



Acute calcific tendinitis of the longus colli muscle, also known as longus colli tendinitis and retropharyngeal tendinitis, is an aseptic inflammatory process characterised by neck pain, neck stiffness, and dysphagia, with or without odynophagia.
We present the case of a patient with sudden-onset dysarthria and dysphagia which were initially suspected to be of neurovascular origin.
The emergency department requested that the on-call neurologist assess a patient with dysarthria, sudden-onset dysphagia, and neck pain due to suspicion of vertebral artery dissection. The patient was a 60-year-old man with a history of tobacco use, arterial hypertension, dyslipidaemia, and primary hypothyroidism who visited the emergency department due to pain in the left side of his neck, dysphagia, odynophagia with solids and liquids, voice changes, and dysarthria, with onset upon awakening.
He reported no history of trauma, visual alterations, loss of strength, or sensory alterations. In the preceding days he had experienced no fever, dyspnoea, sialorrhoea, or upper respiratory tract infection, and did not report having swallowed a fish bone or other foreign body.
Upon arrival at hospital, the patient's blood pressure and respiratory frequency were normal. The neurological examination revealed mild dysarthria, mild nuchal rigidity, and severe neck pain upon mobilisation. He showed no dysfunction of the lower cranial nerves (IX, X, XI, and XII). A nasofibrolaryngoscopy performed during the otorhinolaryngological examination revealed a slight bulging of the left posterolateral pharyngeal wall. The larynx was erythematous and the vocal cords were smooth and mobile; no masses were observed.
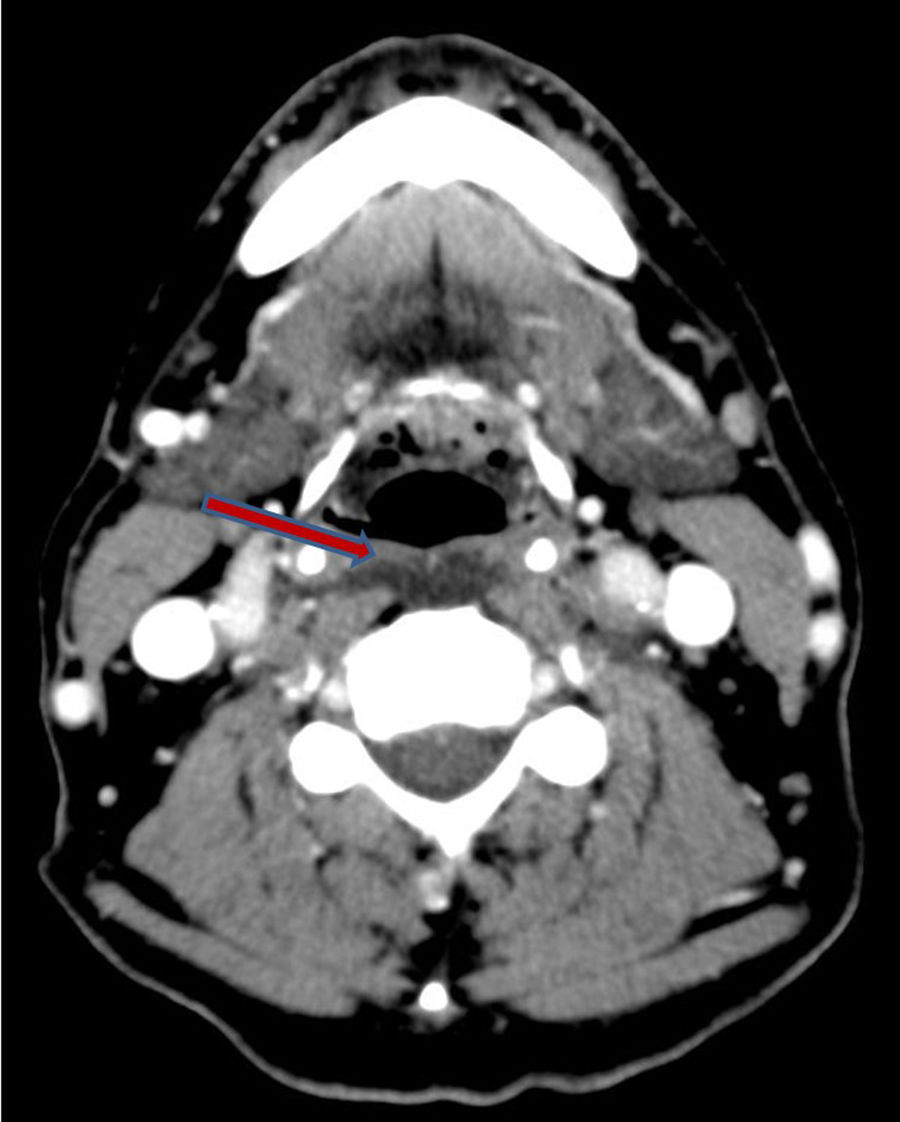
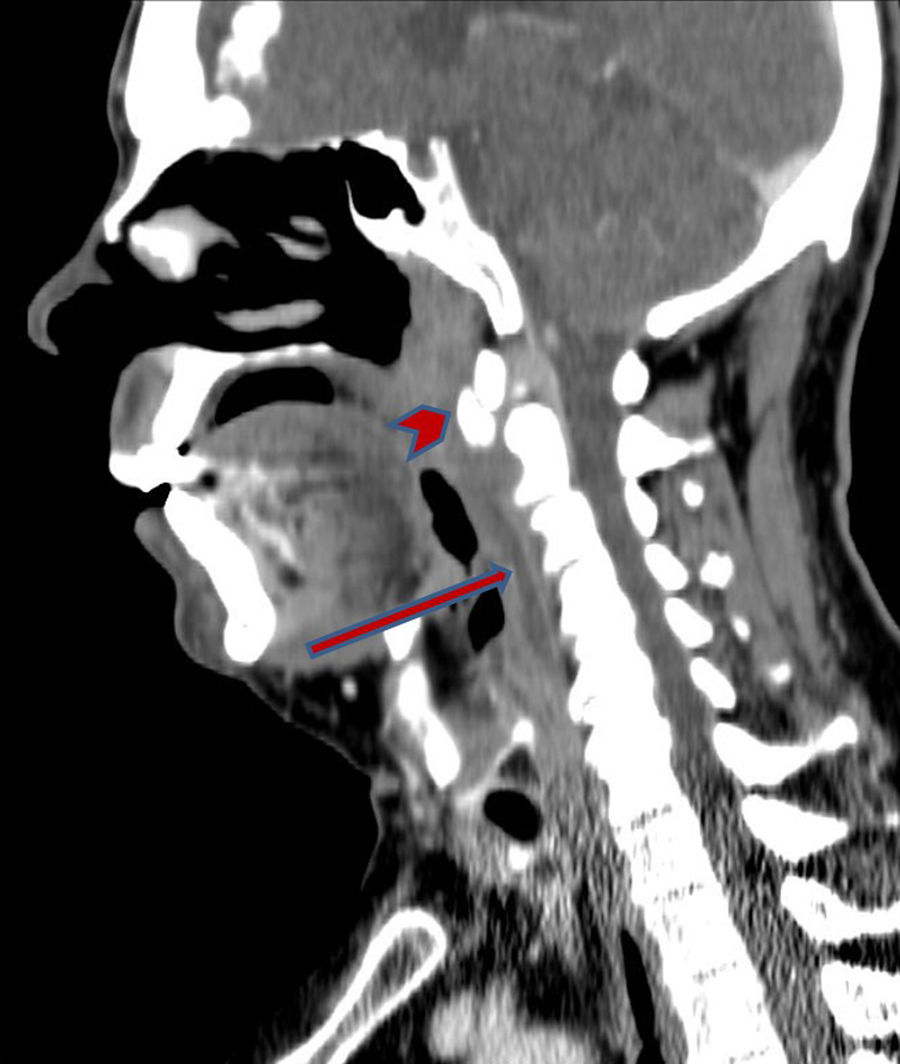
A neck CT scan with intravenous contrast showed a fluid collection in the prevertebral space, with no peripheral contrast uptake, extending from C2 to C5 and associated with calcification in the most cranial portion. These findings are compatible with longus colli tendinitis (Figs. 1 and 2).

 and calcification in the longus colli muscle at the C2 level (arrowhead).")
We started medical treatment with anti-inflammatory drugs, corticosteroids, relative rest, and local heat. Pain and dysphagia improved considerably within several hours; all symptoms resolved in 5 days.
First described by Hartley1 in 1964, longus colli tendinitis is characterised by a number of symptoms, including neck pain, neck stiffness, dysphagia, and odynophagia. Patients may also display mild leukocytosis, mild fever, and increased levels of such markers of inflammation as C-reactive protein or erythrocyte sedimentation rate.
Although the pathophysiology of the condition is not well understood, several trigger factors have been identified; these include recent trauma or a history of viral respiratory tract infection.2–4
Neuroimaging studies are essential, especially neck CT, which shows calcific deposits in the longus colli muscle, typically in the retropharyngeal space at the C1-C2 level, and prevertebral oedema of the soft tissues.5
It is crucial for neurologists and otorhinolaryngologists at emergency departments to be aware of this underdiagnosed entity. Differential diagnosis of longus colli tendinitis includes such severe neurological diseases as meningitis, spinal disc herniation, vertebral artery dissection, and spondylodiscitis, and other conditions that may be treated surgically, such as retropharyngeal abscess.6
The condition follows a benign clinical course, with treatment based on relative rest and the use of non-steroidal anti-inflammatory drugs, combined with opioids and corticosteroids in refractory cases. Symptoms usually resolve within 1-3 weeks.
We would like to thank Dr María Machío for her methodological advice and Dr Blanca Mateos for her clinical advice.
Please cite this article as: Oses M, Cubillos-del Toro L, Alcázar A, Herranz A. Tendinitis del tendón largo del cuello: un imitador inusual del ictus isquémico. Neurología. 2019;34:134–135.
