


To determine the prevalence of Internet addiction, psychiatric symptoms and personality type in university students, and to correlate these variables.
MethodsWe enrolled 522 medical students, 281 men and 241 women, with a mean age of 21.2 years. We used a socio-demographic questionnaire, an Internet questionnaire (Young's Internet Addiction Test [IAT]), the General Health Questionnaire, and the Zuckerman-Kuhlman Personality Questionnaire III (ZKPQ).
ResultsThe mean raw score of respondents in the IAT test was 19.72 points. IA had a highly significant correlation with impulsivity (rs=0.244, p<001), neuroticism-anxiety (rs=0.304, p<001) and aggression-hostility (rs=0.143, p=0.001). It also negatively correlated with work effort (rs=−0.136, p=0.002). As for mental health, IA had a highly significant correlation with somatic symptoms (rs=0.174, p<001), anxiety and insomnia (rs=0.219, p<001), social dysfunction (rs=0.118, p<001) and severe depression (rs=0.199, p<001).
ConclusionsThe Internet is a tool for various activities. When used with control it does not cause any problems. However, when control is lost, addiction occurs together with its comorbidities. Certain personality types are predisposed to this loss of control and Internet abuse.
The Internet is currently a critical component of telecommunications, business, education, and entertainment. It is available worldwide and is used to search for information, online communication, financial transactions, retail sales, sexual services and games, among many other uses. With its growing popularity, overuse soon appeared and thus a new disorder, Internet Addiction (IA).1
The first to propose the term IA was the American psychiatrist Ivan Goldberg in 1995, who described the pathological compulsive use of the Internet, with this term being definitely defined by Kimberly S. Young.2 IA is a deterioration in the control of its use, manifested as a set of cognitive, behavioral and physiological symptoms. That is, the person is “net dependent”, making extensive use of the Internet, which generates a distortion of her/his personal, family or professional goals.3
Griffiths4 proposed assessing seven specific areas for Internet addiction: (a) tolerance, (b) spending more time than planned on the Internet, (c) spending most of their time in activities that allow them to be online, (d) spending more time online than in social or recreational activities, (e) continuing use despite work, academic, economic or family concerns, (f) failed attempts to stop or reduce use of the Internet and (g) withdrawal. According to this author, the diagnosis should be made in the presence of three or more of the areas described.
Hong et al5 found a reduction in thickness of the right orbitofrontal cortex in adolescents with Internet addiction. This reflects a common neurobiological mechanism between IA and other addictive disorders. Young6 classified it into 5 types: (1) cybersexual addiction to adult chat rooms or pornography; (2) addiction to online friendships or situations that replace real-life relationships; (3) web compulsion to gamble, auction, or obsessively trade; (4) the compulsive search for information on the web, and (5) addiction to computer games and programming. Goldberg7 prefers to replace the term IA with pathological computer use.
Some researchers suggest the existence of vulnerable or high risk groups for Internet addiction, primarily focusing on students. A review in Mexico8 concluded that although it is not yet possible to make the diagnosis of “Internet addiction” as such, it is clear that the behavior associated with excessive Internet use has features that, because of its impact on an individual's functioning and interpersonal relationships, warrants an intervention aimed at this problem.
Investigators have attempted to define the clinical and epidemiological profile of individuals with IA, such as that in a study by Cruzado et al.2 who found that patients with IA were characterized by their young age, high daily Internet user time, predominant use of web games, and a high frequency of marked psychotic behaviors. Young9 assessed depression and IA, and her findings suggest an increase in levels of depression associated with Internet addiction. Due to the susceptibility of young people to present addictions, in this study we determined the presence of Internet addiction, psychiatric symptoms, and personality type in university students and correlated these variables.
Methods and subjectsQuestionnaires were administered during the period of March-April 2013 to medical students who had Internet and agreed to participate voluntarily in the study. It was decided to perform this study in this population because of the ease of processing it at the University. The project was reviewed and approved by the Ethics Committee of our institution.
We determined the size of the sample population (p) to be studied by means of a bilateral interval with a 95% confidence interval (α=0.05), with an estimation of error limits±5% (B=0.05) and considering a conservative approach (p=q=0.5). The result meant that, for a population of 5192 students, a sample of 358 individuals was required. The sampling design used was two-stage. In the first stage we stratified by school year (6 strata) and in the second, clusters were selected. The group formed a conglomerate of students and a census was conducted in each of the eight clusters present in the sample. Sample allocation was proportional to the size of the stratum, that is, proportional to the total number of students of that school year. For the first and second school years, we randomly selected 2 groups each, while in the rest (third, fourth, fifth and sixth) a group or cluster was randomly selected by school year.
Application of the instruments was performed in the regular classroom, on the day and time agreed with the course coordinator. The instruments were applied by groups. A member of the research team explained the purpose of the study, conditions and data confidentiality, and voluntary participation of the students who were present was requested. The average time to complete the questionnaires was approximately 30 to 40min. Questionnaires were administered to a total of 543 students, of whom 21 did not answer completely, therefore these were eliminated.
Instruments and variablesThe instruments considered for the study were: a questionnaire of socio-demographic variables including age, sex, marital status, level of study, persons with whom the individual lives, academic performance, and recreational activities; an Internet questionnaire that collects information on frequency of weekly use, time of use for each connection, connection location, and purpose of the connection, and an IA test consisting of a 20-item questionnaire with Likert type responses with a minimum score of 20 and a maximum of 100 (the higher the score, the greater the problem caused by the use of Internet). A score of 20–39 points is an average online user who has complete control over its use, a score of 40–69 means frequent problems with Internet use, and a score of 70–100 means that use of the Internet is causing significant problems.10,11
Goldberg's General Health Questionnaire in its 28-item version (GHQ 28)12 was also included. This instrument consists of four scales: somatic symptoms, anxiety and insomnia, social dysfunction, and severe depression. Internal consistency (Cronbach's alpha) of the total questionnaire varies between 0.82 and 0.93. Test–retest reliability ranges from 0.85 to 0.90.
The Zuckerman-Kuhlman Personality Questionnaire III, translated and adapted with permission from the authors by González et al.13, consists of 99 items with an alternative true or false answer. This questionnaire isolates the five major personality factors proposed by Zuckerman. Impulsive Sensation Seeking (ISS) consists of 19 items that refer to a willingness to take risks to experience arousal and seek new experiences. They also relate to the lack of planning and the tendency to act impulsively without thinking. The Scale of Neuroticism and Anxiety (NA) also has a total of 19 items that describe emotional instability, stress, worry, phobias and/or fears, obsessive indecision and susceptibility to criticism. Aggression Hostility (AH) is a scale that consists of 17 items related to verbal aggression, rudeness-impoliteness, antisocial behavior, and anger. The Activity (A) scale consists of 17 items referring to the need for activity and an inability to sit around doing nothing. The Sociability (S) scale consists of 17 items, and refers to the number of friends you have and the time devoted to them, the desire for partying, preference for being with others as opposed to being alone and doing activities alone. Finally, the Infrequency scale (I) consists of 10 items related to social desirability, which are not entirely true for everyone.
Statistical analysisDescriptive and inferential statistics were used. For the first proportions, percentages and absolute frequencies for categorical variables were obtained. For continuous and/or numeric variables, measures of central tendency, variability and positioning were calculated. Confidence intervals of 95% for both ratios and means were obtained for inferential statistics. For numeric or continuous variables, the Kolmogorov-Smirnov test was used to test the hypothesis of normality. To examine correlations, parametric (Pearson's) or non-parametric (Spearman's) correlation coefficients were used.
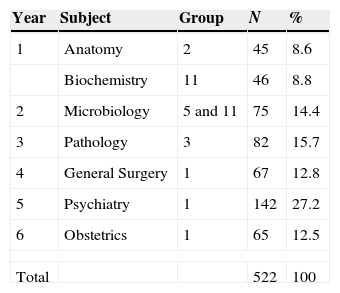
ResultsData analysis was carried out in 522 students, comprising 281 men and 241 women. Of these, 509 were single, 11 married, one common-law married and 1 separated with a mean age of 21.24 years, median 21, SD 3.046 with an age range of 15–61 years (KS=0.147, p=0 001). The level of education, the subject under study and the group of students are shown in Table 1.
Regarding academic performance, 23 considered themselves excellent, 107 very good, 347 good, 42 poor and 3 very poor. Of the total, 327 students engaged in recreational activities and 195 did not. Activities were mainly sports, arts, reading, and video games. Most lived with their family (84.5%).
By analyzing Internet use, it was found that 15 students used the Internet 1 day a week, 5 students, 2 days, 14 students, 3 days, 33 students, 4 days, 25 students, 5 days, 33 students, 6 days and 397, 7 days a week. Connections per day were 0 to 10 times, 86%, 11 to 20 times, 2.4%, 21 to 30 times, 0.4%, 50 times, 0.2%, 144 times, 0.6%, and always, 10.4%.
The approximate time of Internet use each time a user logged in was 1 to 960min and 10.4% referred to staying connected always. Most would connect for 60min (20.1%) followed by 120min (13.2%), and 30min (12.6%). The place chosen as the most frequently used was the home, in 442 (84.7%).
The main reason for being connected to the network most of the time was social networks (Facebook, Twitter, Tumblr, chats) in 43.86%, academic and research activities in 32.95% and entertainment/leisure in 23.18%.
There are differences in IA due to the perception that students have of their academic performance (χ2=10.25, df=3, p=0.016). Those who perceive their academic performance as poor and very poor had the highest Internet addiction test scores.
There was no significant difference in IA due to whether or not a recreational activity was practiced (Z=−0.49, p=0.620). Also, there was no significant difference in IA due to who the person was living with (χ2=2.47, df=2, p=0.29).
The mean raw score of respondents in the IA test was 19.72, with a standard deviation of 12.54 and a range of 0–72 with a possible maximum of 100 points.
The classification of scores according to the interpretation of the IA test showed that 91.8% of the sample had complete control over its use, while 8% had frequent problems and in 0.2%, use caused significant problems.
Internet use caused a greater problem in men with a mean of 21.25 (median 18.00, SD 13.38) unlike women with a mean of 17.95 (median 16, SD 11.25 (U=28,914.5, Z=−2.88, p=0.004). Second, fourth and fifth year students had a greater problem in Internet use (χ2=15.62, df=5, p=0.008).
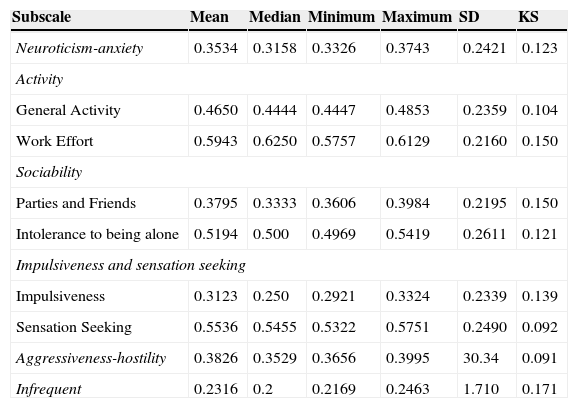
The students’ personality and mental health are shown in Tables 2 and 3.
Results of the Zuckerman-Kuhlman III questionnaire subscales.
| Subscale | Mean | Median | Minimum | Maximum | SD | KS |
|---|---|---|---|---|---|---|
| Neuroticism-anxiety | 0.3534 | 0.3158 | 0.3326 | 0.3743 | 0.2421 | 0.123 |
| Activity | ||||||
| General Activity | 0.4650 | 0.4444 | 0.4447 | 0.4853 | 0.2359 | 0.104 |
| Work Effort | 0.5943 | 0.6250 | 0.5757 | 0.6129 | 0.2160 | 0.150 |
| Sociability | ||||||
| Parties and Friends | 0.3795 | 0.3333 | 0.3606 | 0.3984 | 0.2195 | 0.150 |
| Intolerance to being alone | 0.5194 | 0.500 | 0.4969 | 0.5419 | 0.2611 | 0.121 |
| Impulsiveness and sensation seeking | ||||||
| Impulsiveness | 0.3123 | 0.250 | 0.2921 | 0.3324 | 0.2339 | 0.139 |
| Sensation Seeking | 0.5536 | 0.5455 | 0.5322 | 0.5751 | 0.2490 | 0.092 |
| Aggressiveness-hostility | 0.3826 | 0.3529 | 0.3656 | 0.3995 | 30.34 | 0.091 |
| Infrequent | 0.2316 | 0.2 | 0.2169 | 0.2463 | 1.710 | 0.171 |
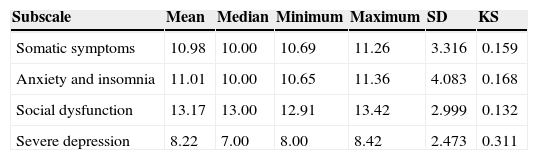
Results of Mental Health subscales.
| Subscale | Mean | Median | Minimum | Maximum | SD | KS |
|---|---|---|---|---|---|---|
| Somatic symptoms | 10.98 | 10.00 | 10.69 | 11.26 | 3.316 | 0.159 |
| Anxiety and insomnia | 11.01 | 10.00 | 10.65 | 11.36 | 4.083 | 0.168 |
| Social dysfunction | 13.17 | 13.00 | 12.91 | 13.42 | 2.999 | 0.132 |
| Severe depression | 8.22 | 7.00 | 8.00 | 8.42 | 2.473 | 0.311 |
According to the results of the Kormogorov–Smirnov test with Lilliefors correction, a normal distribution was not found for any of the variables (p<0.01).
IA has a highly significant correlation with impulsivity (rs=0.244, p<.001), neuroticism-anxiety (rs=0.304, p<.001) and aggression-hostility (rs=0.143, p=.001). This was only significant with sensation seeking (rs=0.95, p=0.030). It was also negatively correlated with work effort (rs=−0.136, p=0.002); the greater the addiction, the lower the work effort.
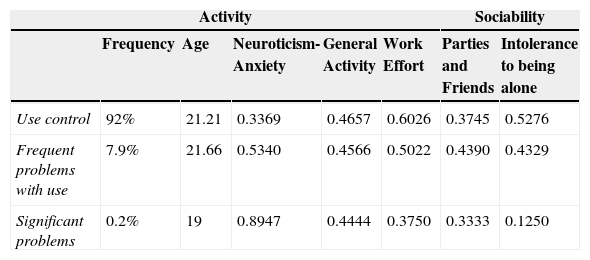
Regarding mental health, IA had a highly significant correlation with somatic symptoms (rs=0.174, p<.001), anxiety and insomnia (rs=0.219, p<.001), social dysfunction (rs=0.118, p<.001) and severe depression (rs=0.199, p<.001). Personality and mental health in the groups formed according to IA test interpretation are shown in Table 4.
Internet addiction, personality and mental health.
| Activity | Sociability | ||||||
|---|---|---|---|---|---|---|---|
| Frequency | Age | Neuroticism-Anxiety | General Activity | Work Effort | Parties and Friends | Intolerance to being alone | |
| Use control | 92% | 21.21 | 0.3369 | 0.4657 | 0.6026 | 0.3745 | 0.5276 |
| Frequent problems with use | 7.9% | 21.66 | 0.5340 | 0.4566 | 0.5022 | 0.4390 | 0.4329 |
| Significant problems | 0.2% | 19 | 0.8947 | 0.4444 | 0.3750 | 0.3333 | 0.1250 |
| Activity | Impulsiveness and Sensation Seeking | Mental health | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Impulsivness | Sensation Seeking | Agressiveness/Hostility | Infrequent | Somatic symptoms | Anxiety and insomnia | Social dysfunction | Severe depression | Total | |
| Use control | 0.2997 | 0.5515 | 0.3760 | 0.2300 | 10.86 | 10.85 | 13.08 | 8.05 | 42.85 |
| Frequent problems with use | 0.4543 | 0.5809 | 0.4577 | 0.2463 | 12.14 | 12.65 | 14.00 | 10.07 | 48.87 |
| Significant problems | 0.5000 | 0.4545 | 0.4706 | 0.4000 | 20 | 19 | 18 | 12 | 69 |
We found, like Young3 and others, that men have a higher prevalence of Internet addiction. Despite the low frequency of IA reported by the students in our analysis, it appears that most use the network seven days a week, mostly 10 times a day, spending an hour on each connection, which seems generally an everyday behavior of young people. It is notable that most responded that they frequently surf the web for a longer period than intended, which shows a lack of control in their use.
We noted a remarkably ludic nature of Internet use since most of the time they connected to the network to participate in social networks and leisure.
Overall, we found a small percentage of students who have problems with Internet use (8.2%); however, this agrees with the literature and the comorbidities found in Internet addiction.
It has been stated that problematic use of the Internet is only the manifestation of an underlying problem, highlighting frequent comorbidities with mood disorders, anxiety, and other addictions.14 Mustafa15 investigated the relationship between IA and psychiatric symptoms and he found a significant relationship between daily use of the Internet and the degree of psychiatric symptoms such as depression, obsessive compulsion, interpersonal sensitivity, anxiety, hostility, phobic anxiety, paranoid ideation and psychoticism. With longer use, more psychiatric symptoms occur. He also found a significant association between the severity of IA and the degree of psychiatric symptomatology.
Ebeling-Witte et al.16 found that scores of shyness were associated with problematic Internet use. That is, the network is used to reduce the deficit perceived in social life by establishing virtual friendships online and to alleviate feelings of loneliness and depression and to avoid attending stressful places. In contrast, Shapira and Goldsmith17 found in a population of subjects with problems with Internet use that 100% met DSM-IV criteria for impulse control disorders not otherwise specified.
In an exploratory study on behavioral problems related to Internet use, a subgroup of netizens who expressed greater anxiety and social dysfunction was identified through the GHQ-28.18
Armstrong, Phillips and Saling19 concluded that self-esteem and the number of hours per week using the network were the variables that best predicted problems related to the Internet. However, impulsivity was not related, which made the authors conclude that unlike other addictions, IA is not characterized by this trait.
In 2012, a study of Egyptian adolescents found that subjects with problematic Internet use were more likely to have anxiety disorders (social phobia, specific phobia, and generalized anxiety disorder).20
Articles that mention the coexistence of psychiatric disorders and Internet addiction were found in a review of data from PubMed carried out up to November 3, 2009. Based on this review, IA is associated with substance use disorder, attention deficit and hyperactivity disorder, depressive disorder, social phobia, and hostility.21
Kubey et al.22 reported four times more academic deterioration in students with IA than was noted in the perception of academic performance in our sample. As to the question of whether or not performing any recreational (extracurricular) activities has an effect – seeking a possible protective factor – no significant difference was found in terms of IA and practicing (or not) these activities.
Garcia del Castillo23 found in his study of university students that the psychosocial profile of the group with the highest frequency of Internet use showed a higher score in the “cognitive social skills” dimension (F=3.76, p=0.01), which indicates that there is a greater presence of “negative thoughts” in the group with the greatest frequency of use, interfering in different social situations. The presence of negative thoughts is associated with the use and abuse of the Internet in searching for “relationships and friendship” (r=0.14; p=0.016) and improving “emotional state” (r=0.16; p=0.007). These results agree with those of other authors who emphasize the tendency to escape, shyness and introversion, social phobia, and also, in contrast to the levels of neuroticism, self-confidence, self-reliance, or the search for feelings as personal characteristics associated with greater use and even abuse of the Internet, coinciding with our study regarding the highly significant correlation of IA with neuroticism-anxiety (rs=0.304, p<0.001), described as emotional instability, stress, worry, phobias and/or fears, obsessive indecision, and susceptibility to criticism. This also coincides with what some researchers think about the network; that it is a means of easy access for anonymous social interaction, thus constituting a space where communication can be less hampered by deficits in the ability of interpersonal relationships. It is important to remember that the network has become the medium for social development. In this sense it often does not eliminate social relations, only changes the means to develop or even generate emotional wellbeing in those with difficulties in face-to-face socialization. Therefore, we would have to rethink those items of interference in social life for the diagnosis of Internet abuse.
We agree with the conclusion of Salman et al.24, that psychiatrists and psychologists involved in the field of mental health must be well informed about mental problems due to Internet addiction, such as anxiety, depression, aggression, and employment and educational dissatisfaction, and consider that IA and its comorbid disorders should be properly evaluated and treated at the same time. Finally, it is also important to pay attention to Internet addiction in the treatment of people with these psychiatric disorders.
Because the participant sample is composed exclusively of university students, we could say that generalization of the results to the entire population is not possible because of their high cultural level. However, the results can generate some idea of what happens in the social group – namely, young individuals – who are being influenced by use of the Internet.
The means by which access to the Internet was achieved, including home computers, laptops or smart phones, were not taken into account in the study. This fact interferes with network access and facilitates more frequent, even problematic use. In addition, since the sample was medical students, they could have similar characteristics in lifestyle and personality. Therefore, research in other university groups could give a less biased idea of these characteristics.
ConclusionAlthough an association between IA and psychiatric symptoms exist, it may be beneficial for those with difficulty in establishing face-to-face relationships. Due to the prevalence of impulsivity and neuroticism/anxiety in people with Internet addiction, we think it would be prudent to better define the diagnostic criteria of addiction since impulsivity is related to other addictions and, in the case of Internet use, could be harmful. It is important to note that the Internet is a tool for various activities (research, education, socialization, and as a means of long-distance communication), which, used with control, does not cause any problems, but losing that control causes addiction and its comorbidities. Also, certain personality types are predisposed to this loss of control and abuse.
Conflicts of interestThe authors declare that they have no conflicts of interest and they received no funds for this work.
We thank Sergio Lozano-Rodríguez, M.D. for his help in translating the manuscript, Marco V. Gómez-Meza for his statistical advice and Ana E. Gutierrez Cortés for reviewing the manuscript.