


The incidence of paravalvular aortic regurgitation (PAR) seems higher among patients submitted to transcatheter aortic valve implantation and its potential association with an increased late mortality has raised concerns in the scientific community. Our objective was to evaluate the incidence and clinical impact of PAR and establish PAR predictors in our patient population.
MethodsBetween July/2009 and February/ 2013, 112 patients were submitted to transcatheter aortic valve implantation. The degree of PAR after the procedure was assessed according to the VARC 2 criteria. The population was divided into no/mild PAR group and moderate/severe PAR group.
ResultsMean age was 82.5+3.9 years, 58.9% were female and the logistic EuroSCORE was 23.6±13.4. There was a decrease in the mean systolic gradient (54.7 ± 15.3mmHg vs 11.7 ± 4 mmHg; P < 0.01) and a gain in the aortic valve area (0.66±0.15cm2 vs 1.8 ± 0.3cm2; P < 0.01). At the end of the procedure 46.4% did not have PAR, and mild or moderate PAR was observed in 42% and 11.6% of the patients. No patient presented severe PAR. Multivariate analysis identified male gender [odds ratio (OR) 5.85, confidence interval (CI] 1.29-26.7; P = 0.022), previous percutaneous aortic valvuloplasty (OR 18.44, CI 2.30-147.85; P = 0.006), ejection fraction < 35% (OR 4.160, CI 1.014-17.064; P = 0.048) and the presence of severe pulmonary hypertension (OR 7.649, CI 1.86-31.51; P = 0.005) as independent predictors of moderate/ severe PAR.
ConclusionsThe incidence of moderate/severe PAR was low and comparable to other studies. Male gender, history of prior percutaneous aortic valvuloplasty, presence of severe pulmonary hypertension and severe left ventricular dysfunction were independent predictors of this complication.
Análise da Incidência e Preditores Clínicos e Ecocardiográficosdo Refluxo Paraprotético Aórtico após o Implante de Prótese Aórtica Transcateter
IntroduçãoA incidência de refluxo paraprotético (RPP) parece maior entre os pacientes submetidos a implante de prótese aórtica transcateter e sua potencial associação com aumento da mortalidade tardia tem suscitado preocupação na comunidade científica. Nosso objetivo foi avaliar a incidência e o impacto clínico e estabelecer preditores do RPP em nossa casuística.
MétodosEntre julho de 2009 e fevereiro de 2013, 112 pacientes foram submetidos a implante de prótese aórtica transcateter. O grau do RPP pós-procedimento foi avaliado segundo os critérios do VARC 2. Dividiu-se a população em grupo RPP ausente/RPP discreto e grupo RPP moderado/RPP grave.
ResultadosA média da idade foi de 82,5 ± 3,9 anos, 58,9% eram do sexo feminino e o EuroSCORE logístico foi de 23,6 ± 13,4. Houve queda do gradiente sistólico médio (54,7 ± 15,3mmHgvs. 11,7 ± 4mmHg; P < 0,01) e ganho da área valvar aórtica (0,66 ± 0,15cm2 vs. 1,8 ± 0,3cm2; P < 0,01). Ao final do procedimento, 46,4% não apresentaram RPP, e RRP discreto ou moderado foi observado em 42% e 11,6% dos pacientes. Nenhum paciente apresentou RPP grave. A análise multivariada identificou sexo masculino [odds ratio (OR) 5,85, intervalo de confiança (IC] 1,29-26,7; P = 0,022), valvoplastia aórtica percutânea prévia (OR 18,44, IC 2,30-147,85; P = 0,006), fração de ejeção < 35% (OR 4,160, IC 1,014-17,064; P = 0,048) e presença de hipertensão pulmonar grave (OR 7,649, IC 1,86-31,51; P = 0,005) como preditores independentes de RPP moderado/grave.
ConclusõesA incidência de RPP moderado/grave foi baixa e comparável à de outras casuísticas. Sexo masculino, antecedente de valvoplastia aórtica percutânea prévia, presença de hipertensão pulmonar grave e disfunção ventricular esquerda grave foram preditores independentes dessa complicação.
In recent years, the implantation of a transcatheter aortic valve prosthesis has become the treatment of choice for patients with severe symptomatic aortic stenosis considered inoperable,1 and an effective alter-native in patients at high surgical risk.2
However, the incidence of paravalvular aortic re-gurgitation (PAR) appears to be higher among patients submitted to transcatheter aortic valve implantation than after surgical aortic valve replacement,1,2 and its potential association with increased late mortality3 has raised concern in the international scientific community; PAR is considered the downfall of transcatheter aortic prosthesis implantation.4
The present study aimed to evaluate the incidence, severity, and clinical impact of PAR in patients under-going transcatheter aortic prosthesis implantation at two institutions in the State of São Paulo, Brazil, and to try to establish the clinical and echocardiographic predictors of this serious problem.
METHODSSubjects and procedureThis retrospective study included all symptomatic patients with severe aortic stenosis, considered to be at high surgical risk/inoperable, submitted to transcatheter aortic prosthesis implantation at Instituto de Cardiologia Dante Pazzanese and at Hospital do Coração da Associação do Sanatório Sírio between June 2009 and February 2013.
As part of the pre-intervention assessment, patients underwent computed tomography, angiography of the heart, aorta, and iliac arteries; coronary angiography; and transthoracic echocardiography. Based on the results of these tests, and after discussing with the lo-cal heart team, the access route was chosen, and the type and diameter of the prosthesis to be implanted was established. Three types of prosthesis were used:
CoreValve® (Medtronic – Minneapolis, USA) by trans-femoral, trans-subclavian, or transaortic approach; SAPIEN XT™ (Edwards Lifesciences – Irvine, California, United States), by transfemoral or transapical approach; and Acurate TF™ (Symetis Inc. – Geneva, Switzerland) by transfemoral approach.
All procedures were performed under general anes-thesia and guided by transesophageal echocardiography. After left ventricular catheterisation, aortic balloon val-vuloplasty was performed in cases in which the SAPIEN XT™ and Acurate TF™ prostheses were used or, when necessary, in cases in which the CoreValve® prosthesis was used. Subsequently, the prosthesis was implanted, and post-dilation was performed at the surgeon’s discretion.
DefinitionsThe pre-intervention clinical variables followed the definitions published by the Society of Thoracic Surgeons, 5 and surgical risk and possible post-intervention complications were determined in accordance with the logistic EuroSCORE.6
Transthoracic echocardiography was used to de-fine the left ventricular end-systolic and end-diastolic diameter, left ventricular ejection fraction, aortic annulus diameter, the diameter of the sinus of Valsalva, the ascending aorta diameter, the aortic valve area, the maximum and mean systolic gradients, the severity of aortic valve calcification, and the prosthetic valve area.
The degree of PAR after the procedure was evalu-ated by transthoracic echocardiography performed by one of three experienced echocardiographists designated as members of the heart team and according to the criteria proposed by the Valve Academic Research Consortium – 2 (VARC 2),7 classified as mild, moderate, or severe PAR using semi-quantitative and quantitative parameters.[4,7,8]
The study population was divided into two groups, according to the occurrence of post-procedure PAR: absent PAR/mild PAR and moderate PAR/severe PAR.Device success was considered when a single pros-thesis was implanted properly and final results showed absence of prosthesis-patient mismatch, mean aortic transvalvular gradient < 20 mmHg, peak velocity < 3 m/s, and mild aortic regurgitation at the maximum.7
Statistical AnalysisContinuous variables were shown as means and standard deviations, and categorical variables as fre-quencies and percentages, compared, respectively, by the chi-squared test and Student’s t-test.
A Cox logistic regression model was used to de-termine independent predictors of moderate/severe PAR after transcatheter aortic valve implantation, including variables with P-values ≤ 0.2 in the univariate model.
Data were analyzed using SPSS, version 20 (SPSS Inc. – Chicago, USA). P-values < 0.05 were considered statistically significant.
RESULTSCharacteristics of the population and the procedureBetween June 2009 and February 2013, a total of 182 patients with symptomatic severe aortic stenosis were evaluated for transcatheter aortic valve implantation. Of these, 112 patients (62%) underwent trans-catheter aortic valve implantation at Instituto Dante Pazzanese de Cardiologia (n = 96, 86%) and at the Hospital do Coração da Associação do Sanatório Sírio (n = 16, 14%).
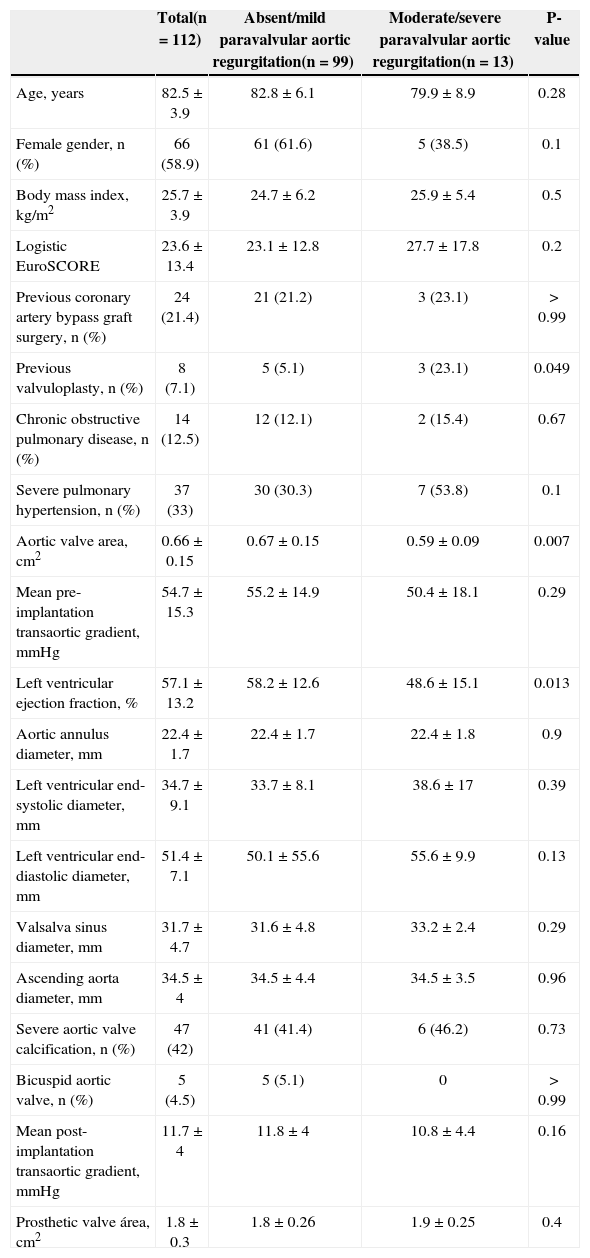
Basal clinical and echocardiographic characteristics of the 112 patients are shown in Table 1. The mean age of patients was 82.5 ± 3.9 years, and the majority (58.9%) were female. The mean logistic EuroSCORE was 23.6 ± 13.4 and 88 (79%) were in functional class III – IV of the New York Heart Association (NYHA) criteria before the intervention.
Basal clinical and echocardiographic characteristics
| Total(n = 112) | Absent/mild paravalvular aortic regurgitation(n = 99) | Moderate/severe paravalvular aortic regurgitation(n = 13) | P-value | |
|---|---|---|---|---|
| Age, years | 82.5 ± 3.9 | 82.8 ± 6.1 | 79.9 ± 8.9 | 0.28 |
| Female gender, n (%) | 66 (58.9) | 61 (61.6) | 5 (38.5) | 0.1 |
| Body mass index, kg/m2 | 25.7 ± 3.9 | 24.7 ± 6.2 | 25.9 ± 5.4 | 0.5 |
| Logistic EuroSCORE | 23.6 ± 13.4 | 23.1 ± 12.8 | 27.7 ± 17.8 | 0.2 |
| Previous coronary artery bypass graft surgery, n (%) | 24 (21.4) | 21 (21.2) | 3 (23.1) | > 0.99 |
| Previous valvuloplasty, n (%) | 8 (7.1) | 5 (5.1) | 3 (23.1) | 0.049 |
| Chronic obstructive pulmonary disease, n (%) | 14 (12.5) | 12 (12.1) | 2 (15.4) | 0.67 |
| Severe pulmonary hypertension, n (%) | 37 (33) | 30 (30.3) | 7 (53.8) | 0.1 |
| Aortic valve area, cm2 | 0.66 ± 0.15 | 0.67 ± 0.15 | 0.59 ± 0.09 | 0.007 |
| Mean pre-implantation transaortic gradient, mmHg | 54.7 ± 15.3 | 55.2 ± 14.9 | 50.4 ± 18.1 | 0.29 |
| Left ventricular ejection fraction, % | 57.1 ± 13.2 | 58.2 ± 12.6 | 48.6 ± 15.1 | 0.013 |
| Aortic annulus diameter, mm | 22.4 ± 1.7 | 22.4 ± 1.7 | 22.4 ± 1.8 | 0.9 |
| Left ventricular end-systolic diameter, mm | 34.7 ± 9.1 | 33.7 ± 8.1 | 38.6 ± 17 | 0.39 |
| Left ventricular end-diastolic diameter, mm | 51.4 ± 7.1 | 50.1 ± 55.6 | 55.6 ± 9.9 | 0.13 |
| Valsalva sinus diameter, mm | 31.7 ± 4.7 | 31.6 ± 4.8 | 33.2 ± 2.4 | 0.29 |
| Ascending aorta diameter, mm | 34.5 ± 4 | 34.5 ± 4.4 | 34.5 ± 3.5 | 0.96 |
| Severe aortic valve calcification, n (%) | 47 (42) | 41 (41.4) | 6 (46.2) | 0.73 |
| Bicuspid aortic valve, n (%) | 5 (4.5) | 5 (5.1) | 0 | > 0.99 |
| Mean post-implantation transaortic gradient, mmHg | 11.7 ± 4 | 11.8 ± 4 | 10.8 ± 4.4 | 0.16 |
| Prosthetic valve área, cm2 | 1.8 ± 0.3 | 1.8 ± 0.26 | 1.9 ± 0.25 | 0.4 |
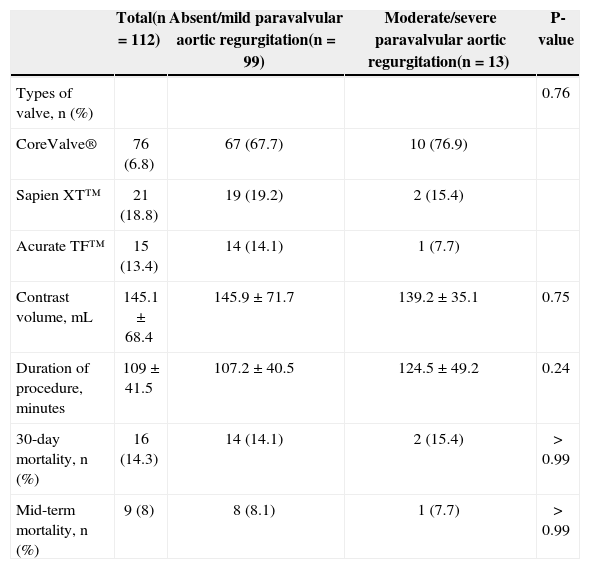
The femoral vein was used in 91% of the patients, followed by transapical (6%), transaortic (2%), and subclavian (1%) routes. The CoreValve® prosthesis was used in 76 patients (68.8%), whereas the Sapien XT™ was used in 21 (18.8%), and the Acurate TF™, in 15 (13.4%).
The maximum transaortic gradient before the procedure was 88 ± 24.3mmHg and the mean was 54.7 ± 15.3 mmHg, whereas the mean aortic valve area was 0.66 ± 0.15cm2. There was a decrease in the mean systolic gradient (pre = 54.7 ± 15.3mmHg vs. post = 11.7 ± 4mmHg; P < 0.01) and a gain in aortic valve area (pre = 0.66 ± 0.15cm2 vs. post = 1.8 ± 0.3cm2; P < 0.01) immediately after device implantation.
Device success was achieved in 94 patients (83.9%). There were two deaths during the procedure (1.8%), and five cases (4.5%) needed a second prosthesis due to inappropriate positioning of the first.
Immediately after prosthesis implantation, 38 patients (33.9%) required post-dilation to reduce PAR, which occurred in two-thirds of the patients. At the end of the procedure, 52 patients (46.4%) had no PAR and 47 (42%) had mild PAR, while moderate PAR was observed in 13 patients (11.6%). No patients had severe PAR.
Among the patients who developed moderate/severe PAR, the incidence of previous aortic valvuloplasty was higher (23.1% vs. 5.1%; P = 0.049). Additionally, patients in this group had smaller aortic valve area (0.67 ± 0.15cm2 vs. 0.59 ± 0.09cm2; P = 0.007), and left ventricular ejection fraction was also lower (58.2 ± 12.6% vs. 48.6 ± 15.1%; P = 0.013) at the pre-intervention echocardiography. There was no difference between the groups regarding mean transaortic gradient, aortic annulus diameter, severity of aortic valve calcification, and incidence of bicuspid aortic valve.
Patients in both groups did not differ regarding the type of prosthesis used and the amount of contrast or procedure duration. Overall 30-day mortality of patients included in this study was 14.3%, with no statistical dif-ference between groups. After the first 30 days, mortality from all causes, considering only patients who were discharged from the hospital, was 9.4%. The mid-term follow-up (16 ± 11 months) showed no difference in mortality between the groups (Table 2).
Types of valve used and main characteristics of the procedure
| Total(n = 112) | Absent/mild paravalvular aortic regurgitation(n = 99) | Moderate/severe paravalvular aortic regurgitation(n = 13) | P-value | |
|---|---|---|---|---|
| Types of valve, n (%) | 0.76 | |||
| CoreValve® | 76 (6.8) | 67 (67.7) | 10 (76.9) | |
| Sapien XT™ | 21 (18.8) | 19 (19.2) | 2 (15.4) | |
| Acurate TF™ | 15 (13.4) | 14 (14.1) | 1 (7.7) | |
| Contrast volume, mL | 145.1 ± 68.4 | 145.9 ± 71.7 | 139.2 ± 35.1 | 0.75 |
| Duration of procedure, minutes | 109 ± 41.5 | 107.2 ± 40.5 | 124.5 ± 49.2 | 0.24 |
| 30-day mortality, n (%) | 16 (14.3) | 14 (14.1) | 2 (15.4) | > 0.99 |
| Mid-term mortality, n (%) | 9 (8) | 8 (8.1) | 1 (7.7) | > 0.99 |
Multivariate analysis identified the following in-dependent predictors of moderate/severe PAR: male gender (odds ratio [OR] 5.85; confidence interval [CI]: 1.29 to 26.7; P = 0.022], aortic valvuloplasty prior to the percutaneous procedure (OR: 18.44; CI: 2.30 to 147.85; P = 0.006), ejection fraction < 35% (OR: 4.160; CI: 1.014 to 17.064; P = 0.048), and presence of severe pulmonary hypertension (OR: 7.649; CI: 1.86 to 31.51; P = 0.005). No variables of the procedure were associated with the occurrence of this complication.
DISCUSSIONThe most important finding of the present study was that, although the occurrence of transcatheter aortic valve post-implantation PAR is common (53.6%), most cases are mild. In this study, there were no cases of severe PAR, and moderate PAR did not result in poor clinical outcome in the mid-term follow-up.
The incidence of moderate/severe PAR in the pres-ent patients (11.6%) was similar to that observed in the Placement of Aortic Transcatheter Valve Trial (PARTNER),[1,2] a randomized study in which the incidence in the A and B cohorts was 12.2% and 11.8%, respectively. Regarding the high incidence of mild PAR (42%), se-veral international registries have shown similar rates.[9–11]
It has been speculated that the high incidence of PAR described after transcatheter aortic valve implantation, a result of the incomplete apposition of the prosthesis in the aortic annulus, may be caused by the heterogeneity of calcium distribution in the leaflets and annulus, or by the incorrect selection of the prosthesis diameter due to inadequate annulus measurement or the presence of extremely oval-shaped aortic annuli.4,12
One of the main predictors of PAR described in the literature is the low ratio between prosthesis diameter and annulus diameter assessed by echocardiography (or cover index).13 In a study published in 2009, Detaint et al.13 reported the absence of PAR moderate/severe in patients with cover index > 8%. Therefore, it is believed that the oversizing of the annulus diameter when choosing the prosthesis could be a good measure to prevent significant PAR after implantation. Another way to minimize the occurrence of this complication would be to choose the prosthesis diameter based on the tomography, not on the transthoracic echocardiography, as some recent studies have shown this method to be more accurate in predicting the size of the annulus and the valve area.[14–16] Currently, it is recommended to choose a prosthesis with a diameter at least 1mm larger than the mean annulus diameter, or area 10% larger than the annulus area measured by multiple-slice computed tomography.15 However, it is worth mention-ing that oversizing the prosthesis is not devoid of risk, as it can lead to annulus rupture.17
In the present series, the only echocardiographic predictor of PAR identified was the presence of severe left ventricular dysfunction (LV ejection fraction < 35%). Although the degree of calcification of leaflets and annulus was not a predictor of this event, it is worth noting that calcium assessment was performed qualitatively, based on transthoracic echocardiography evaluation. Several recent studies have used the Agatston score, defined by computed tomography, to quantitatively evaluate the valve apparatus degree of calcification. In this series, the degree of moderate/high calcification, which was more objectively assessed, emerged as an independent predictor of significant PAR.[18,19]
It is currently believed that the presence of PAR may have a negative impact on patient evolution.[3,4,9,10,20,21] In the recently published two-year evolution of the PARTNER study cohort A,3 the effect of PAR on mortality was proportional to PAR severity, and even the pres-ence of mild PAR was associated with increased late mortality. Recent meta-analysis conducted by Athappan et al.21 demonstrated that moderate or severe PAR after transcatheter aortic prosthesis implantation is frequent (11.7%), and is considered an independent predictor of immediate (OR 2.95; CI: 1.73 to 5.02) as well as long-term mortality (hazard ratio [HR] 2.27; 95% CI: 1.84 to 2.81). These results suggest that measures to improve PAR may lead to improved survival in patients submitted to transcatheter aortic valve implantation. It is noteworthy that the present series had no cases of severe PAR, and that moderate PAR was not associated with worse evolution in the mid-term.
CONCLUSIONSIn this initial experience of two national centers, the incidence of moderate/severe PAR was relatively low and comparable to other international samples. Male gender, history of previous percutaneous aortic valvuloplasty, and presence of severe pulmonary hypertension and severe left ventricular dysfunction were identified as independent predictors of the occurrence of this complication.
CONFLICTS OF INTERESTMagaly Arrais is a proctor at Medtronic (Minneapolis, USA) and Edwards Lifesciences (Irvine, USA). The other authors declare to have no conflicts of interest.