There is controversy concerning the risk/benefit of anticoagulation/antiaggregation in chronic kidney disease (CKD) patients. We analyzed the impact of anticoagulation/antiaggregation on anaemia and haemorrhagic events in CKD patients.
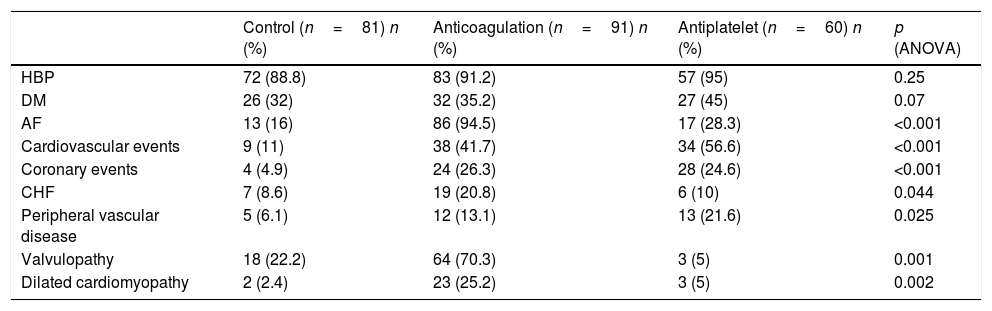
Patients and methodsA total of 232 CKD patients stages 3 and 4 were followed during a mean follow-up time of 36.7±11.6 months: 81 patients did not receive any anticoagulation or antiaggregation treatment, 91 received anticoagulation treatment and 60 patients received platelet antiaggregation. Haemorrhagic and cardiovascular events were recorded.
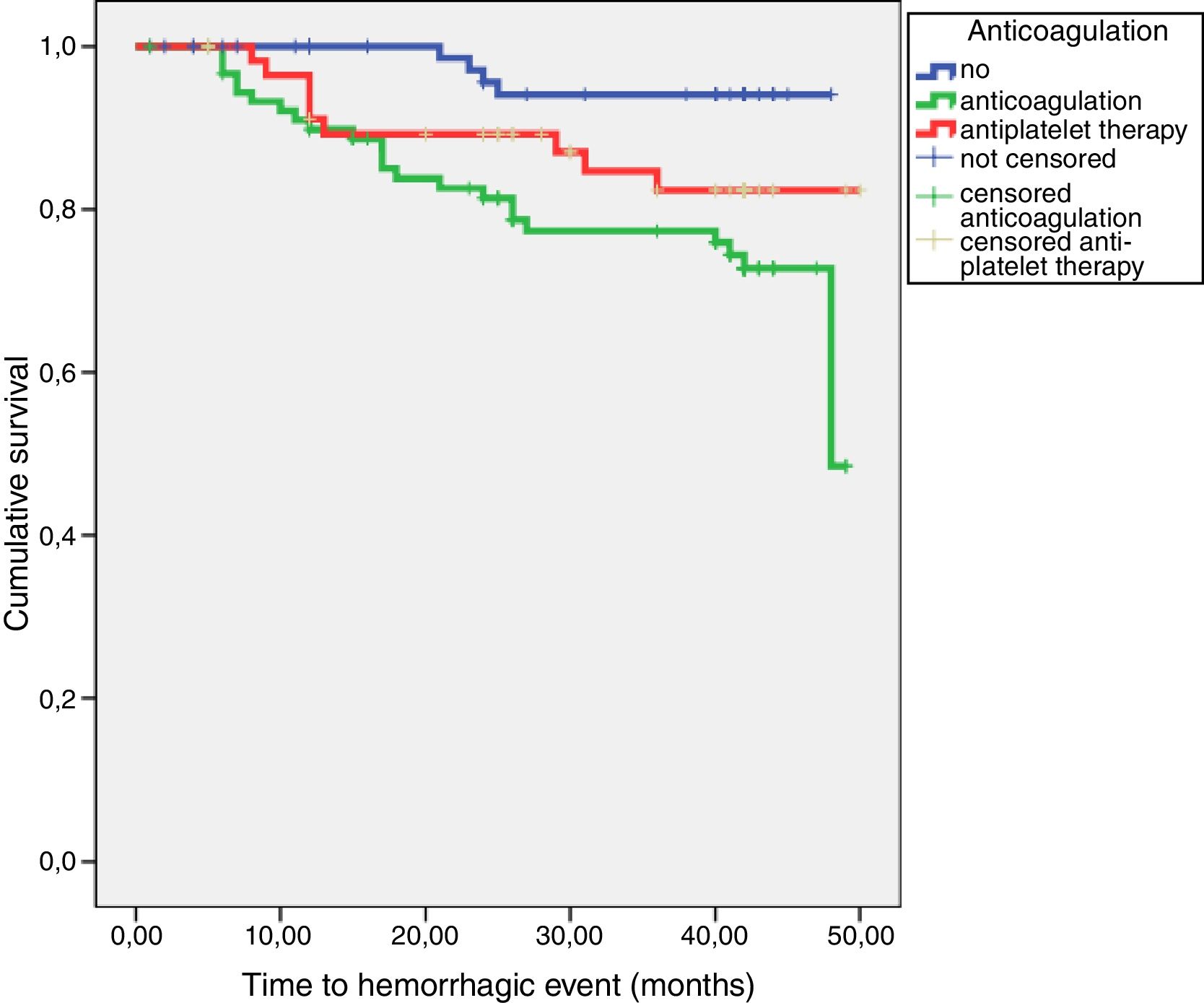
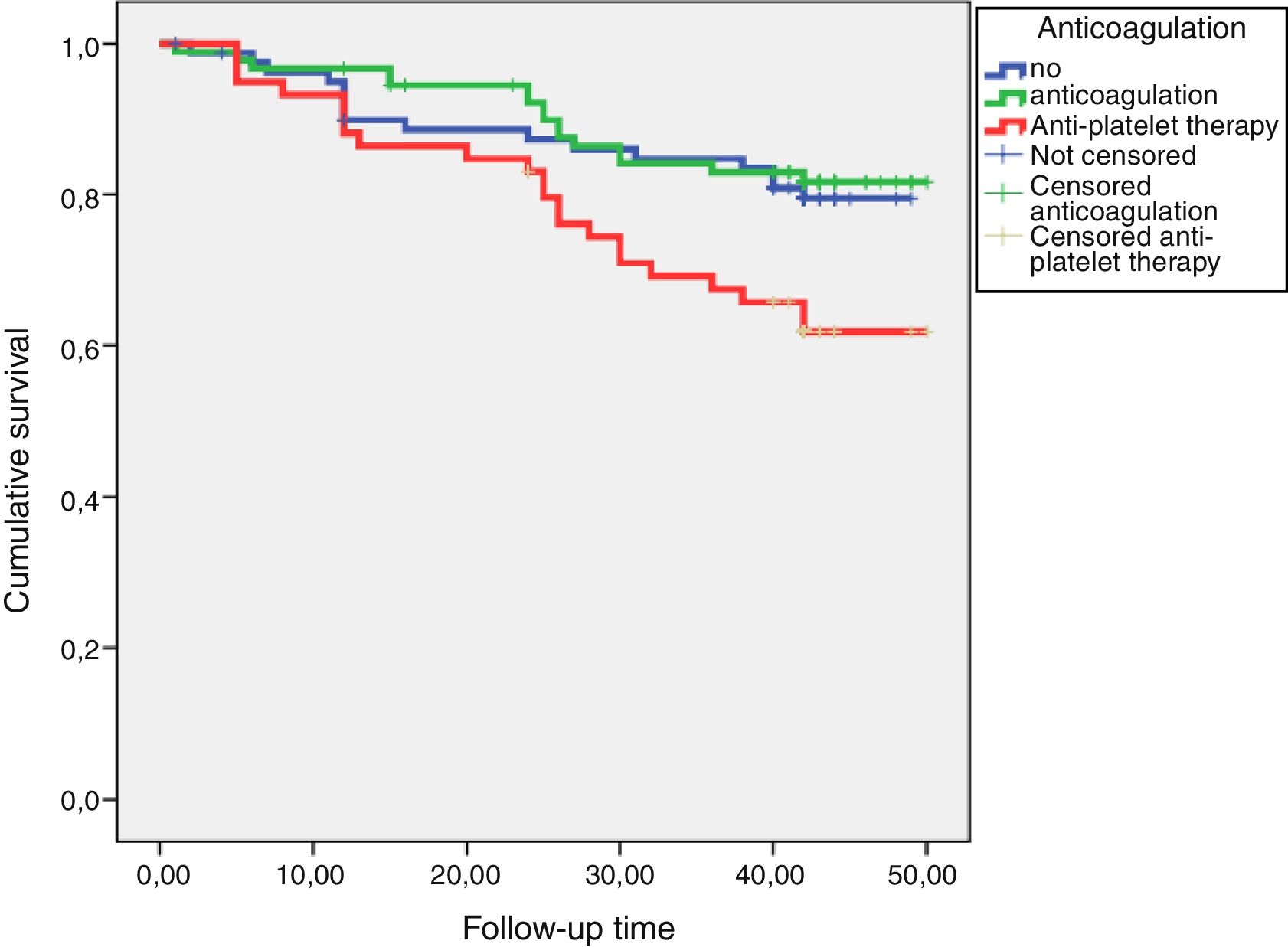
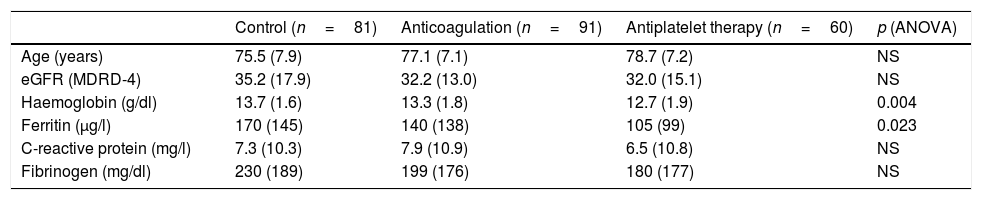
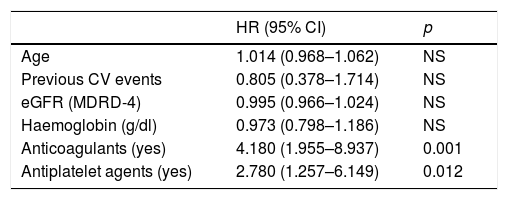
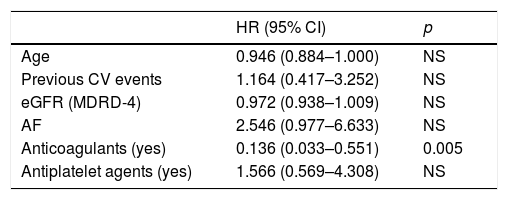
ResultsHaemoglobin and ferritine levels were significantly higher in patients who did not receive anticoagulation or antiaggregation (Hb 13.7±1.6, 13.3±1.8 and 12.7±1.9g/dl, p=0.004; ferritine 170±145, 140±138, 105±99μg/l, p=0.023). During follow up, 36 haemorrhagic events were registered: 4 in the control group, 23 in the anticoagulation group and 9 in the antiaggregation group (log rank 12.5; p=0.002). In a Cox model adjusted by age, renal function and haemoglobin levels, the anticoagulation increased the risk of bleeding by 4 times (HR 4.180, 1.955–8.937); p=0.001) and antiaggregation by almost 3 times (HR 2.780, 1.257–6.149, p=0.012). A total of 64 cardiovascular events were registered, 21 of which were classified as atherosclerotic events: 10 in the antiaggregation group, 8 in the control group and 3 in the anticoagulation group (log rank: 8.351; p=0.015). Anticoagulation treatment showed a reduction in the risk of atherosclerotic events (HR 0.136, 0.033–0.551, p=0.005) while platelet antiaggregation did not modified this risk (HR 1.566, 0.569–4.308).
ConclusionsAnticoagulation and antiaggregation increase haemorrhagic risk in patients with CKD and worsen anaemia. Anticoagulation reduces atherosclerotic events by more than 85% while platelet antiaggregation does not modify this risk.
Existe controversia sobre el riesgo/beneficio de anticoagular/antiagregar a pacientes con enfermedad renal crónica (ERC). Analizamos el impacto de la anticoagulación/antiagregación en pacientes con ERC sobre el riesgo hemorrágico, cardiovascular y la mortalidad.
Pacientes y métodosSe estudió a 232 pacientes (81 controles, 91 anticoagulados y 60 antiagregados) con ERC en estadios 3 y 4, que fueron seguidos durante un tiempo medio de 33,7±14,8 meses. Se recogieron eventos hemorrágicos, cardiovasculares y mortalidad.
ResultadosLa hemoglobina sérica y los niveles de ferritina fueron significativamente mayores en pacientes controles (hemoglobina 13,7±1,6; 13,3±1,8 y 12,7±1,9g/dl; p=0,004; ferritina 170±145; 140±138; 105±99μg/l; p=0,023). Durante el seguimiento hubo 36 eventos hemorrágicos: 4 en pacientes control, 23 en anticoagulados y 9 en antiagregados (log rank 12,5; p=0,002). En un modelo de Cox ajustado para edad, función renal y niveles de hemoglobina, la anticoagulación aumentó el riesgo de sangrado 4 veces (HR 4,180; 1,955-8,937; p=0,001) y la antiagregación en casi 3 veces (HR 2,780; 1,257-6,149; p=0,012). Se registraron 64 eventos cardiovasculares, 21 de los cuales fueron clasificados como eventos ateroscleróticos: 10 en el grupo de antiagregación, 8 en el grupo control y 3 en el grupo de anticoagulación (log rank: 8,351; p=0,015). El tratamiento anticoagulante demostró un efecto protector frente al riesgo de padecer eventos ateroscleróticos (HR 0,136; 0,033-0,551; p=0,005), mientras que el tratamiento antiagregante no lo modificó (HR 1,566; 0,569-4,308; ns).
ConclusionesLa anticoagulación y la antiagregación aumentan el riesgo hemorrágico en pacientes con ERC y empeoran la anemia. La anticoagulación disminuye el riesgo de eventos cardiovasculares ateroescleróticos en más de un 85% y la antiagregación no lo modifica.