


The minimal luminal area (MLA) measured by intravascular ultrasound (IVUS) is a predictor of cardiovascular events in patients with angiographically moderate lesions. On the other hand, the presence of calcium is a predictor of lesion stability. The objective of this study is to evaluate the influence of the total amount of coronary calcium, obtained by multislice CT scanner (MDCT), on the severity of moderate lesions as assessed by IVUS.
MethodsIVUS was performed in 27 moderate lesions in a consecutive series of 22 patients with indication for the procedure who had a previous MDCT. Measurements of the minimal luminal area (MLA), plaque burden and percentage area stenosis were obtained.
ResultsMost patients were male (85%), with mean age of 60±9 years and 41% were diabetic. A significant correlation was observed between the MLA and total calcium score (r=0.67; P=0.002), but there was no correlation between the total calcium score and plaque burden (r=0.02; P=0.93) or percentage area stenosis (r=0.3; P=0.32). Independent predictors of MLA in the multivariate analysis were age (P=0.02), body mass index (P=0.01), diabetes (P=0.02), dyslipidemia (P=0.02), high-sensitive C-reactive protein (P=0.02), glucose (P=0.02), HDL-cholesterol (P=0.02), triglycerides (P=0.02), left ventricular ejection fraction < 50% (P=0.02) and total calcium score (P=0.03).
ConclusionsThe total calcium score correlates positively with MLA in coronary arteries, suggesting that a large calcium burden in the coronary tree is related to angiographically moderate lesions with larger luminal areas at IVUS.
Influência do Escore de Cálcio na Gravidadede Lesões Coronárias Moderadas Avaliadas pelo Ultrassom Intracoronário
IntroduçãoA área luminal mínima (ALM), obtida pelo ultrassom intracoronário (USIC), é preditora de eventos em pacientes com lesões de moderada gravidade, identificadas à angiografia coronária. Por outro lado, a presença de cálcio é preditora de estabilidade das lesões. O objetivo deste estudo é avaliar qual a influência da quantidade total de cálcio coronário, obtido pela tomografia computadorizada cardíaca (TCC), na gravidade de lesões moderadas, avaliadas por meio de USIC.
MétodosRealizamos USIC de 27 lesões moderadas, em uma série consecutiva de 22 pacientes com indicação para o procedimento, e que tinham TCC prévia. Foram obtidas medidas da ALM, carga de placa e porcentual de área de estenose.
ResultadosOs pacientes eram, em sua maioria, do sexo masculino (85%), com idade de 60±9 anos e 41% eram diabéticos. Observamos correlação significativa entre ALM e escore de cálcio total (r=0,67; P=0,002), mas não houve correlação entre escore de cálcio total e carga de placa (r=0,02; P=0,93) ou porcentual de área de estenose (r=0,3; P=0,32). Os preditores independentes da ALM na análise multivariada foram idade (P=0,02), índice de massa corporal (P=0,01), diabetes (P=0,02), dislipidemia (P=0,02), proteína C-reativa ultrassensível (P=0,02), glicemia (P=0,02), HDL-colesterol (P=0,02), triglicerídeos (P=0,02), fração de ejeção do ventrículo esquerdo < 50% (P=0,02) e escore de cálcio total (P=0,03).
ConclusõesO escore de cálcio total apresenta correlação positiva com a ALM em artérias coronárias, sugerindo que maior quantidade de cálcio na árvore coronária implica lesões ateroscleróticas moderadas com maiores áreas luminais ao USIC.
Coronary artery disease (CAD) is of utmost relevance in contemporary society due to its epidemic occurrence in developed and developing countries. CAD evaluation using complementary methods is fundamental in order to stratify patients in primary and secondary prevention.
Several advances in recent years have intensified the accuracy of these methods in CAD assessment. Cardiac computed tomography (CT) has been used as a non-invasive technique for CAD screening and detection of coronary calcifications. The calcium score is a quantitative index of total coronary artery calcium detected by CT.1 Among the invasive modalities, intravascular ultrasound (IVUS) is the method of choice, presenting good accuracy to assess coronary stenosis severity and the minimal lumen area and demonstrated prognostic value.2
This study aimed to evaluate the influence of the total amount of calcium in coronary arteries, detected by CT, on the severity of moderate lesions assessed by IVUS.
METHODSStudy protocol and definitionsBetween August 2007 and April 2011, 22 patients with IVUS indication to assess moderate lesions detected by angiography were included in this prospective registry. A total of 27 de novo coronary lesions were evaluated, in native vessels with a stenosis diameter between 40% and 69%, by visual estimation, in one or more vessels, which could be crossed by an IVUS catheter at the time of the diagnostic examination or immediately before the percutaneous coronary intervention, and minimal luminal area (MLA) was measured. All patients had undergone pre-procedure cardiac CT that identified the lesions, their severity, and calcium score, measured in accordance with the Agatston scale. The ethics committees of the participating institutions approved the protocol, and an informed consent was obtained from all participants.
Image acquisition protocol and data analysisThe coronary angiograms were performed according to well-established techniques3 and standardized at the Hemodynamics Service of Instituto de Cardiologia Ecoville/Instituto de Neurologia de Curitiba (INC), Curitiba, PR, Brazil. An Atlantis IVUS catheter (Clearview – Boston Scientific, Boston, USA) of 40MHz was positioned distal to the lesion and recoiled at 0.5mm/second until the proximal reference was reached. The contours of the outer elastic membrane, plaque+media, and lumen were generated by the online analysis of the CT section related to the MLA, and the plaque+media area (area of the outer elastic membrane – MLA) and plaque burden (plaque+media area / MLA) were calculated.
CT scans were performed using a LightSpeed VCT XT device with 64 slice multidetector (GE Healthcare – Milwaukee, USA) at the INC/CETAC (Diagnostic Imaging Center). The acquisition of calcium score required a mean inspiratory pause of approximately 15 seconds, following the protocol of Agatston et al.4 The parameters for the acquisition of calcium score were: tube rotation velocity of 0.75seconds, detector collimation of 4 by 3mm, tube voltage of 120kV, and tube current of 300mA. Total calcium scores were obtained for each patient. The Agatston score was used in the analysis of calcium score images. Target vessel calcium score, defined as the calcium score of the assessed artery, was also analyzed.
Statistical AnalysisThe statistical analysis was performed using the software StatView, version 5.0.1 (SAS Institute – Cary, United States). Categorical variables were expressed as numbers and percentages and compared using the chi-squared test. Continuous variables were expressed as mean and standard deviation and compared with the unpaired Student’s t-test. Linear regression was used to determine the association between continuous variables. Multivariate regression performed in steps was used to identify predictors of MLA, and standardized coefficients (b) were calculated to quantify the importance of each independent variable in the final model. P-values < 0.05 were considered statistically significant.
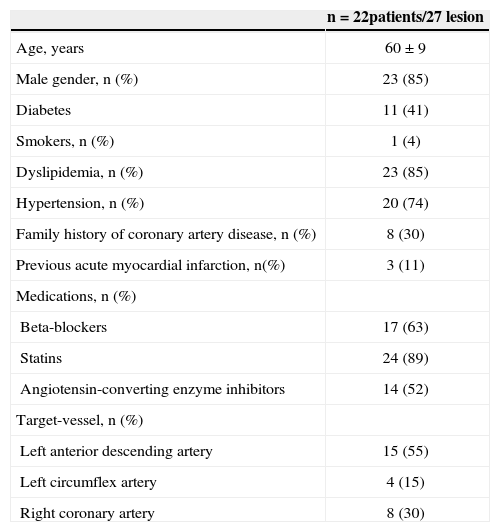
RESULTSDemographic and lesion characteristics are shown in Table 1. The patients were aged 60±9 years, 85% were males, and 41% were diabetics. The most frequently assessed vessel was the left anterior descending artery (55%) and the stenosis diameter of the lesions was 60±6% at the angiography (visual estimation).
Demographic and lesion characteristics
| n=22patients/27 lesion | |
|---|---|
| Age, years | 60±9 |
| Male gender, n (%) | 23 (85) |
| Diabetes | 11 (41) |
| Smokers, n (%) | 1 (4) |
| Dyslipidemia, n (%) | 23 (85) |
| Hypertension, n (%) | 20 (74) |
| Family history of coronary artery disease, n (%) | 8 (30) |
| Previous acute myocardial infarction, n(%) | 3 (11) |
| Medications, n (%) | |
| Beta-blockers | 17 (63) |
| Statins | 24 (89) |
| Angiotensin-converting enzyme inhibitors | 14 (52) |
| Target-vessel, n (%) | |
| Left anterior descending artery | 15 (55) |
| Left circumflex artery | 4 (15) |
| Right coronary artery | 8 (30) |
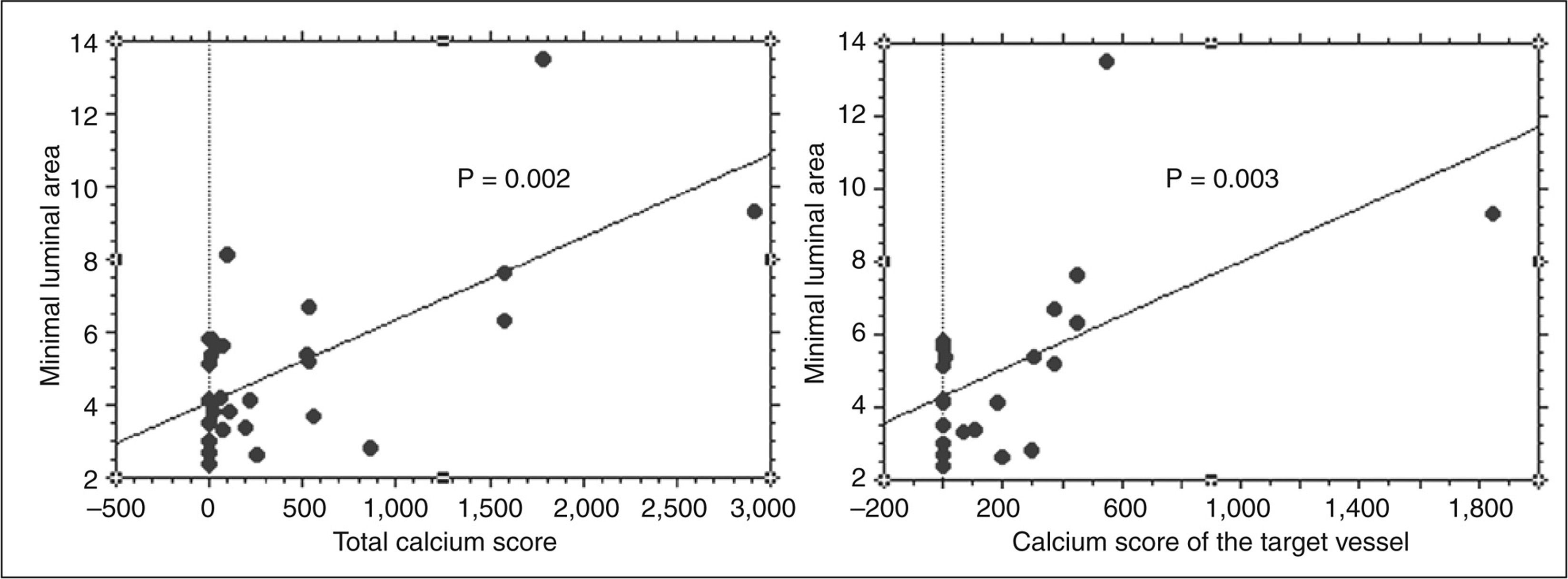
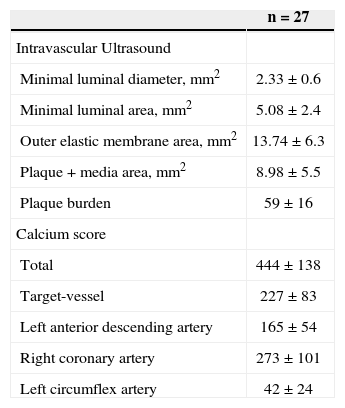
IVUS parameters and calcium scores are shown in Table 2. The MLA of the analyzed lesions was 5.08±2.4mm2. The mean total calcium score was 444±138. A simple univariate regression showed an association between the MLA and the total calcium score (r=0.67; P=0.002) and calcium score of the target vessel (r=0.59; P=0.003) (Figure 1). The plaque burden and the percentage of stenosis area were not significantly associated with the total calcium score. When the groups were separated according to the MLA values, patients with MLA > 4mm2 were compared with patients with MLA≤4mm2, there was no significant difference in the total calcium score (619±872 vs. 189±280; P=0.12) and calcium score of the target vessel (302±475 vs. 83±111; P=0.21).
Intravascular ultrasound parameters and calcium score
| n=27 | |
|---|---|
| Intravascular Ultrasound | |
| Minimal luminal diameter, mm2 | 2.33±0.6 |
| Minimal luminal area, mm2 | 5.08±2.4 |
| Outer elastic membrane area, mm2 | 13.74±6.3 |
| Plaque+media area, mm2 | 8.98±5.5 |
| Plaque burden | 59±16 |
| Calcium score | |
| Total | 444±138 |
| Target-vessel | 227±83 |
| Left anterior descending artery | 165±54 |
| Right coronary artery | 273±101 |
| Left circumflex artery | 42±24 |
 and calcium score of the target vessel (r=0.59; P=0.003).")
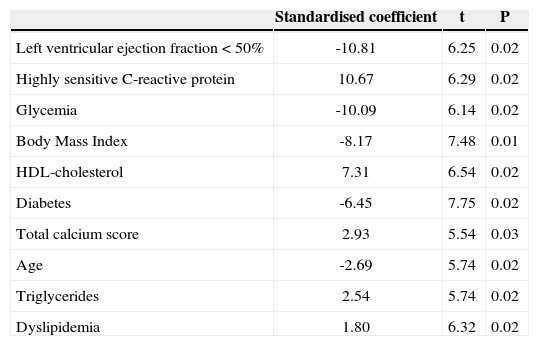
Multivariate regression was performed in steps to identify independent predictors of MLA, including risk factors for cardiovascular disease (age, diabetes, dyslipidemia, body mass index, highly-sensitive Creactive protein), lipid profile parameters (high-density lipoprotein [HDL]-cholesterol, triglycerides), glycemia, left ventricular ejection fraction, and total calcium score. Systemic arterial hypertension; smoking; family history; acute coronary syndrome; LDL-cholesterol; and use of statins, beta-blockers, and angiotensin-converting enzyme inhibitors did not reach significant correlation for entering the model. The final predictor model of the MLA comprised left ventricular ejection fraction < 50% (coefficient=−10.81; P=0.02), highly-sensitive C-reactive protein (coefficient=10.67; P=0.02), glycemia (coefficient=−10.09; P=0.02), body mass index (coefficient=−8.17; P=0.01), HDL-cholesterol (coefficient=7.31; P=0.02), diabetes (coefficient=−6.45; P=0.02), total calcium score (coefficient=2.93; P=0.03), age (coefficient=−2.69; P=0.02), triglycerides (coefficient=2.54; P=0.02), and dyslipidemia (coefficient=1.80; P=0.02) (Table 3).
Independent predictors of minimal luminal area in the multivariate analysis
| Standardised coefficient | t | P | |
|---|---|---|---|
| Left ventricular ejection fraction<50% | -10.81 | 6.25 | 0.02 |
| Highly sensitive C-reactive protein | 10.67 | 6.29 | 0.02 |
| Glycemia | -10.09 | 6.14 | 0.02 |
| Body Mass Index | -8.17 | 7.48 | 0.01 |
| HDL-cholesterol | 7.31 | 6.54 | 0.02 |
| Diabetes | -6.45 | 7.75 | 0.02 |
| Total calcium score | 2.93 | 5.54 | 0.03 |
| Age | -2.69 | 5.74 | 0.02 |
| Triglycerides | 2.54 | 5.74 | 0.02 |
| Dyslipidemia | 1.80 | 6.32 | 0.02 |
Multiple regression performed in stages. Systemic arterial hypertension, smoking, family history, acute coronary syndrome, LDL-cholesterol and use of statins, beta-blockers and angiotensin-converting enzyme inhibitors did not reach significant correlation for entering the model.
This study aimed to determine, in patients with moderate lesions at the angiography, whether the total calcium score could identify patients with smaller luminal areas. However, this correlation was shown to be positive: patients with higher amounts of calcium had larger MLA at the IVUS, raising the hypothesis that calcium is a possible stability factor in the context of secondary prevention.
Lesion calcium score and MLAThe presence of coronary calcium correlates with the presence and extent of coronary atherosclerosis.5 Thus, in the context of primary prevention, the absence of calcium in the coronary excludes the presence of significant luminal stenosis, with high predictive value. However, paradoxically, since large plaque burdens are not necessarily associated with hemodynamicallysignificant luminal narrowing, the detection of large amounts of calcium in the coronary does not necessarily imply the presence of significant stenosis.6,7 Therefore, the finding of marked coronary calcification by itself is not an indication for invasive coronary angiography.
In the context of secondary prevention, the role of calcium quantification in the coronary tree has not been well established. In agreement with the proposed concept that the degree of calcification of a coronary lesion is not necessarily a marker of severity degree, it was demonstrated in the classic study by Mintz et al.,6 correlating the extent of the lesion calcification (measured in arcs of calcium by IVUS) to other parameters detected by the method (such as plaque burden and MLA), that there was no significant correlation between the amount of calcium and the degree of luminal involvement.
However, recent studies have correlated the atherosclerotic plaque area detected by histopathology and the MLA measured by IVUS with calcium score of the lesion, with results discrepant from those of the present study.8−12 The authors determined that the lesion plaque area is positively correlated with calcium score of the lesion, while MLA by IVUS has an inverse correlation with calcium score of the lesion.13 It is noteworthy that the present study used different parameters from those used in previous studies: calcium score was measured in the entire target artery and coronary tree, which may explain the discrepancy in findings. Additionally, the calcium score of the lesion is still an experimental variable, without clinical validation and defined prognostic influence, different from the Agatston calcium score, which is undoubtedly a predictor of clinical events, as well as the MLA of the lesion. It was previously demonstrated that the MLA has prognostic influence – MLAs at IVUS≤4mm2 in angiographically moderate lesions (30% to 59% luminal stenosis) have greater chance of causing future cardiac events.14 Recently, Stone et al.15 demonstrated, in a prospective study including 679 patients undergoing intracoronary imaging of the three epicardial arteries, that the lesions associated with recurrent events in three years had significantly one or more of the following parameters compared to the lesions that did not cause events: plaque burden≥70% (hazard ratio [HR]=5.03; 95% confidence interval [95% CI]: 2.51 to 10.11; P < 0.001), MLA < 4mm2 (HR=3.21; 95% CI: 1.61 to 6.42; P=0.001), or being classified as thin-cap fibroatheroma at virtual histology (HR=3.35; 95% CI: 1.77 to 6.36; P < 0.001). These recent findings reinforce the importance of measuring the luminal area and studying the atherosclerotic plaque composition in an attempt to identify, as part of the investigation, lesions that have the potential to cause future cardiac events.
Thus, considering all concepts of coronary calcification and MLA, it can be stated that in primary prevention, a higher amount of total coronary calcium is associated with greater likelihood of significant lesion, and the absence of calcium has a high negative predictive value for future events. In the context of secondary prevention, the importance of calcium quantification is less clear. The presence of highly calcified lesions may be a predictor of stability, as demonstrated in previous histopathological16 and virtual histology studies; 17,18 the present finding that larger amounts of coronary calcium imply in moderate lesions with larger luminal areas is in agreement with these findings.
Study limitationsThe present study has limitations. The lack of serial evaluation with IVUS to analyze plaque regression/progression limits the present conclusions to an observational, non-longitudinal study, from which conclusions regarding plaque progression/regression and its association with calcium score should not be inferred. Additionally, since the study was performed in a small sample size, larger studies are needed to confirm these findings.
CONCLUSIONSIn a sample of patients with known CAD, the total calcium score showed a positive correlation with the lesion MLA. The present findings that a greater amount of calcium in the coronary tree implies lower severity of moderate lesions assessed by IVUS corroborates the concept that the calcification process in atherosclerotic disease, within the secondary prevention scenario, may be a stability factor.
CONFLICTS OF INTERESTThe authors declare no conflicts of interest.