





Congenital anomalies of the pulmonary arteries are uncommon. They can occur in isolation or in association with congenital heart defects. Isolated congenital anomalies remain undiscovered until they are reported as incidental findings on imaging tests, usually not until adolescence. We review the embryological development and normal anatomy of the pulmonary arteries as well as the spectrum of computed tomography findings for various congenital anomalies: unilateral interruption of the pulmonary artery, anomalous origin of the left pulmonary artery (pulmonary artery sling), idiopathic aneurysm of the pulmonary artery, and other anomalies associated with congenital heart defects.
ConclusionCongenital anomalies of the pulmonary arteries represent a diagnostic challenge for clinicians and radiologists. Computed tomography is useful for their diagnosis, and general radiologists need to be familiar with their imaging appearance because they are often discovered incidentally.
Las anomalías congénitas de las arterias pulmonares (AP) son poco frecuentes y pueden presentarse aisladas o asociadas a defectos cardiacos congénitos. En general, si son aisladas, suelen pasar clínicamente inadvertidas hasta la adolescencia y ser un hallazgo incidental en exploraciones radiológicas. Nuestro objetivo es revisar las bases embriológicas del desarrollo de las AP, su anatomía normal y el espectro de hallazgos por tomografía computarizada (TC) de sus anomalías congénitas, en concreto la interrupción unilateral de la AP, el origen anómalo de la AP izquierda (sling pulmonar), el aneurisma idiopático de la AP y otras anomalías asociadas a defectos cardiacos congénitos. Las anomalías congénitas de las AP representan un reto diagnóstico, tanto clínico como radiológico. La TC es una herramienta útil en su diagnóstico y el radiólogo general debe estar familiarizado con su apariencia, ya que pueden ser un hallazgo incidental.
Congenital anomalies of pulmonary arteries (PA) are usually associated to other congenital heart defects and they do not usually occur in isolation. Although they can result in symptoms during childhood, the PA isolated anomalies usually go unnoticed until adolescence or early adult age.1,2
The imaging diagnosis of PA anomalies are challenging both for the clinician and the radiologist since conventional image modalities like X-rays and ultrasounds have a limited value when it comes to detection and characterization, while the pulmonary angiography is an invasive method usually reserved for cases that require treatment. This is the reason why both the computed tomography (CT) and magnetic resonance imaging (MRI) play an essential role in the study of PA. In part thanks to the possibility of generating particular multiplanar and volumetric reconstructions the angio-CT offers great advantages in the diagnosis and follow-up of these anomalies making the characterization of the vascular and valvular anatomies possible as well as any other associated findings in other organs. Also these reconstructions facilitate the communication of findings and the understanding of the anatomy for an optimal surgical plan.
The goal of this paper is to review the embyological basis for the development of PA, the PA normal anatomy and image findings of PA congenital anomalies—especially the unilateral interruption of PA, the anomalous origin of the left PA (pulmonary sling), the main PA idiopathic aneurysm and other anomalies associated with congenital heart anomalies.
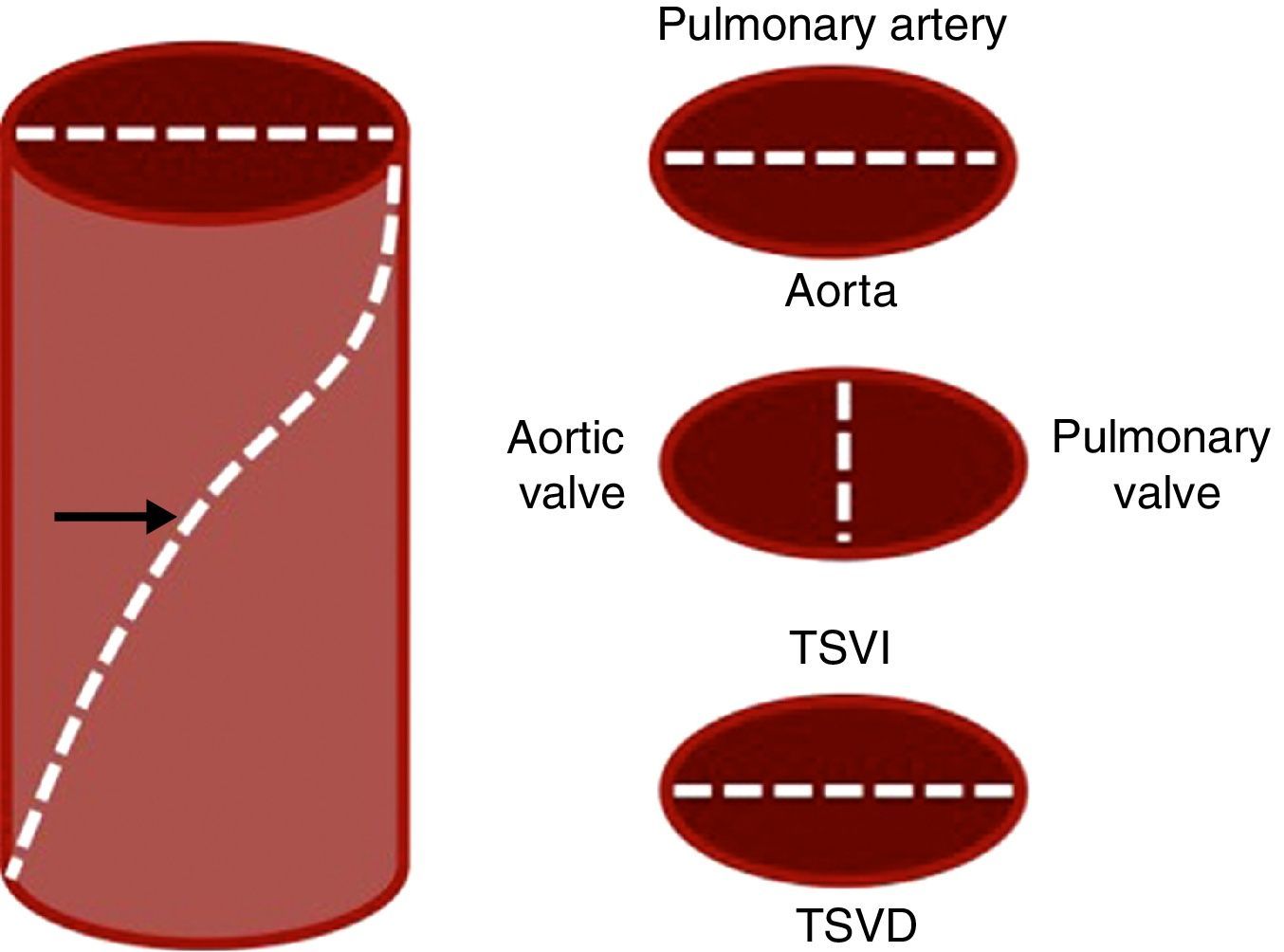
Embryological basisAfter the formation of the cardiac tube and its differentiation into primitive segments that give rise to cardiac structures the arterial trunk gives rise to the aorta and the proximal section of the PA.3 During the fifth week of embryonic life the aortopulmonary septum is created in a spiral-like shape that splits the truncus arteriosus into aorta and PAs (Fig. 1).
. The aortopulmonary septum (arrow) shows a spiral disposition and divides the arterial trunk into aorta and pulmonary aorta as well as the aortic and pulmonary valves while dividing the outflow track of both ventricles inferiorly. RVOT: right ventricle outflow track; LVOT: left ventricle outflow track.")
Embryonic development of pulmonary artery. Schematic illustration of the arterial trunk (left). The aortopulmonary septum (arrow) shows a spiral disposition and divides the arterial trunk into aorta and pulmonary aorta as well as the aortic and pulmonary valves while dividing the outflow track of both ventricles inferiorly. RVOT: right ventricle outflow track; LVOT: left ventricle outflow track.
Thus the trunk of the pulmonary artery is derived into the truncus arteriosus. The proximal sections of the sixth bilateral aortic arches make up the right and left Pas.4 The distal sections of the PAs are derived from primitive buds that come from these arches and grow toward the inside of lung buds (the origin of lungs) to later anastomose with them.
We should remember that: since the embryonic lung morphogenesis is a process parallel to the airway branching morphogenesis,4 it is not rare to find a combination of vascular and bronchial tree anomalies.
The anatomy of pulmonary arteriesThe PA trunk stems from the right ventricle and bifurcates into the main right and left PAs. The pulmonary valve is made up of three valvular sinuses and can be found in the proximal section of the pulmonary trunk—the pulmonary root.5
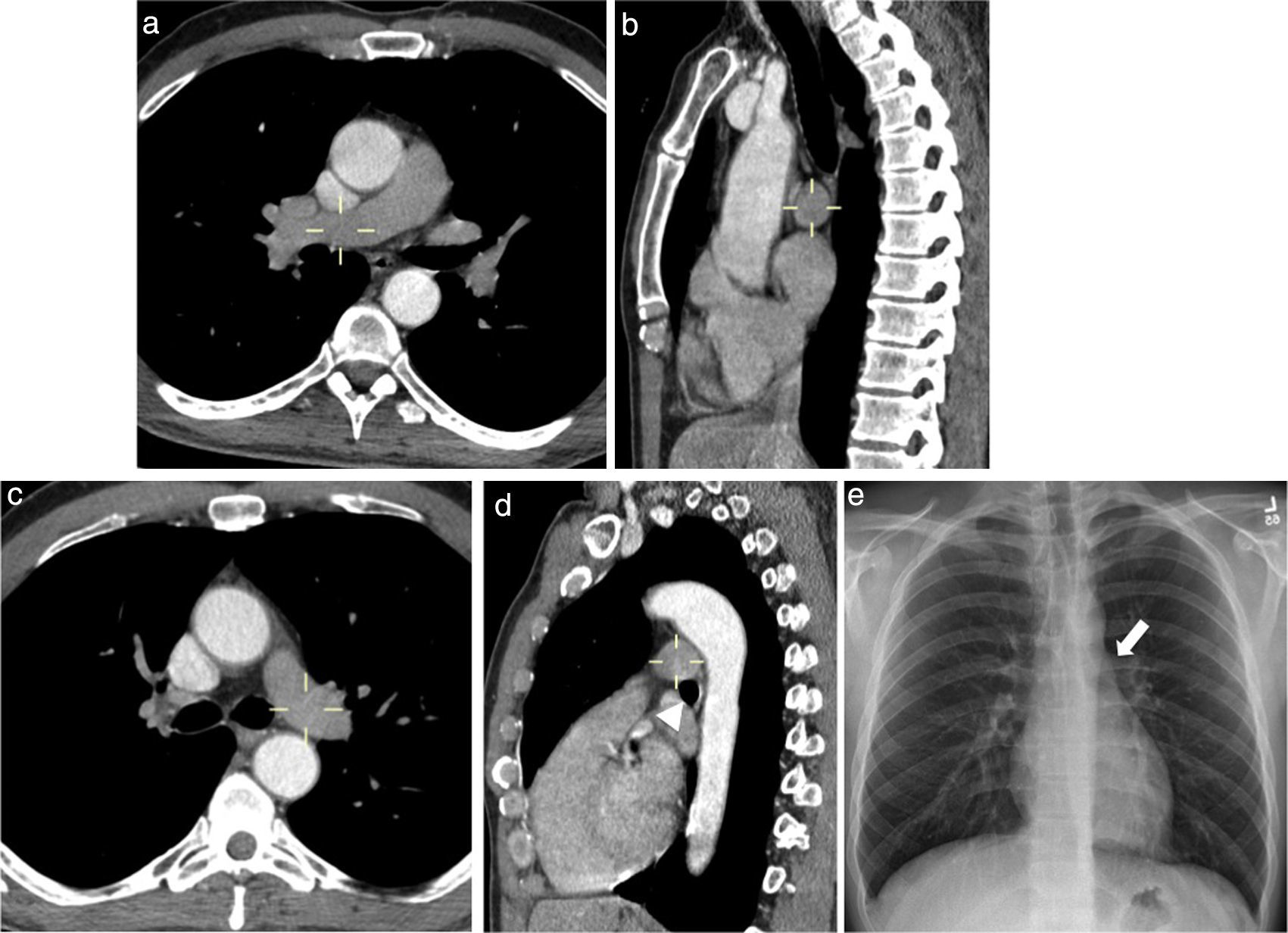
The maximum diameter of the adult pulmonary trunk is 28mm.6 The right and left PAs show an intrapericardial trajectory before bifurcating into the lobar arteries in every side. Because of the special location of the pulmonary trunk—left to the middle line, the intrapericardial segment of the right PA is longer ant its bifurcation occurs at pulmonary root level. The right PA is located under the right upper lobar bronchus (hypobronchial) laterally following the intermediate bronchus (Fig. 2a and b). The distal left PA resides in an epibronchial location (superior to the left main bronchus) and keeps a posterior location to the bronchus until it bifurcates into the left lobar arteries (Fig. 2c–e). Both PAs should be of a similar caliber.
 has an inferior location with respect to the main right bronchus. The left pulmonary artery (marker in c and d) has a superior location with respect to the main left bronchus (arrowhead in d) and is the culprit of the higher position of the left pulmonary hilum in the normal thoracic X-ray (arrow in e).")
Normal anatomy of pulmonary arteries. The right pulmonary artery (marker in a and b) has an inferior location with respect to the main right bronchus. The left pulmonary artery (marker in c and d) has a superior location with respect to the main left bronchus (arrowhead in d) and is the culprit of the higher position of the left pulmonary hilum in the normal thoracic X-ray (arrow in e).
The central axial interstice area—a network of connective tissue supporting the pulmonary structures reaches out from the pulmonary hila while surrounding the PAs and the main bronchi—reaching out distally as they originate lobar, segmental and sub-segmental branches. Both the arteries and the bronchi are therefore one single bronchovascular package and have a similar diameter.
Congenital anomalies of pulmonary arteriesThe congenital anomalies of PAs are usually associated with other congenital heart defects such as Fallot's tetralogy. The isolated anomalies of PAs are a very select less common group made up of four main anomalies each and everyone of them with defined anatomic characteristics.
Unilateral absence of pulmonary arteryAlso known as proximal interruption of the PA since the distal section of the artery inside the pulmonary parenchyma is usually intact due to its different embryonic origin.3,6 The congenital interruption of PA is uncommon (reported in one of every 200,000 individuals7) and it is thought to be due to an abnormal involution of the proximal section of the sixth primitive aortic arch with a higher frequency in the right side.3,8,9
We should remember that: when the homolateral lung is present—at times formed partially or rudimentary the pulmonary perfusion is provided by systemic collaterals mainly bronchial arteries and intercostal arteries through transpleural branches, the internal mammary artery, the subclavian artery or the brachiocephalic trunk (Figs. 3 and 4). The affected PA can be totally absent or end 1cm away from its origin, while the aortic arch is usually contralateral to the affected artery (Fig. 4).
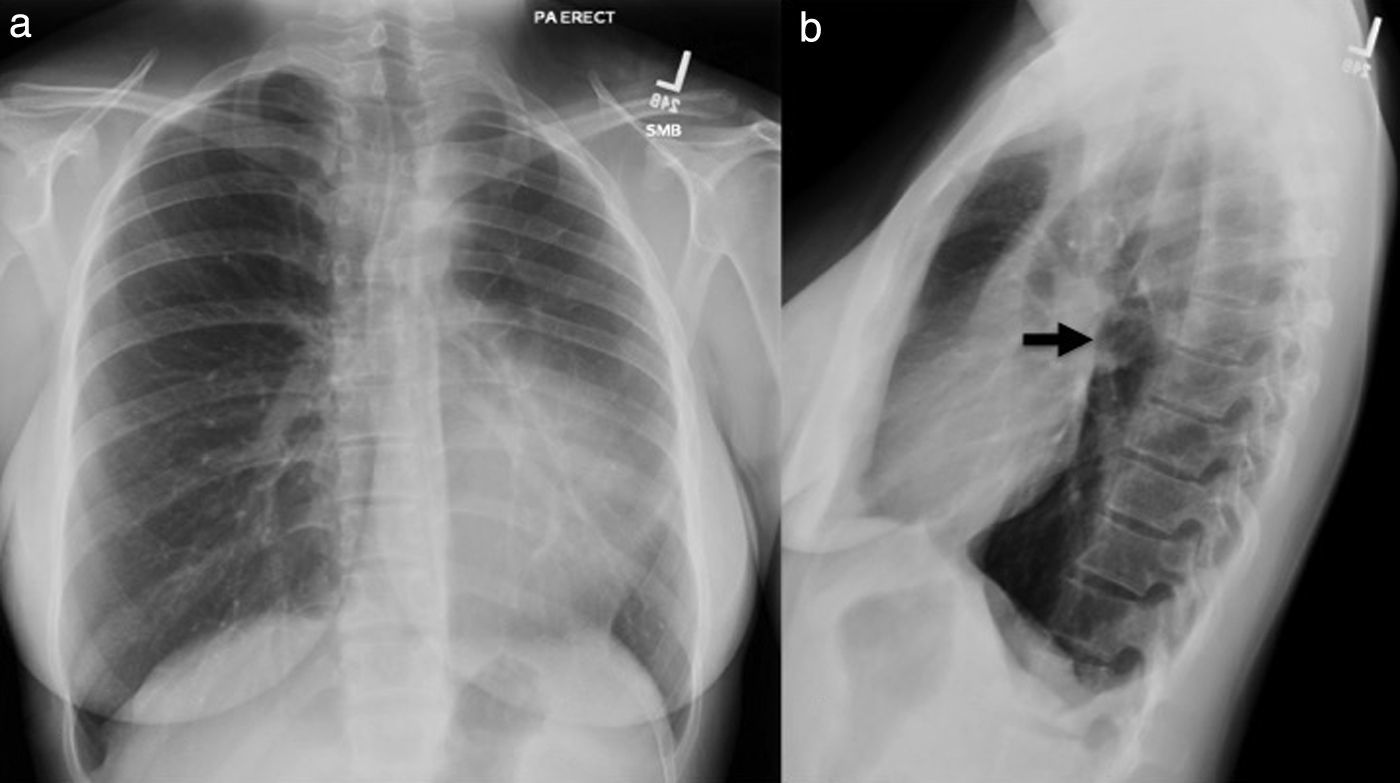
 and lateral projections of PA (b) showing deviation of the mediastinum to the left accompanied by a reduced left pulmonary volume (a). In the lateral X-ray (b) we can see what looks like an abnormal looking left pulmonary hilum (arrow) without any circular lucency so typical of the main left lobe bronchus due to a partial congenital absence of the pulmonary artery on this side. The X-ray does not show pneumonic consolidation.")
Eighteen-year-old female with suspicion of pneumonia. Thoracic X-ray; posterior-anterior (a) and lateral projections of PA (b) showing deviation of the mediastinum to the left accompanied by a reduced left pulmonary volume (a). In the lateral X-ray (b) we can see what looks like an abnormal looking left pulmonary hilum (arrow) without any circular lucency so typical of the main left lobe bronchus due to a partial congenital absence of the pulmonary artery on this side. The X-ray does not show pneumonic consolidation.
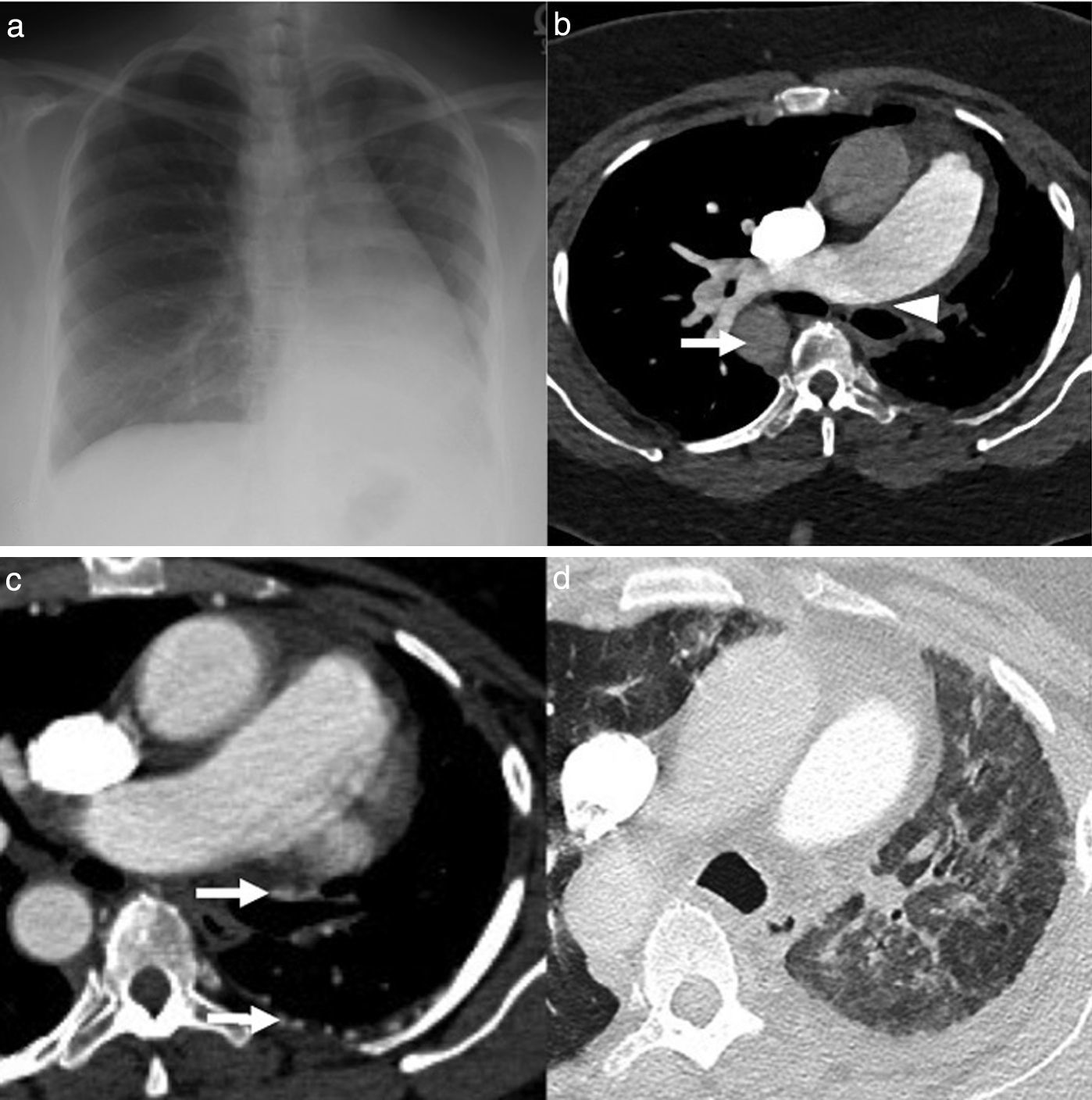
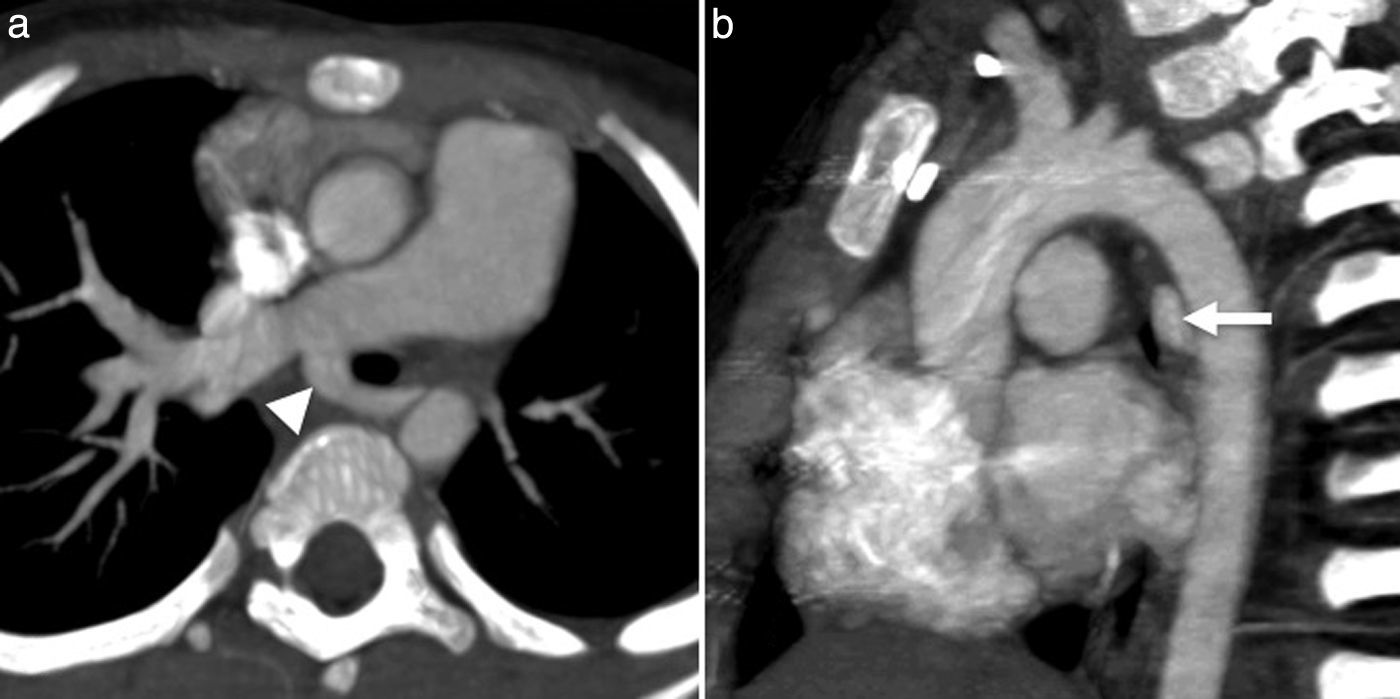
 showing loss of left pulmonary volume and mediastinic deviation to the left as well as right aortic arch (arrow). The angio-CT axial images (b–d) confirm the congenital absence of the left pulmonary artery (arrowhead) from its origin (b). The descending thoracic aorta is located to the right (arrow in b). Pulmonary perfusion is provided by bronchial and intercostal dilated arteries (arrows in c). In the pulmonary window (d) we can see left lung hyperplasia showing diffuse attenuation in polished glass and interlobular septal thickening. Subpleural reticulation is due to perfusion provided by transpleural branches from intercostal arteries (arrow).")
Fifty year old asymptomatic female. Posterior-anterior thoracic X-ray (a) showing loss of left pulmonary volume and mediastinic deviation to the left as well as right aortic arch (arrow). The angio-CT axial images (b–d) confirm the congenital absence of the left pulmonary artery (arrowhead) from its origin (b). The descending thoracic aorta is located to the right (arrow in b). Pulmonary perfusion is provided by bronchial and intercostal dilated arteries (arrows in c). In the pulmonary window (d) we can see left lung hyperplasia showing diffuse attenuation in polished glass and interlobular septal thickening. Subpleural reticulation is due to perfusion provided by transpleural branches from intercostal arteries (arrow).
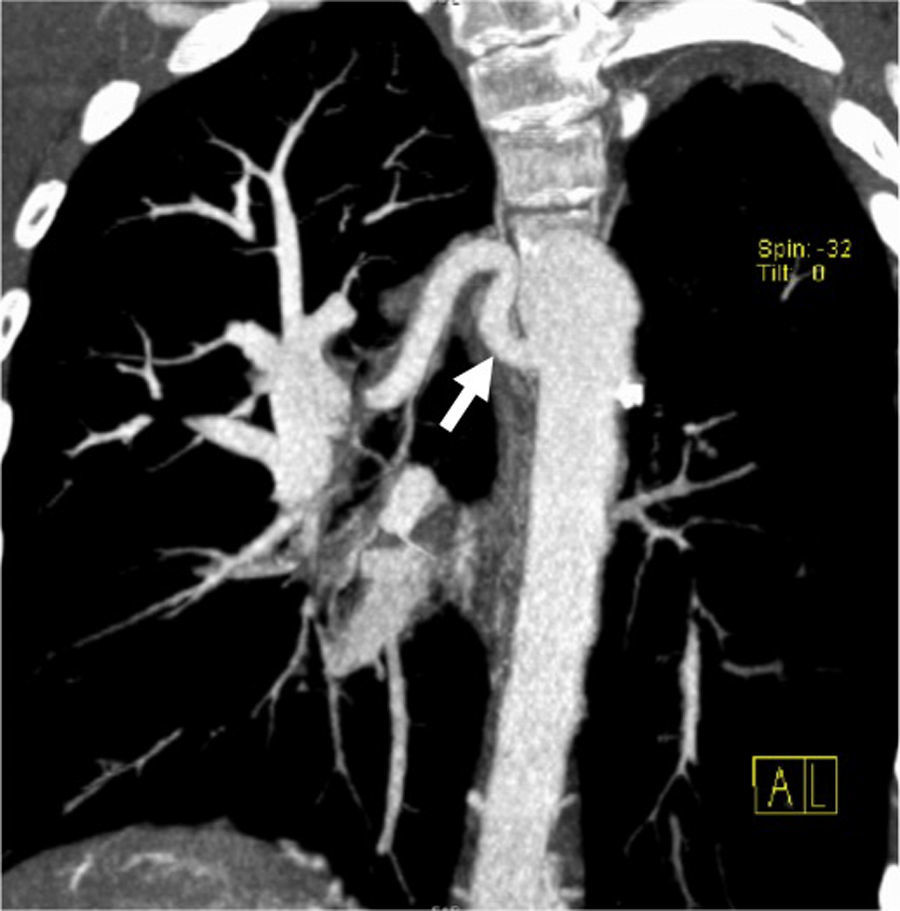
The aberrant disposition of the left pulmonary artery is due to its abnormal origin from the right pulmonary artery and is called pulmonary sling due to its abnormal trajectory across the tracheoesophageal space (Fig. 5). This anomaly is due to an abnormal process of involution of the sixth left proximal aortic arch.7,10,11 It usually occurs with respiratory distress or repetitive pulmonary infections.12,13
 reconstruction, axial (a) and sagittal (b) images showing the abnormal origin of the left PA from the right PA (a), and an abnormal retrotracheal trajectory toward the left pulmonary hilum (arrowhead). The sagittal MIP reconstruction (b) shows the abnormal position of the left pulmonary artery, posterior to the main left bronchus (arrow).")
Five-year-old male with stress dyspnea. Angio-CT, maximum intensity projection (MIP) reconstruction, axial (a) and sagittal (b) images showing the abnormal origin of the left PA from the right PA (a), and an abnormal retrotracheal trajectory toward the left pulmonary hilum (arrowhead). The sagittal MIP reconstruction (b) shows the abnormal position of the left pulmonary artery, posterior to the main left bronchus (arrow).
We should remember that: the abnormal associated tracheal or bronchial segmentation (supernumerary bronchus, tracheal bronchus, tracheobronchial stenosis) subcategorizes these patients into a group with higher rates of mortality or morbidity6 (Fig. 6).
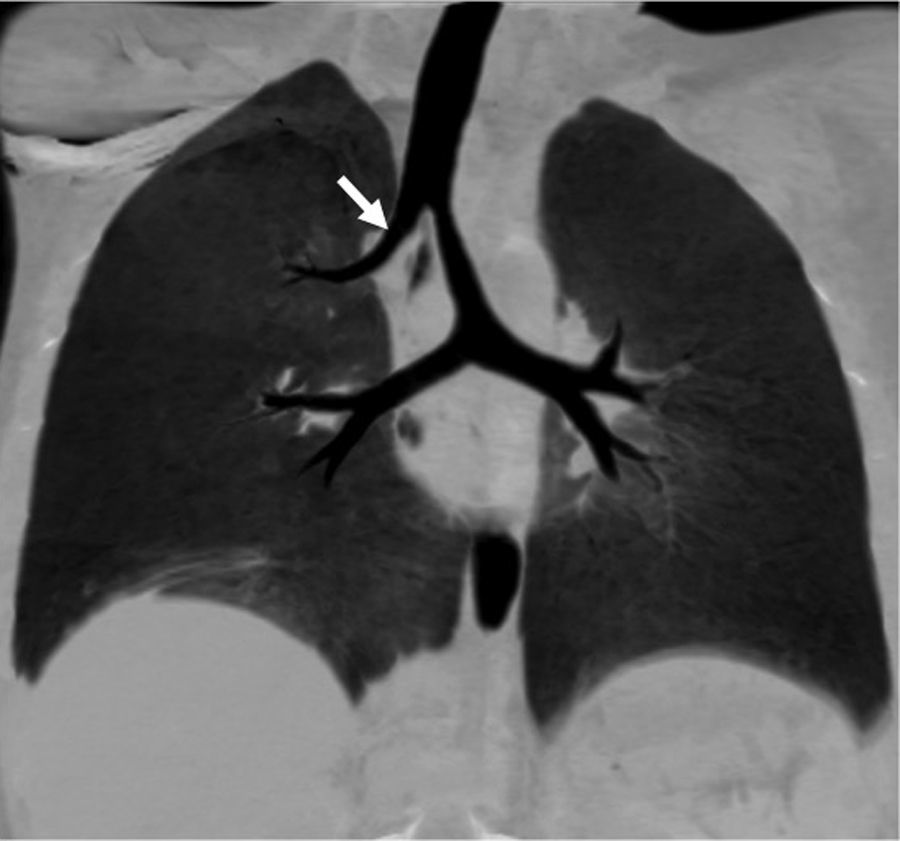
 with anomalous origin of left pulmonary artery or pulmonary sling. Coronal reconstruction in minimum intensity projection (MinIP) showing abnormal segmentation of the tracheobronchial tree. The bronchus for the right upper lobe stems directly from the trachea (tracheal bronchus) (arrow). In this case there are no stenosed areas.")
Five-year-old male (same patient from Fig. 5) with anomalous origin of left pulmonary artery or pulmonary sling. Coronal reconstruction in minimum intensity projection (MinIP) showing abnormal segmentation of the tracheobronchial tree. The bronchus for the right upper lobe stems directly from the trachea (tracheal bronchus) (arrow). In this case there are no stenosed areas.
The idiopathic dilation of the trunk of the PA is a rare condition that usually affects the pulmonary trunk in isolation (Fig. 7), but can reach out the left or right pulmonary arteries. Even though it can occur in isolation, the aneurysms of the PA are usually associated with other congenital heart anomalies.17
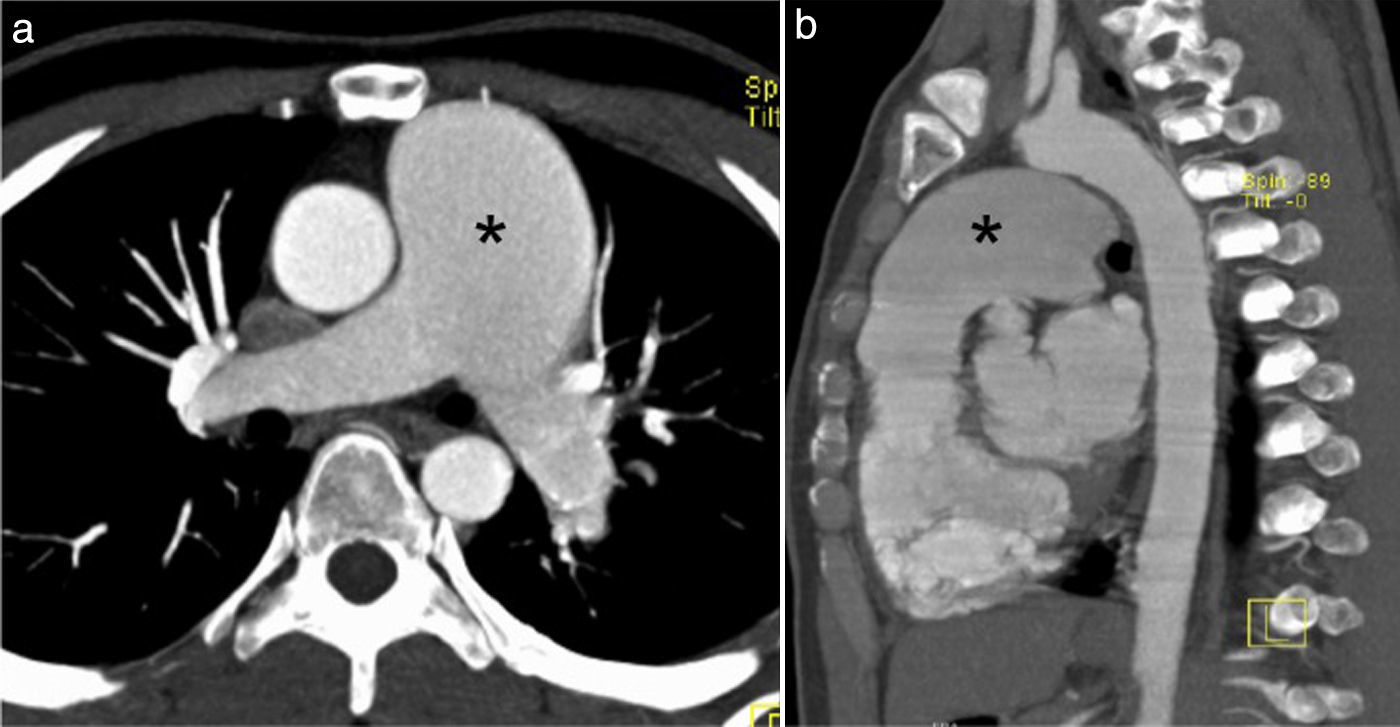
 and CT sagittal reconstruction (b) with contrast showing massive dilation of the main left pulmonary artery (asterisk) that measures 45mm. Right and left pulmonary arteries of normal caliber. In this case the pulmonary valve was competent.")
Asymptomatic sixteen-year-old male. Axial image (a) and CT sagittal reconstruction (b) with contrast showing massive dilation of the main left pulmonary artery (asterisk) that measures 45mm. Right and left pulmonary arteries of normal caliber. In this case the pulmonary valve was competent.
The exact etiology is not fully established but it is thought to be due to the weakness of the middle elastic layers of the arterial wall14—suggestive of a similar physiopathology to that of aortic aneurysms.
The diagnosis is achieved when there is dilation of the trunk of the pulmonary artery (>30mm) and intracardiac or extracardiac shunts, pulmonary disease or chronic heart disease, vascular disease and pulmonary artery hypertension.15
We should remember that: the pulmonary valve disease is a finding associated with the idiopathic aneurysm of the PA16,17—usually accompanied by valve heart failure. Even though the development of symptoms due to pulmonary valve failure can lead to an early diagnosis, most these patients are usually asymptomatic until old age and can be diagnosed incidentally.
Other anomalies associated to congenital heart defectsOther congenital anomalies like pulmonary valve stenosis (Fig. 8), atresia, hypoplasia or segmental stenosis of the PA, or the anomalous origin of the PAs from the aorta are more common than the isolated cases and they are associated with other congenital heart defects like the double outflow tract of the right ventricle and Fallot's tetralogy.
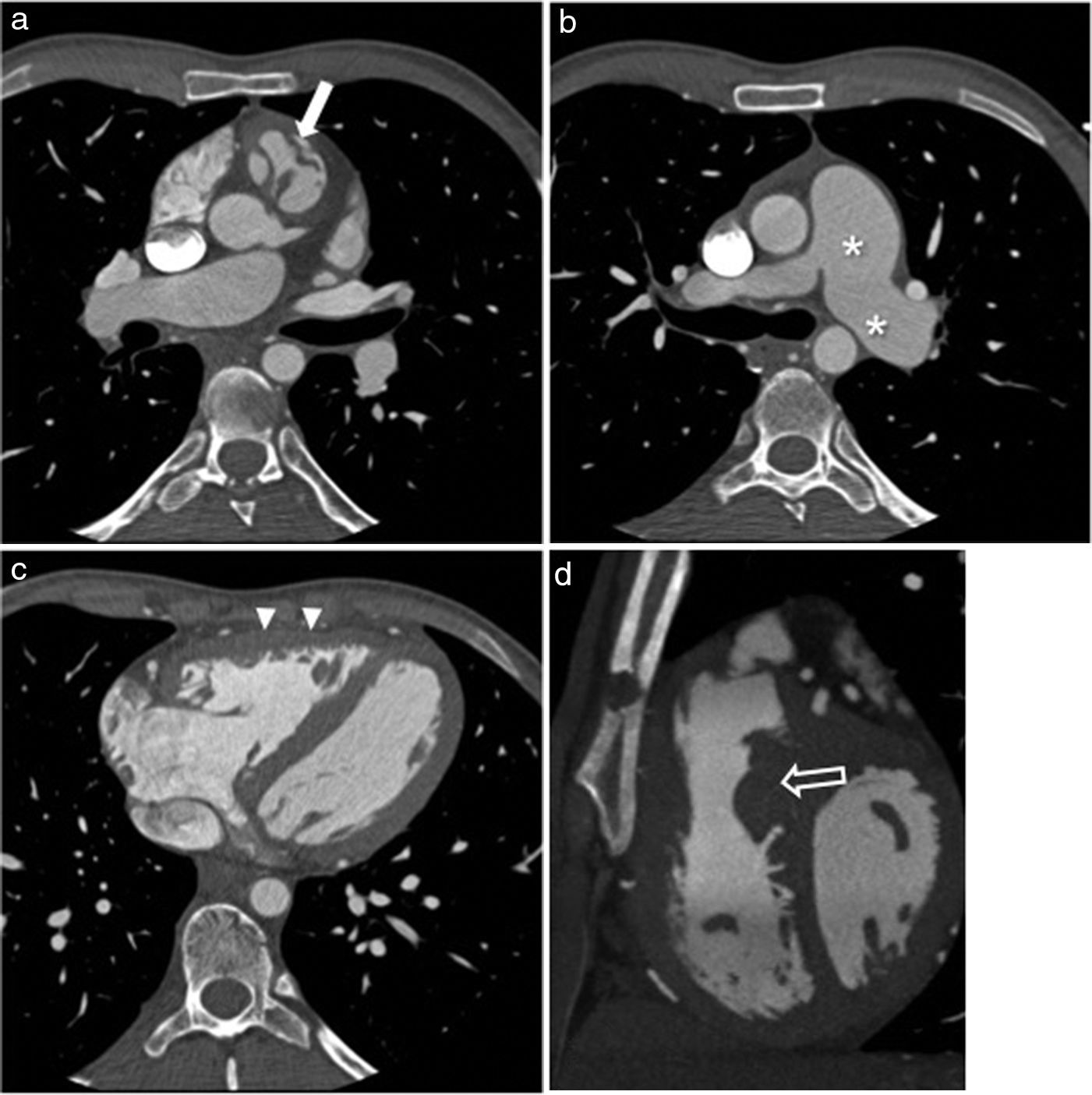
 and oblique sagittal reconstruction (d) showing pulmonary valve thickening (arrows in a) and dilation typical of the pulmonary trunk and left pulmonary artery (asterisk in b) showing post-stenotic dilation. Right ventricle in the borderline threshold of normalcy with marked hypertrophy (arrowheads). We can also see infundibular hypertrophy (hollow arrow) conditioning the added subvalvular stenosis.")
Thirty-two-year old male with serious stenosis of his pulmonary valve and moderate failure. Angio-CT images – axial images (a–c) and oblique sagittal reconstruction (d) showing pulmonary valve thickening (arrows in a) and dilation typical of the pulmonary trunk and left pulmonary artery (asterisk in b) showing post-stenotic dilation. Right ventricle in the borderline threshold of normalcy with marked hypertrophy (arrowheads). We can also see infundibular hypertrophy (hollow arrow) conditioning the added subvalvular stenosis.
The combination of an abnormal position (cephalic and anterior) of the aortopulmonary septum and hypertrophy of the septo-parietal trabeculations of the right ventricle are the cause for the outflow tract obstruction of the right ventricle that is so characteristic of Fallot's tetralogy.18 This is characteristically associated with variable degrees of outflow tract obstruction of the right ventricle with infundibular stenosis or pulmonary valve stenosis (or both). Pulmonary atresia in extreme cases of Fallot's tetralogy and trunk stenosis of the pulmonary artery (Fig. 9) or its branches are associated findings too.19 The seriousness of the patient's symptoms and the surgical plan are initially determined by the degree of obstruction to pulmonary flow. In serious cases of Fallot's tetralogy there is pulmonary atresia (extreme Fallot or arterious pseudo trunk) with a complete absence of the main pulmonary artery and pulmonary circulation replaced by aortopulmonary collateral circulation or thoracic arteries stemming directly from the descending aorta (Fig. 10).


Eleven-year-old female with a history of Fallot's tetralogy and pulmonary atresia (arterious pseudo-trunk). Coronal reconstruction with MIP showing one aortopulmonary collateral of large caliber (arrow) that provided arterial flow to the right lung due to complete obstruction of the right ventricle outflow tract so typical of this condition.
Angio-CT is an excellent tool for both preoperative and postoperative assessments since it allows us to diagnose complications such as stenoses or pulmonary residual obstructions (that can affect the outflow tract of the right ventricle all the way to the pulmonary branches—surgical ducts included (Fig. 11), outflow tract aneurysms of the right ventricle and defects at residual interventricular septum level (Fig. 12).

Seventeen-year-old male with a history of Fallot's tetralogy and pulmonary stenosis corrected through angioplasty. Volumetric (a) and multiplanar reconstructions in oblique planes showing calcification and serious stenosis also affecting the right ventricle outflow tract and the pulmonary trunk (arrows in b). Also stenosis is evident in the proximal section of both main pulmonary arteries above all the left one where one intimal flap of skin (hollow arrow) can be seen probably due to dissection secondary to a prior angioplasty (c). Dilation of the right ventricle (asterisk) can be seen too.

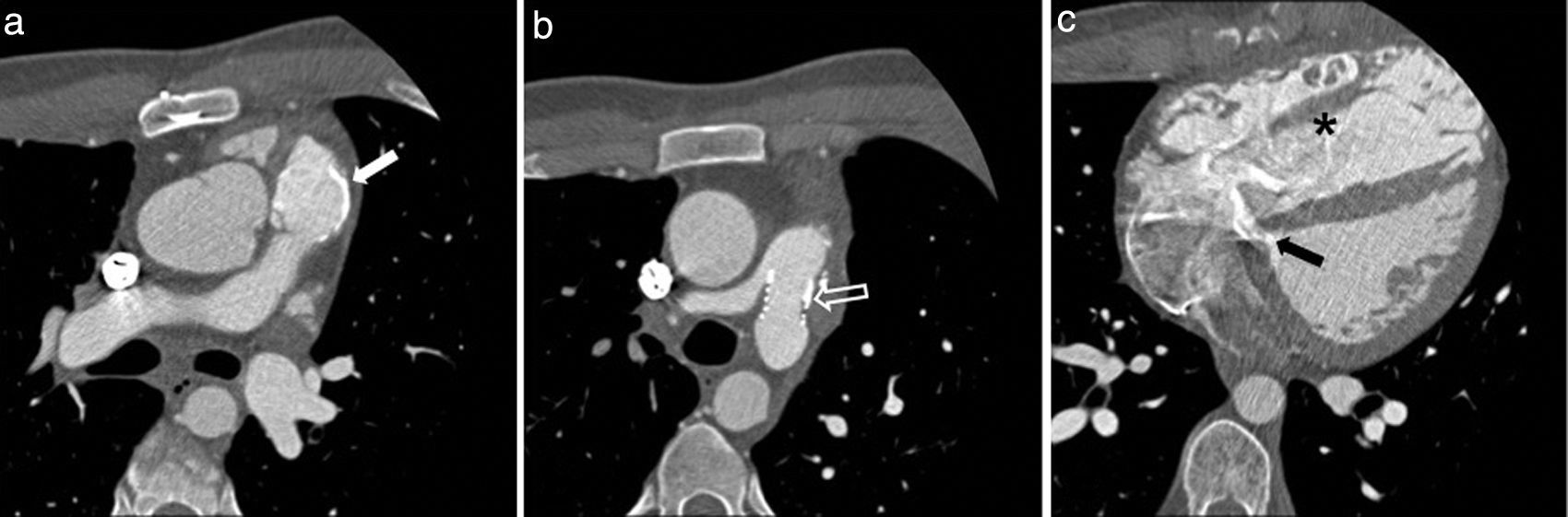
Sixteen-year-old male with a history of Fallot's tetralogy corrected through transannular patch during his infancy and further stenosis of left pulmonary artery corrected through stent implantation. The patient was asymptomatic yet the ultrasound showed serious pulmonary failure. Angio-CT axial images showing calcification (arrow in a) of dilated transannular ring and left pulmonary artery with patent stent (hollow arrow) of normal caliber (b). We can also see a significant dilation of the left ventricle (asterisk in c) and residual interventricular septum defects (black arrow).
Dilation and right ventricular dysfunction – usually due to pulmonary valve failure as the result of transannular patch can also be assessed through cardiac CT with electrocardiographic synchronization which is considered an alternative to cardiac magnetic resonance imaging (MRI) in cases where it is not recommended such as in patients with pacemakers.20,21
ConclusionsThe congenital anomalies of the PAs can be asymptomatic until old age and be challenging when it comes to a correct diagnosis. Finding them and characterizing them through transthoracic echocardiography (TTE) or X-ray is complex and this is the reason why the angio-CT is an essential modality that allows us to characterize the vascular and valvular anatomies of these conditions as well as any associated findings in other organs. It is important for the radiologist to know this spectrum of anomalies since incidental diagnoses are not uncommon.
Ethical responsibilitiesProtection of people and animalsThe authors declare that no experiments with human beings or animals have been performed while conducting this investigation.
Confidentiality of dataThe authors confirm that in this article there are no data from patients.
Right to privacy and informed consentThe authors confirm that in this article there are no data from patients.
Authors- 1.
Manager of the integrity of the study: JB, LF, MM.
- 2.
Study Idea JB, LF, MM.
- 3.
Study Design: JB, LF, MM.
- 4.
Data Mining: JB, LF, MM.
- 5.
Data Analysis and Interpretation: JB, LF, MM.
- 6.
Statistical Analysis: N/A.
- 7.
Reference: JB, LF.
- 8.
Writing: JB, LF, MM.
- 9.
Critical review of the manuscript with intellectually relevant remarks: JB, LF, MM.
- 10.
Approval of final version: JB, LF, MM.
The authors declare no conflict of interests associated with this article whatsoever.
Please cite this article as: Bueno J, Flors L, Mejía M. Anomalías congénitas de las arterias pulmonares: espectro de hallazgos en tomografía computarizada. Radiología. 2017;59:209–217.

