



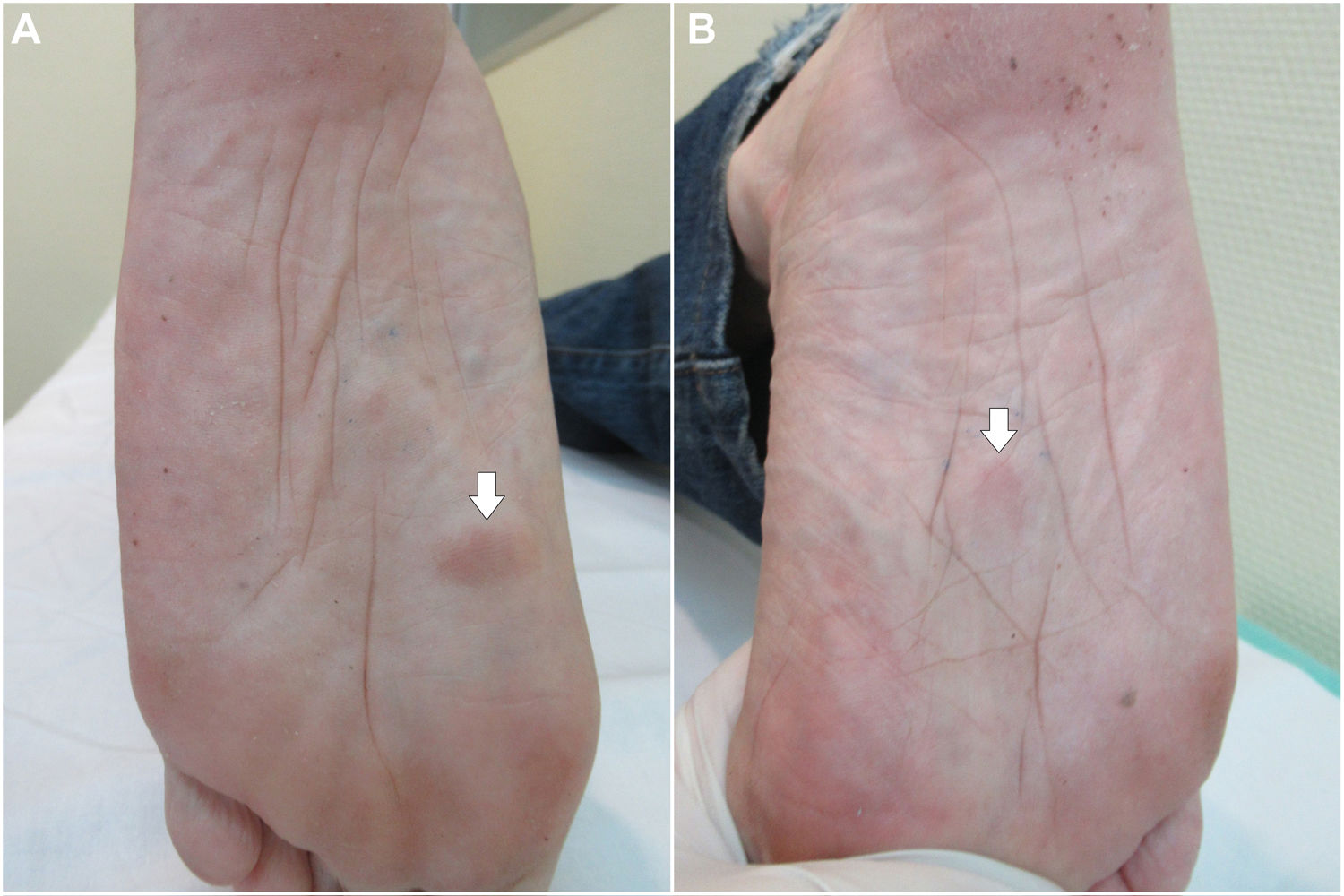
We present the case of a 66-year-old man with a history of smoking (102 packs per year) and alcohol use. This man sought care due to some asymptomatic subcutaneous tumours which had been present for the past year on the soles of his feet. Physical examination revealed firm nodules adhered to deep planes (Fig. 1A-1B).
 Soles of both feet on which nodules can be seen (arrows).")
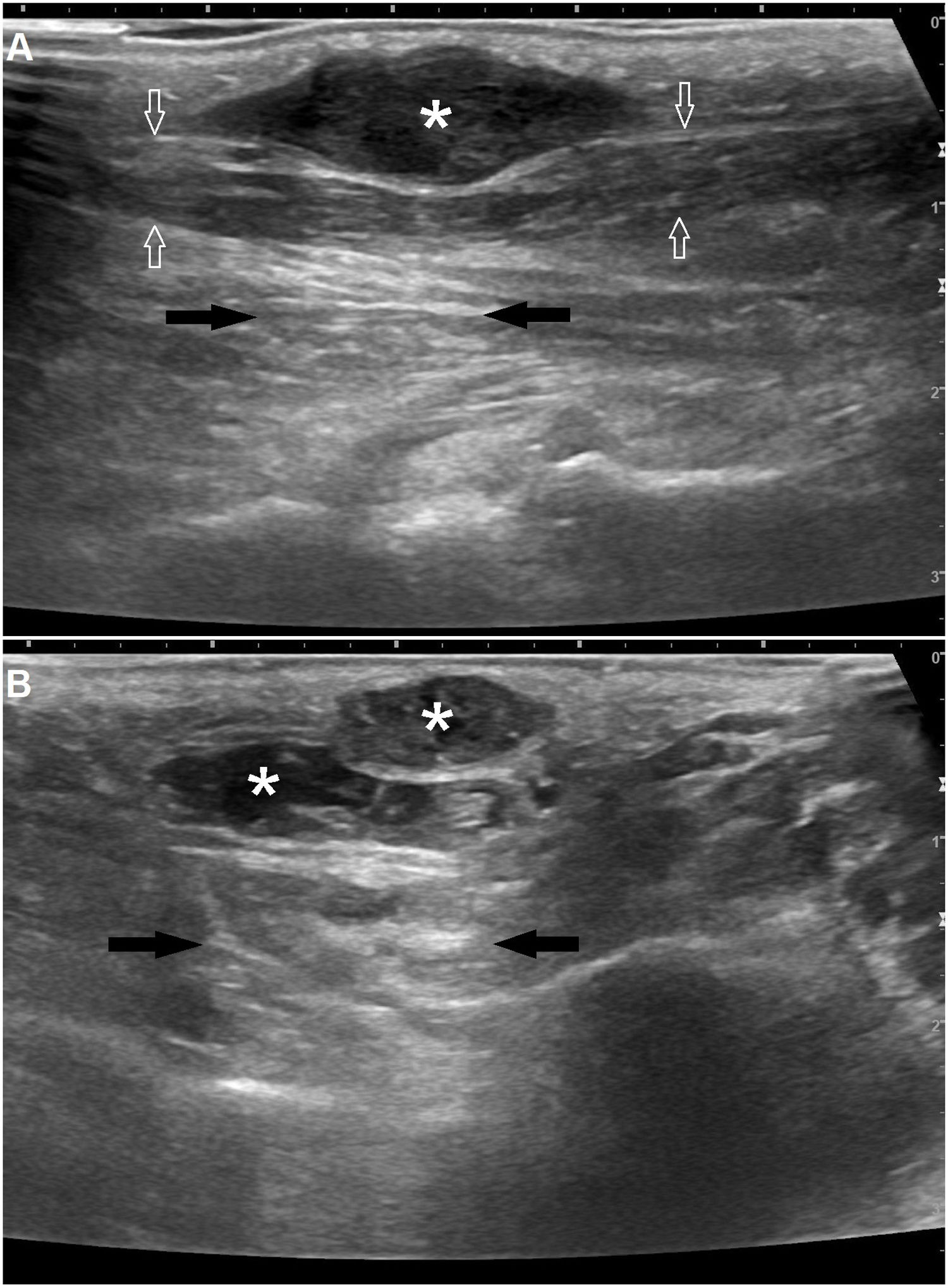
An ultrasound was performed on both feet with a high frequency linear transducer (7.5–13MHz). Hypoechoic and isoechoic lesions with a fusiform morphology, nodular profiles and irregular borders, with posterior acoustic enhancement and no colour Doppler recording, were identified on the long axis. All the lesions found had a similar echostructure and were located in the medial segment of the plantar fascia on the superficial and medial planes. The lesions depended on the plantar fascia, varied in size and measured up to 25mm, and were found to be in contact with the subcutaneous cellular tissue (Fig. 2A). On the short axis, the lesions could be seen to be in contact with each other (Fig. 2B).
 A well-defined hypoechoic nodule with a fusiform morphology (asterisk) can be seen in the middle third of the medial band of the plantar fascia (white arrows). This lesion presses against the underlying muscle and presents posterior acoustic enhancement (black arrows). (B) Pseudonodular lesions in contact with each other with a mixed internal structure (asterisk), arising from the medial band of the plantar aponeurosis, located in the medial to distal third thereof. The lesions also show posterior acoustic enhancement (black arrows).")
A) A well-defined hypoechoic nodule with a fusiform morphology (asterisk) can be seen in the middle third of the medial band of the plantar fascia (white arrows). This lesion presses against the underlying muscle and presents posterior acoustic enhancement (black arrows). (B) Pseudonodular lesions in contact with each other with a mixed internal structure (asterisk), arising from the medial band of the plantar aponeurosis, located in the medial to distal third thereof. The lesions also show posterior acoustic enhancement (black arrows).
With these findings, a diagnosis was made of plantar fibromatosis or Ledderhose disease. Nodules with similar characteristics, but smaller in size, were found on the flexor apparatus of the palms of both of the patient's hands. Hence, he was incidentally diagnosed with concomitant subclinical palmar fibromatosis.
Ledderhose disease is a form of superficial fibromatosis caused by benign proliferation of fibroblasts of the plantar aponeurosis. Even today, the aetiopathogenesis of this disease is unknown. It is a rare disease with a higher prevalence in males, and although it may appear at any age, it is more common in middle age.1 Various predisposing factors have been reported, such as alcohol use, diabetes and epilepsy.
The plantar fascia or plantar aponeurosis is a fibrous band of connective tissue that lends support and structure to the longitudinal arch or plantar vault. This fascia, which is normally 1–2mm thick, consists of three compartments or bands (central, lateral and medial). The central compartment extends from the medial tubercle of the calcaneus to its insertion in the metatarsophalangeal joints. The lateral compartment originates in the lateral margin of the medial tuberosity of the calcaneus and inserts into the joint capsule of the fifth metatarsal joint. Finally, the medial compartment spans from its origin in the medial portion of the central band to its insertion in the first metatarsal joint.2
Lesions are usually asymptomatic, but may become painful or even debilitating. Bilateral involvement is seen in just 25% of cases.1 This fibromatosis usually does not involve retraction of anatomical structures, unlike palmar fibromatosis or Dupuytren's disease. Often, patients with plantar fibromatosis also have other fibromatous diseases such as induratio penis plastica (Peyronie's disease) or palmar fibromatosis.
Diagnosis is based on physical examination and complementary imaging tests consistent with the nature of this disease. In rare cases, histological confirmation is required. Magnetic resonance imaging and ultrasound are the tests of choice, though ultrasound is the most accessible and least costly imaging test for diagnostic confirmation.
On ultrasound, lesions present as hypoechoic nodules (76% of cases) or isoechoic nodules (24% of cases) that are well defined with a uniform internal structure featuring sparse, thin hyperechoic septa. The most common site of lesions is the medial compartment or band (60%); the second most common is the central compartment or band (40%). Colour Doppler is usually negative, shows no flow and reveals intrinsic vascularisation in just 8% of cases.3,4 Lesions often show posterior acoustic enhancement (in 20%-65% of cases, depending on the case series); posterior acoustic shadowing is more uncommon.3,5
The differential diagnosis of plantar fibromatosis should include consideration of the following diseases of the plantar fascia: diabetic fascial disease, plantar fascia rupture, xanthomas, reactions to foreign bodies, plantar infections and aggressive plantar fibromatosis presenting in the form of nodules with poorly defined margins that exhibit superficial or deep infiltration of the plantar fascia.2
Magnetic resonance imaging is most useful in evaluating disease severity and in assessing the depth or extent of aggressive or wide-spreading forms of the disease.4
Please cite this article as: García-Gil MF, Lezcano Biosca V. Fibromatosis plantar o enfermedad de Ledderhose: diagnóstico ecográfico. Radiología. 2020;62:415–416.

