



Grounded theory is a qualitative method that emphasises the induction or emergence of information from data, in order to establish a theory or model. From the classic description by Strauss and Glaser, different developments or schools are recognised, and some of the peculiarities and differences among them are discussed. Grounded theory is a versatile, organised and rigorous method, the application of which in health includes diverse fields such as public health, clinics and education.
La teoría fundamentada es un método cualitativo que enfatiza la inducción o emergencia de información de los datos para establecer una teoría o modelo. Desde la descripción clásica de Strauss y Glaser, se reconocen desarrollos o escuelas y se discuten algunas de las particularidades y diferencias entre ellos. La teoría fundamentada es un método versátil, organizado y riguroso, cuya aplicación en salud incluye campos diversos como la salud pública, la clínica y la educación.
Grounded theory (GT) is a qualitative research method that searches data for emerging conceptualisations in integrated and categorised patterns, analysing, through rigorous steps, in a process of constant comparison. This method is designed to generate concepts and theories which are grounded in data,1 hence its name. GT is both a method of studying processes and a method in process.2 The discovery of GT is the most cited qualitative research reference.3
According to Glaser, “GT is what it is, not what it should or could be”.4 It maintains an approach free of prejudices and preconceptions and produces the knowledge that lies in and emerges from the data. The investigator acts as a witness, regardless of their previous assumptions or expectations for the analysis; although one of the trends with a social constructionist vision of GT establishes that the role of the researcher is not limited to being a witness, since a particular understanding of the phenomenon under investigation is constructed, meaning that for this trend it is impossible to capture social “reality” as it is a social construction of reality in itself.2,5
In GT, data from any research method and source can be used, be it a clinical experiment, survey or content analysis, etc., without being linked to them; it transcends descriptive methods and their limitations, such as the search for accurate data, interpretation and how data are constructed.1
GT is a method of data gathering and analysis to develop middle-range theories. The method begins, but does not end, with inductive inquiry; it is a comparative, iterative and interactive method.2 GT is also considered a form of latent structure analysis which reveals fundamental patterns in an area.1
The most important property of the conceptualisation in GT is its abstraction of time, place and person, which it transcends; without this consideration, there can be no integrated theory based on conceptual and hypothetical relationships.1
As a theory, GT leads to a final product (explanation or theory) with an explanatory framework to understand the phenomenon studied, in an ordered and constant process of comparison, analysis and coding.5
A review of publications in the medical field using the PubMed search engine revealed that there is scant literature on the use of this method, despite the fact that it emerged from medical sociology, has been available for some time and that further developments have been made since its inception; for example, we found only nine articles on diabetes, five on depression, eight on schizophrenia, seven on dementia and none on euthanasia (PubMed).
Qualitative research in epidemiologyThe traditional model of evidence-based medicine (EBM) promotes the use of quantitative research and has emphasised that tests have a hierarchy in which qualitative or mixed methods research is not considered; among other characteristics, EBM places the emphasis on measurability, quantity and external validity. Qualitative research, including GT, has been devalued in the more conservative model of EBM.6 Nevertheless, qualitative research has gradually been gaining greater traction and influence in health research. However, its potential has not been sufficiently exploited to generate evidence, partly due to the greater difficulty in obtaining research funds7,8 and to the difficulty in understanding qualitative arguments and the greater ease of integrating numerical arguments.
Quantitative research is undeniably successful, offering certainty and reassurance in a world of uncertainty.9 Despite this, there are many barriers preventing the full use of the outcomes of such research, although these barriers are becoming increasingly more acknowledged; therefore, the use of qualitative research alone or in mixed methods for the generation, analysis and application of information does have a place in healthcare research.10
HistoryGT was developed by the sociologists Barney Glaser and Anselm Strauss who, having studied the dying in hospitals, published the book Awareness of Dying in 1965, in which they laid the foundations of GT and presented it as an alternative research approach. In view of its origins in medical sociology, GT places the emphasis on developing an understanding of behaviour through discovery and induction rather than the traditional process of deduction and hypothesis testing typical of medicine; hence, the theory is based on routine clinical practice.11,12
After Glaser and Strauss had developed their initial model of “classic grounded theory”, the rift between them spawned two distinct processes that yielded the two best-known GT schools, Glaserian and Straussian, along with other emerging schools:
- •
Emerging design, described by Glaser. In this approach, the theory is based on the data and the data are not categorised into preconceived categories, and analysis focuses less on characterisation based on such (deductive) categories. This design is used mainly in anthropology and sociology, it attempts to extract the greatest amount of information possible from the data and, as in anthropology methods, is free of preconceptions.13
- •
Constructivist design, developed by Charmaz. This design is based on constructivism and social constructionism. The researcher interprets the data as a construct, in other words, as valid and contextualised interpretations or visions of reality. The constructivist design initially focused on the study of chronic diseases. For example, the concept of HIV has changed over time, from a fatal to a chronic disease, but its meaning also varies from one individual to another, since while some regard it as a punishment, others see it as unavoidable, etc. These constructions determine how one copes (in different ways) or does not cope with a condition.2 Constructivism denies objectivity and a single reality, as there are as many constructions as there are individuals, although some constructions must be shared or common.12 From the standpoint of constructivism, it is people, including the researchers, who construct reality; in constructivist GT, the emphasis is placed on the construction of theories in the research process and the interaction between researcher and informant.14
- •
Systematic design, developed by Strauss and Corbin. This design is considered more open and more structured and is currently the most widely-used method due to its greater structure and a process that explicitly includes coding, categorisation and a more in-depth analysis.12
In addition to the above, some authors consider two further ones: postmodern situational analysis (Adele Clarke) and dimensional analysis.16
Although some have only referred to GT as initially described by Glaser and Strauss and that other developments should use a different name, one may say that there are different methods and developments that have expanded the possibilities and adaptations.15
Strauss and Corbin wrote Basics of Qualitative Research: Grounded Theory Procedures and Techniques, which presented a more descriptive view of GT; in response, Glaser4 wrote Emergence vs. Forcing: Basics of Grounded Theory Analysis, criticising the Strauss and Corbin view, asserting that it was a different method altogether. Another one of Strauss's criticisms of Glaser states that knowledge is linked to a specific time, person and place; GT forces us to ask, for example, “What power is there in situation and specific conditions? How is it manifested, by whom or what?” Failure to be receptive to this range of questions would ultimately prevent the discovery of important findings and preclude further conceptualisation.1
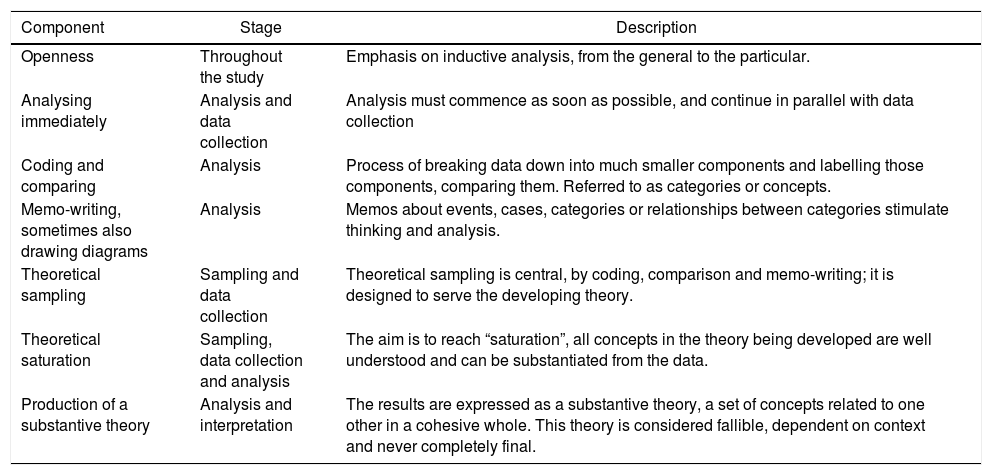
What the GT should contain remains a matter for debate, as shown in Table 1. Although these components may appear in other qualitative methods, the process is systematic in GT. Although there is no simple guide for developing it, researchers must be conversant with the method if they wish to adapt it for use.12,15
Fundamental components of a grounded theory study.
| Component | Stage | Description |
|---|---|---|
| Openness | Throughout the study | Emphasis on inductive analysis, from the general to the particular. |
| Analysing immediately | Analysis and data collection | Analysis must commence as soon as possible, and continue in parallel with data collection |
| Coding and comparing | Analysis | Process of breaking data down into much smaller components and labelling those components, comparing them. Referred to as categories or concepts. |
| Memo-writing, sometimes also drawing diagrams | Analysis | Memos about events, cases, categories or relationships between categories stimulate thinking and analysis. |
| Theoretical sampling | Sampling and data collection | Theoretical sampling is central, by coding, comparison and memo-writing; it is designed to serve the developing theory. |
| Theoretical saturation | Sampling, data collection and analysis | The aim is to reach “saturation”, all concepts in the theory being developed are well understood and can be substantiated from the data. |
| Production of a substantive theory | Analysis and interpretation | The results are expressed as a substantive theory, a set of concepts related to one other in a cohesive whole. This theory is considered fallible, dependent on context and never completely final. |
Adapted from Sbaraini et al.15
The basic principles of GT can be described as follows4:
- •
Constant comparative analysis: the emergence of subcategories is reviewed; for example, subcategories may emerge from the emotion category, such as joy, jealousy, anger, etc. In turn, differential subcategories may emerge from them, such as emotions that require an object (hatred and jealousy) and others that do not (joy and anxiety); this method recognises the complexity and diversity of the data.
- •
Negative case analysis: this ensures that the researcher develops the emerging theory in the light of the evidence, looking for negative cases.
- •
Theoretical sensitivity: the researcher is positioned analytically, asking questions, which means going back to the source to gather data.
- •
Theoretical sampling: data are collected in the light of categories that emerged in previous analysis stages.
- •
Theoretical saturation: ideally, the data collection process continues until categories cease to emerge.
- •
Memo-writing: a written record is kept of the development of the theory.
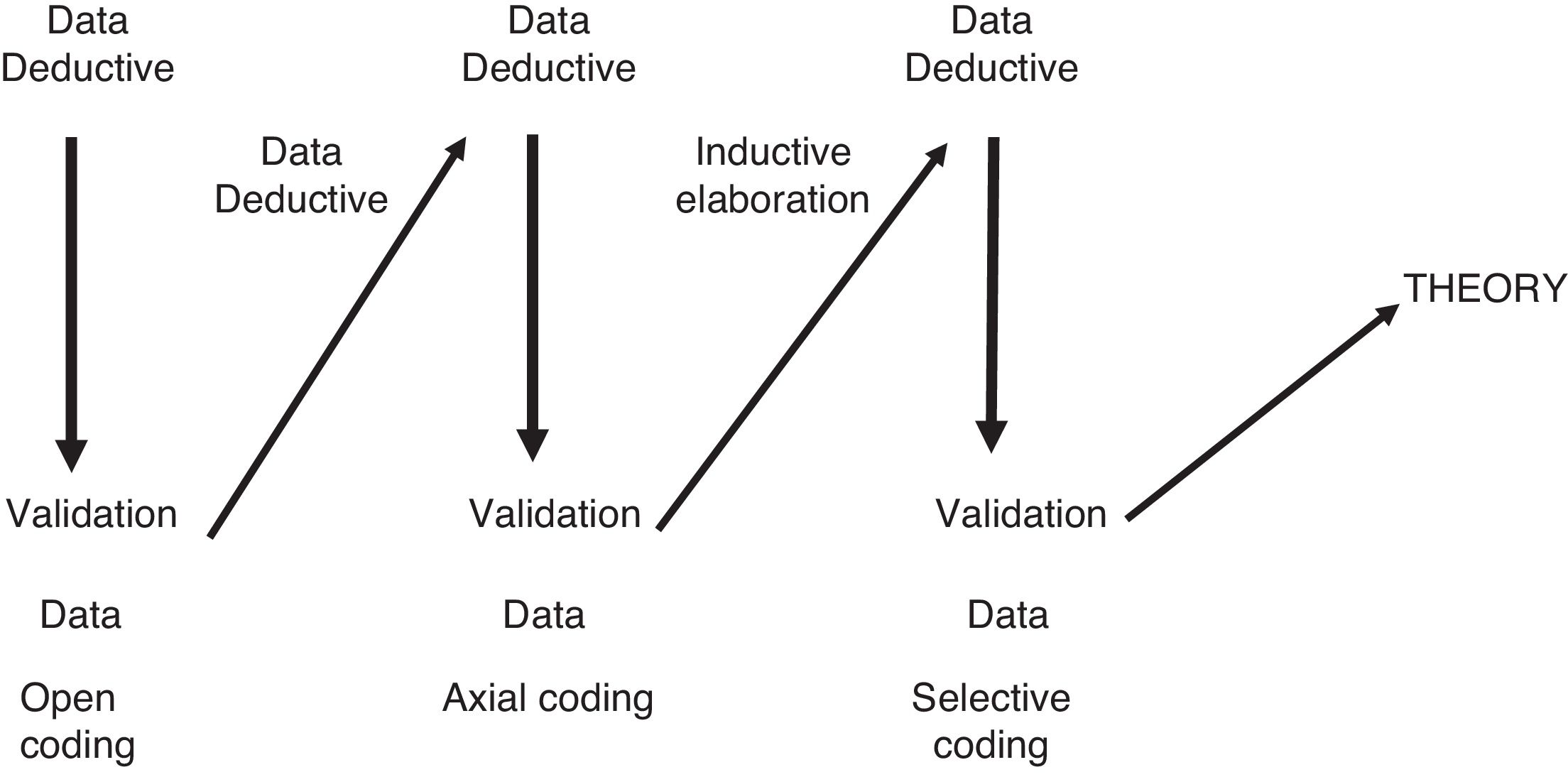
The GT process begins with data, which are transcribed. Memos are written and open encoding performed. Categories emerge from the codes, and from these, topics, ultimately yielding an explanatory theory or model.
The initial deductive categories (if there are any according to the model) generate inductive categories through the data review, and this process yields new deductive categories, the data are reviewed again and inductive categories are analysed until a theory can finally be established (Fig. 1).

Data collection and analysis in grounded theory.
The goal in GT is to reach at least the third level of conceptual analysis; the first level is data collection; the second, the generation of categories; the third level is to discover the core category that organises the other categories, from where a higher level, called formal theory, can be accessed.1
Coding is an essential part of the process and it involves an exhaustive reading and identification of topics, classes and categories to identify important subtopics. Consistency and depth must be guaranteed in the topics by means of a coding process. Coding can involve the following stages:
- •
Open: it seeks to find conceptual categories in the data.
- •
Axial: the aim is to relate categories.
- •
Selective: it accounts for relationships and finds core categories.
Glaser described certain requirements for being a good GT researcher that are typical of qualitative research, such as being able to tolerate confusion and regression, trusting emerging data without fear of having to justify oneself, having someone to talk to, being open to emerging evidence, being able to conceptualise to derive a theory from the data and being creative.2
Quality in grounded theoryQuality in qualitative methods can be addressed with the following criteria16:
- •
Credibility: the truth of the findings through the eyes of the research respondent or interviewee and in the context in which the research is carried out.
- •
Transferability: the extent to which findings can be transferred to other contexts.
- •
Dependability: the extent to which the research would yield similar and consistent findings if it were carried out as described.
- •
Confirmability: evidence that corroborates the findings, from the subjects and the research context.17
According to Glaser and Strauss (1967), quality in GT lies in adaptability (fit), work, relevance and modifiability, whereas for Strauss and Corbin (1990) there are two sets of criteria: the research process and the empirical grounding of the findings.11
Due to the continuous cycle of collection and rigorous data analysis inherent in GT, which includes the use of concurrent data collection, constant comparative analysis, theoretical sampling and memoing as an integral and non-optional part of its method, GT may be said to promote quality research.11
The following questions can be asked to evaluate a GT design18:
- •
Are the categories based on the data?
- •
Have sufficient data been gathered for dimensions to emerge and for saturation to occur?
- •
Does the theory emerge from the data?
- •
Does the theory provide an explanation of the process?
- •
Can the theory be modified by changes in conditions?
- •
Has the theory been validated?
Due to its origin in medical sociology, GT occupies an important field in healthcare research, as it allows problems to be analysed from a social and cultural perspective, with the emphasis on the forms of communication and language and the development of theoretical proposals.19 However, its applications have transcended the field of health to politics, the economy, companies, etc.2
There are multiple applications of GT in the field of health and in medicine in particular.20 For example, to study how general practitioners make sense of symptoms with no medical explanation, a study was conducted on approach and treatment in which clinicians avoided labelling patients with diagnoses such as “borderline personality disorder”, were afraid of overlooking serious complaints, focused on physical findings and referred the patient to other specialist areas in search of coordinated care. This demonstrates the ethical importance of psychiatric diagnoses and physicians’ attempts to protect patients from stigma and the careful collection of patient narratives about their condition in the case of symptoms with no clinical explanation.21
As for the applicability of GT to medical research, although its origin was the study of social processes and medical sociology, it can be used in different areas. In psychiatry, one criticism that could be levelled at the method is that it can be reduced to a technique for systematic categorisation which, while it may help to understand the structure of the participants’ experience, does not constitute a theory and is more descriptive than explanatory.4
ExamplesNursing is one of the health disciplines in which GT-based research has been developed most. The following question was asked in a research setting: “What is the role of gifts in the patient-nurse relationship?”, as it had transpired that patients often give presents to nurses for the care provided to them. In the course of the research it became clear that the fundamental question was the specific relationship, which led the question to be phrased differently: “How does the patient-nurse/nurse-patient relationship unfold?” In the transcription and coding, the terms of process and change and the negotiation of the relationship emerged as the core category and the types of relationship, which were divided into mutual and unilateral with subcategories.22
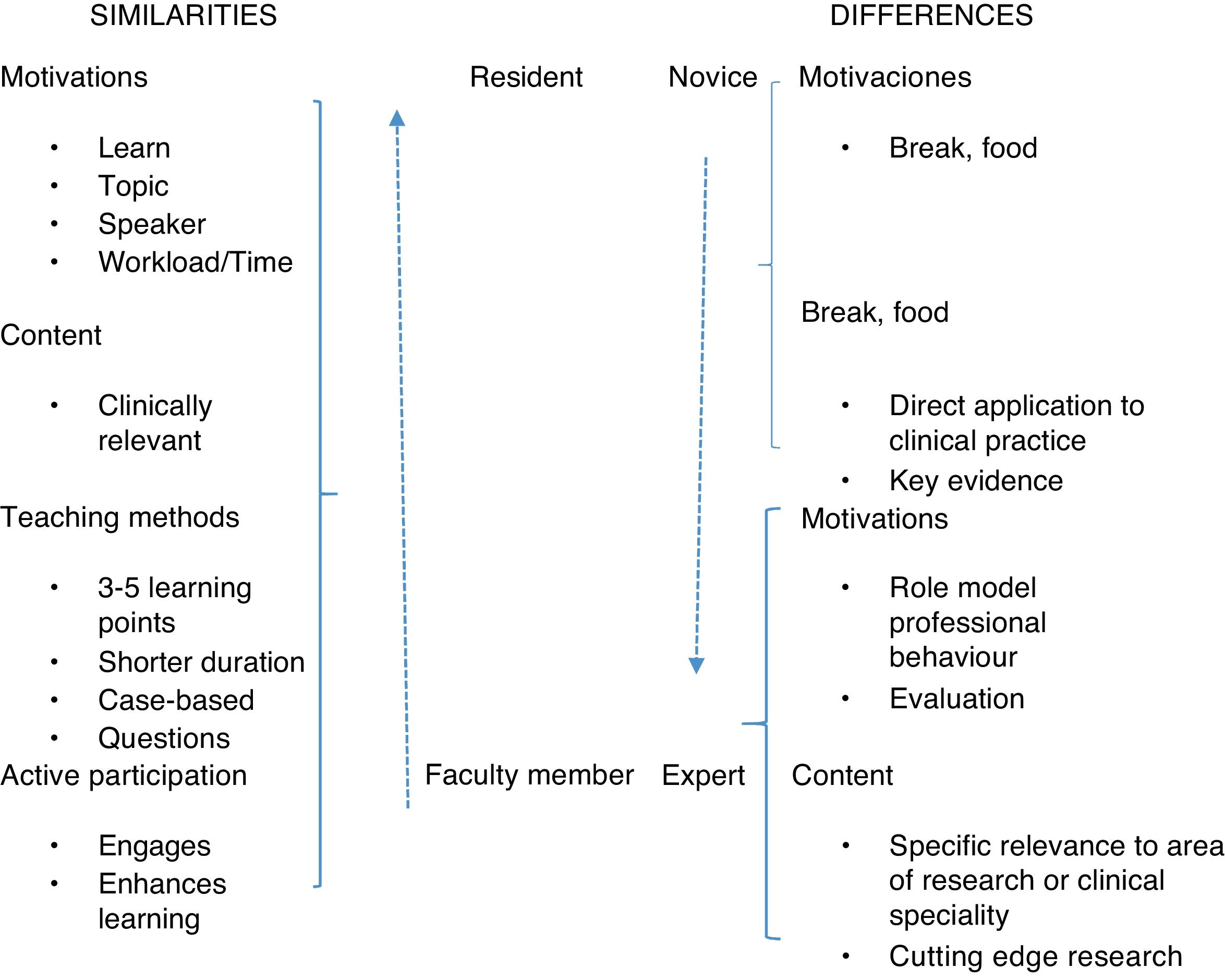
In order to meet the requirements of the Accreditation Council for Graduate Medical Education (ACGME) on knowledge competencies through lectures taken by internal medicine residents of a particular institution, focus groups were held with specialists and sub-specialists about barriers to and preferences for learning in the lectures; barriers related to the environment, the department staff and those of the actual residents were determined, and finally differences and similarities with regard to the faculty members were established. The results may be taken as recommendations emerging from the experience of learning through lectures which can transform, making the residents real learners23 (Fig. 2).

Similarities and differences in learning preferences between residents and faculty members.
One of the advantages of GT is that this method allows us to interpret complex phenomena, such as those typical in healthcare; the fact that GT can be adapted to multiple settings, researchers and purposes makes it a versatile tool, and it is an appropriate method for socially constructed experiences, such as disease and health, access to and the use of services and technologies, and therapeutic adherence, to name but some. GT allows new explanations to emerge and is not limited to data that are meant to be confirmed in advance; it is not limited by a priori knowledge; it can also yield powerful concepts and theories and is useful when there are gaps in the literature. Moreover, qualitative and quantitative data can be integrated into this method.2
Thanks to its methodology and strategies, GT provides structured and explicit analytical tools and guidelines to study processes and is open to all possible theoretical understandings, linking alternative data interpretations through coding and categorising, and it builds systematic checks, refining the researcher's major categories.2
One of the biggest advantages of GT is that it can be adopted by researchers with different theoretical perspectives, with different objectives, in fields as varied as social justice research, policy analysis and organisational, social and psychological studies, and in clinical health, preventive medicine, nursing, etc.2
LimitationsIn terms of limitations, the GT method may be said to be costly, in view of the structure and steps involved, which include successive data reviews in the attempt to leverage them and to achieve a description that produces a theory or explanation; while this is a limitation, most research results depend on a rigorous analysis, which takes time and effort.24
The emergence of many inductive categories can complicate the analysis, as their emergence cannot and should not be controlled.
It may be difficult to actually construct a theory when there are few data or infrequent categories, rendering it necessary to analyse extreme values (outliers).
This method requires experience and skill in qualitative methods, and any existing prejudices must be effectively and permanently set aside,25 as the analysis could be biased by the researcher's “blindness”. One way to combat this is by reviewing the data and triangulating information, since, as von Foerster said in the blind spot metaphor, “we do not see that we do not see”.26
Often times no theory is ever developed, only descriptions, thus rendering the initial intention unfulfilled.
The use of a GT-specific language renders it difficult for researchers who are accustomed to other methods to understand it initially, to say nothing of for the reader; while it is necessary for the process, it has been referred to as “methodological and self-confirming rhetoric”.4
FutureGT may be seen to be headed in three directions: firstly, it is becoming more international and multidisciplinary in all its variants; the second is the turn towards research in social justice and areas of social policy; thirdly, there is the fact that mixed-method researchers are leveraging it as a useful qualitative method.2
Due to its explanatory power, GT has a huge appeal for a range of different disciplines and enables people to identify with the theory and use it in their own lives.12 With the movements towards the participation of users and minorities, GT has a fertile field for the development of healthcare research.
Given that in classic GT, researchers identify their ontological and epistemological stance, which in turn makes it easier for them to set aside their beliefs,12 it maintains an objectivity consistent with the positivist paradigm of science and can achieve acceptance in mixed methods of health research.
Constructivism, which emphasises the subjective interrelation between the researcher and the participant, and the joint construction of meaning (co-construction),27,28 is a field that GT has also developed and in which challenges are envisaged. Given that in this vision the researchers are part of the research, rather than external observers,12,16,29 this contrasts with the vision of the external researcher outside the process being observed. The development of this epistemology is a particular challenge for research in clinical medicine, perhaps with greater acceptance among researchers with training in the social sciences.
In recent years, GT has been applied in mental health research, although its use in that field has been questioned, as the method is based on social, and not individual, processes, and it can be reduced to being merely a systematic categorisation technique, forgetting the nature of the individual experiences.12
GT does not seek to produce formal theories, but rather to theorise about very specific problems that could acquire a higher category as new studies from other substantial areas are added; the researcher does not intend to prove their ideas by generating GT, but rather only to demonstrate that they are plausible19 and can assist other approaches, processes and areas, such as psychometrics, epidemiology and public health.
Given that the clinician has access to patients, and that social science researchers have more difficulty in this regard,28 there is a field of development specifically for healthcare personnel to carry out research applying the GT method. However, for this purpose clinical researchers’ skills in qualitative techniques, including GT, must be improved, as this would render it possible generate a greater body of knowledge from daily practice on topics such as diseases and unusual situations, the use of health services, treatment adherence, the role of the family in health-disease processes, etc.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: de la Espriella R, Gómez Restrepo C. Teoría fundamentada. Rev Colomb Psiquiatr. 2020;49:126–132.
