |
| Low (0–25%) | 79 (36.1) |
| Moderate (25–50%) | 59 (26.9) |
| High (50–75%) | 59 (26.9) |
| Very high (75–100%) | 12 (5.5) |
| Among your IBD patients, which have a special need of a face-to-face consultation?a | |
| Patients with active perianal disease | 188 (83.2) |
| Patients with a clinical exacerbation | 155 (68.6) |
| Patients receiving biological treatment | 22 (9.7) |
| Elderly patients | 44 (19.5) |
| Other | 29 (12.8) |
Half of the surgeons reported that they had conducted immediate postoperative follow-ups remotely and most of them considered the main difficulty was revision of the surgical wound (Table 3).
Specific questions for surgeons regarding medical practice before and after the onset of the pandemic of COVID-19.
| N (%) | |
|---|---|
| What was the average proportion of these diseases among your patients before the onset of the pandemic? | |
| Colorectal diseases | |
| None | 16 (28.6) |
| Low (0–25%) | 15 (26.8) |
| Moderate (25–50%) | 14 (25.0) |
| High (50–75%) | 10 (17.9) |
| Very high (75–100%) | 1 (1.8) |
| Inflammatory bowel disease | |
| None | 20 (35.7) |
| Low (0–25%) | 26 (46.4) |
| Moderate (25–50%) | 7 (12.5) |
| High (50–75%) | 1 (1.8) |
| Very high (75–100%) | 2 (3.6) |
| Proctology | |
| None | 12 (21.4) |
| Low (0–25%) | 13 (23.2) |
| Moderate (25–50%) | 16 (28.6) |
| High (50–75%) | 11 (19.6) |
| Very high (75–100%) | 4 (7.1) |
| Pelvic floor or functional disease | |
| None | 23 (41.1) |
| Low (0–25%) | 24 (42.9) |
| Moderate (25–50%) | 4 (7.1) |
| High (50–75%) | 3 (5.4) |
| Very high (75–100%) | 2 (3.6) |
| Have you performed “immediate” postoperative follow-ups remotely? (first visits after surgery or similar) | |
| Yes | 35 (50.7) |
| No | 34 (49.3) |
| Have you experienced any difficulties?a | |
| Problems checking the surgical wound | 46 (75.4) |
| Problems checking the stoma | 33 (54.1) |
| Problems explaining or clarifying postoperative care | 15 (24.6) |
| Other | 13 (21.3) |
The COVID-19 pandemic has created a huge challenge for the safe provision of quality care. Spain is one of the most affected countries and this has dramatically altered care pathways in healthcare centers and, with it, our routine management of outpatients with IBD.4,5,14–16 The results of our study showed that many IBD units have adapted to the circumstances using telephone and e-mail to contact their patients, and these tools have expanded their presence in clinical practice during the pandemic. They are usually considered useful and cost-effective, but the perspective of healthcare professionals with their use has not been addressed thus far.
Although patients with IBD are at increased risk of infection due to immunosuppression, the incidence of SARS-CoV-2 infection in IBD patients is estimated to be similar to that of the general population.3,17 Data are still scarce and minimizing exposure in these patients is a priority. To this end, a key tool during the pandemic has been the use of telemedicine, understood as the provision of medical care using communication technologies in the form of text, video, or audio.17 This strategy not only reduces the individual risk of exposure to the virus but also reduces community transmission in high-traffic areas such as hospitals and health centers, care burdens at times of high demand, and the use of personal protective equipment. It is also safe, easy to use, and well accepted by most patients.6,8,18
Despite the exceptional nature of the situation in which we find ourselves and the potential benefits of telemedicine, its increasing use raises new doubts and uncertainties that are hampering its widespread implementation. Among them, confusion regarding medical liability due to the absence of specific regulations governing its use in our legal system of laws and regulations. Moreover, telemedicine has been successful in some patients and in certain disease profiles, but not in others, and some patients have an inherent need for face-to-face physical explorations, such as those with active perianal disease, as pointed out by the gastroenterologists who participated in this survey. Thus, the favorable efficacy and cost-effectiveness reported in previous trials11 may not apply to all patients and, besides, more than 70% of respondents in our survey reported that telephone consultations were not time-saving procedures. In addition to the disadvantages of remote visits most frequently reported by the study respondents, namely the impossibility to perform examinations and complete visits properly and inhibition of the physician-patient relationship, another limitation to consider is access to telemedicine, especially for older patients, whether due to the lack of a device or the difficulties that patients may encounter in its use. Another important barrier may be the integration of IBD telemedicine platforms in electronic medical records, although some efforts have been made toward solving this specific issue.19 Regardless of the current or future possible pandemic events, telemedicine shows the potential, in terms of cost-effectivity and suitability to be the future standard to manage IBD patients.11,15 Thus, efforts must be focused on the further promotion and the application of telemedicine platforms properly integrated into all levels of the health care system.
This study has some limitations. First, the survey was delivered on behalf of the Spanish scientific societies to all their members, but the representativity of the results must be read in the context of the participation of healthcare providers with a special interest in IBD management. Thus, their responses may not represent the reality of the whole population of gastroenterologists, surgeons, and pediatricians. The low response rate is another limitation of the study, especially between surgeons and pediatricians. Epidemiological variations in the incidences of COVID-19 among regions in Spain can also reflect different healthcare burdens or even different management approaches that may be reflected in the different responses from respondents on the use of telemedicine.
ConclusionsThe COVID-19 pandemic has generated numerous social and healthcare challenges, while daily practice has changed dramatically to respond to the imperative need to adapt to ensure the continuity of care of our IBD patients. Our results show that most IBD units have implemented remote visits for the management of IBD patients. However, most professionals found remote visits more time-consuming than face-to-face visits and some disease profiles, such as postoperative care or active perianal disease, are considered unsuitable candidates for remote care. Therefore, there is a need for the development of adequate telemedicine systems with a patient-centered design that can perform according to professionals’ and patients’ requirements.
FundingSupported by: This study was supported by grants from the Instituto de Salud Carlos III-Fondo de Investigaciones Sanitarias (FIS PI18/00593), co-funded by FEDER (Fondo Europeo de Desarrollo Regional).
Conflicts of interestThere are none to report.
The authors would like to thank the Spanish Working Group on Crohn's Disease and Ulcerative Colitis (GETECCU), the Spanish Association of Gastroenterology (AEG), and the Spanish Association of Coloproctology (AECP).
The following are the supplementary data to this article:

