




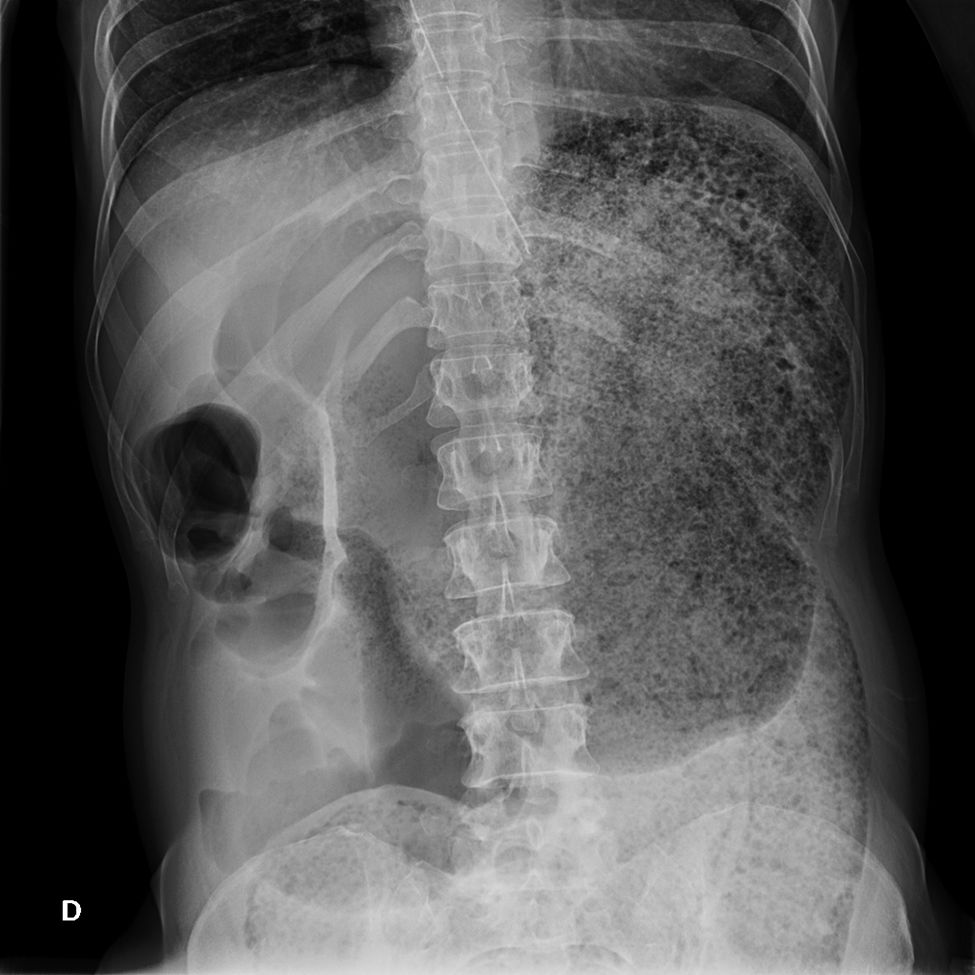

45-year-old woman diagnosed with advanced Huntington's chorea. She went to the A&E due to vomiting, with nondescript abdominal examination and digital rectal examination. The abdominal X-ray (Fig. 1) showed loop dilation, so conservative treatment was initiated.

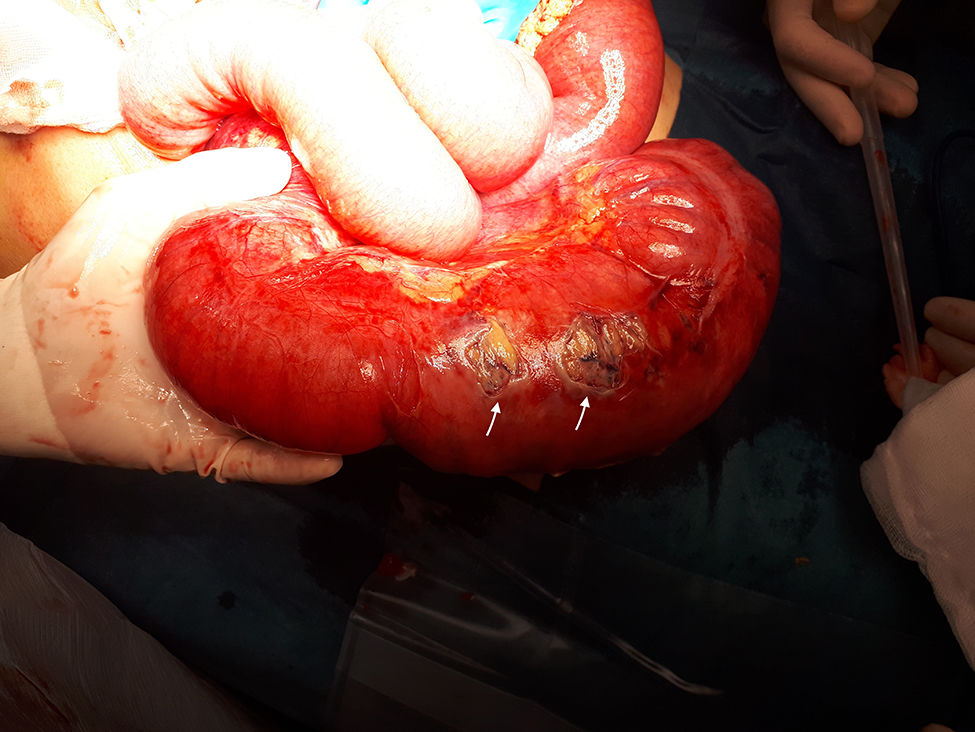
In the absence of improvement, a CT scan was (Fig. 2) performed 2h later, revealing intestinal occlusion. Emergency surgery was scheduled, in the course of which a volvulated and ischaemic right colon was observed (Fig. 3). A right hemicolectomy and mechanical isoperistaltic L-L anastomosis were performed. The patient was discharged without complications.


Huntington's chorea has an incidence of 1–2 cases/million.1 It presents involvement of the enteric neurons, causing intestinal hypomotility and chronic constipation.1,2
Caecal volvulus has an incidence of 3–7 cases/million,3 representing 1–2% of intestinal obstructions. Treatment is initially conservative with the placement of a nasogastric tube.3If symptoms persist, devolvulation by colonoscopy can be considered, although it was ruled out in this case due to pneumatosis and risk of perforation.3 Laparotomy is indicated in cases of absence of improvement or worsening given the high risk of ischaemia and necrosis.3
The association between both diseases is not described in the literature. Caecal volvulus should be suspected in occlusive conditions in these patients in whom, as they present less pain, the diagnosis is more difficult and delayed.2
Please cite this article as: Ferrer-Inaebnit E, Segura-Sampedro JJ, Molina-Romero FX, González-Argenté X. Oclusión e isquemia por vólvulo de ciego en corea de Huntington. Gastroenterol Hepatol. 2020. https://doi.org/10.1016/j.gastrohep.2020.03.005
