



Myasthenia gravis is associated with thymomas in approximately 10% of cases; surgery is the recommended treatment, except in cases of advanced age or poor general health. Spontaneous regression of thymomas is rare: according to our literature review, only 9 cases have been reported1–5; 7 of these were reported in Japan and most cases were women. Only one of these patients also had myasthenia gravis.2
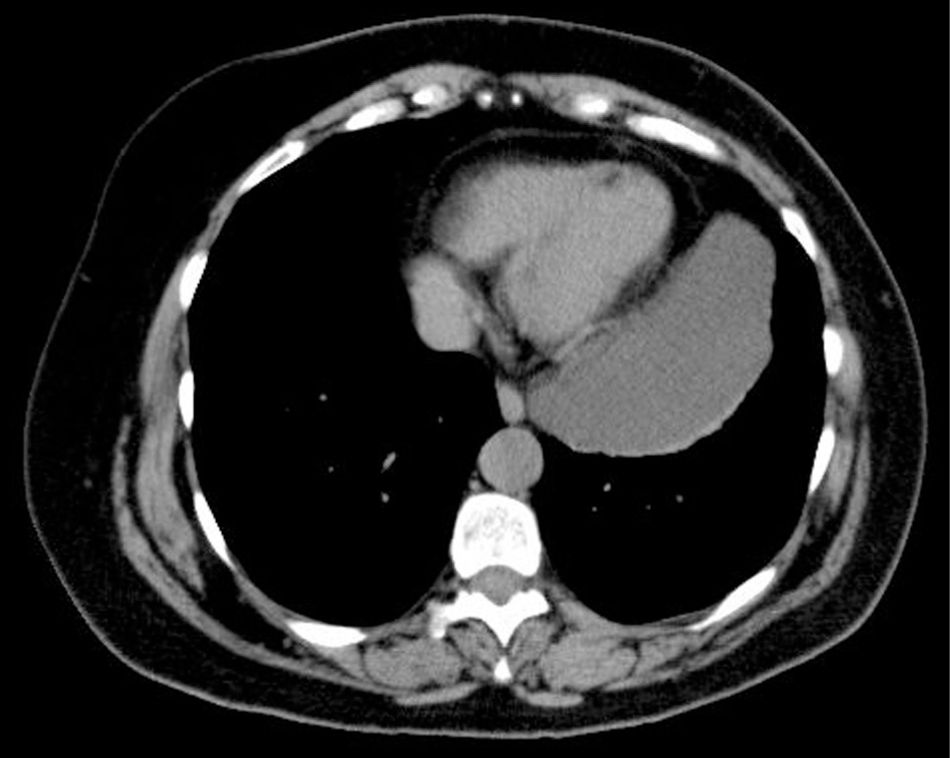
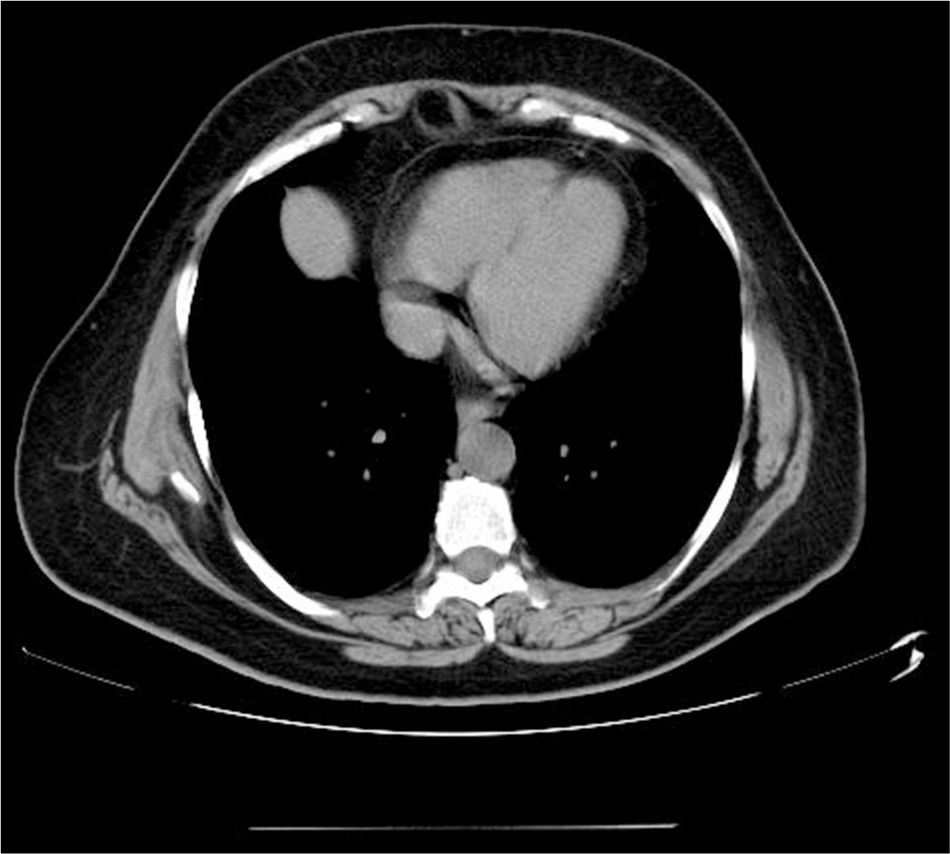
We present the case of a 55-year-old woman who was diagnosed with generalised myasthenia gravis (Osserman type IIb) based on the presence of acetylcholine receptor antibodies. A chest CT scan performed in October 2010 revealed a homogeneous mass in the left side of the anterior mediastinum measuring 111×58×167mm; there was no mass infiltration (Fig. 1). The CT scan also revealed small adenopathies in the inferior paratracheal area plus another in the aortopulmonary window; these findings were consistent with thymoma. The patient started treatment with pyridostigmine dosed at 60mg/8hour and prednisone dosed at 60mg/day; the dose was progressively decreased the following month. Resection of the thymoma was suggested, but the patient refused surgery. Medical treatment achieved clinical stabilisation, but the patient experienced a relapse after withdrawal of corticosteroid treatment. Prednisone achieved stabilisation; we further administered azathioprine dosed at 150mg/day, which enabled prednisone to be withdrawn. The patient progressed favourably; she experienced mild fatigability but could independently perform the activities of daily living. A second CT scan was performed one year later, revealing that the mass had decreased considerably. One year after onset of treatment with azathioprine, the patient had experienced no further relapses and recovered progressively until she was nearly asymptomatic. A subsequent follow-up CT scan performed recently showed that the mass had disappeared completely (Fig. 2).
×58mm (transverse)×167mm (vertical).")

The real rate of spontaneous thymoma regression is unknown since most thymomas are surgically removed. The mechanism underlying the process is still to be determined. In our patient, symptoms progressed favourably with tumour regression. Complete tumour regression has been reported in only one of the 9 cases published4; the other patients underwent thymectomy. Radiological follow-up may be an alternative to surgery in certain cases.
Although we have no histopathological data from our patient, we were surprised to find complete spontaneous regression of a mass of such dimensions.
Please cite this article as: Modrego PJ, Arribas J. Resolución espontánea de una masa mediastínica en una mujer con miastenia gravis. Neurología. 2018;33:556–557.
