





Behçet's disease is defined as a vasculitis affecting all types of vessels, presenting with local and systemic clinical manifestations that may involve concern any organ or organ system.
ObjectiveTo describe the clinical and epidemiological behavior of Behçet's disease in Cuba.
MethodsAn observational, longitudinal, retrospective, and descriptive study was conducted on a group of 8 patients with Behçet's disease, who were evaluated and followed-up by the National Rheumatology Centre of the “10 October” Clinical Surgical Hospital, Havana, Cuba.
ResultsThe mean age of the 8 patients (6 women and 2 men) found was 47±17 years old. The most common clinical manifestations were oral (100%) and genital (100%) ulcers, and bone, muscle and joint system involvement, followed by psychological disorders (62.5%). An increased C-reactive protein (100%) was the most common laboratory finding. Colchicine (100%), combined with steroids and methotrexate (87.5%) is the most commonly treatment used.
ConclusionsThere was a predominance of females and patients over 40 years, with a higher incidence of general symptoms, oral and genital ulcers, arthralgia, arthritis, and psychological disorders. Combined therapy with steroids, methotrexate and colchicine was the most commonly found.
La enfermedad de Behçet se define como una vasculitis que afecta a vasos de cualquier calibre, cursa con manifestaciones clínicas locales y sistémicas que interesan cualquier órgano o sistema de órgano de la economía humana.
ObjetivoDescribir el comportamiento clínico epidemiológico de la enfermedad de Behçet en nuestro medio.
MétodosSe realizó un estudio observacional, longitudinal, retrospectivo, descriptivo de una serie de 8 pacientes con diagnóstico de enfermedad de Behçet, diagnosticados y seguidos en el Centro Nacional de Reumatología perteneciente al Hospital Clínico Quirúrgico «10 de Octubre», La Habana, Cuba.
ResultadosSe identificó a 8 pacientes (6 mujeres y 2 hombres) con una edad promedio±desviación estándar de 47±17 años. Las manifestaciones clínicas más frecuentes fueron las úlceras orales (100%) y genitales (100%), y la afectación del sistema osteomioarticular (100%), seguidas de los trastornos psicológicos (62,5%). La elevación de las cifras de proteína C reactiva (100%) fue el hallazgo de laboratorio más frecuentemente encontrado. El uso de colchicina (100%) combinado con esteroides y metotrexato (87,5%) es el esquema de tratamiento más utilizado.
ConclusionesPredominó el sexo femenino y la edad mayor de 40 años. Los síntomas generales, las úlceras orales y genitales, las artralgias, las artritis y los trastornos psicológicos son las manifestaciones que mayor incidencia presentaron. La combinación terapéutica más utilizada es el uso de esteroides, metotrexato y colchicina.
Rheumatic diseases include approximately 250 conditions, in their majority of autoimmune origin, characterized by the presence of pain, stiffness, systemic affectation, decreased perception of the quality of life and varying degrees of functional disability. Among these stand out, due to their variety and characteristics, the vasculitis and within them, Behçet's disease (BD) undoubtedly occupies a privileged place.1
BD is defined as a chronic multisystem disease of unknown cause, characterized by a recurrent course, which evolves in outbreaks and with inflammatory involvement of blood vessels of all calibers. Its first description was published by Hippocrates in the fifth century BC, after being described by the Turkish dermatologist Hulusi Behçet, after 17 years of studies of similar cases.2
A worldwide distribution is described; being reported more frequently in the countries corresponding to the antique Silk Road (Iran, Iraq, Uzbekistan, Turkmenistan, China and Turkey) and less frequently in Northern Europe and the United States. It is estimated that Turkey is the country with the highest incidence, with 80–420 cases per 100,000 inhabitants. In countries like Japan, Korea, China, Iran and Saudi Arabia it fluctuates between 13 and 22 cases per 100,000 inhabitants. In the American countries it has been reported as a rare disease.3,4
It is reported that BD mainly affects young adults between the third and fourth decades of life. In relation to the gender, is described that it varies from country to country; for example, in the Middle East of Asia, including Israel, Egypt and Turkey, is more common in males, with a ratio of 3–5 men for every woman; in the reports from Germany, Japan, the United States and Brazil is more frequent in women.2,5,6
It is described as a disease with a varied symptomatology, which can affect any organ or systems of organs of the human body. Although is stated that there is no specific laboratory test to establish its diagnosis, there are classification criteria whose greater usefulness is framed for academic an scientific purposes.7–19
Several authors describe the treatment of BD as symptomatic, but being an affection of autoimmune origin, the use of immunosuppressive drugs is suggested. Anti-inflammatory drugs and corticosteroids are reported as other medications commonly used. Recently, the use of biological drugs is reported, but the published studies on the subject are scarce and with small numbers of patients.16–18 The variety and non-specificity of symptoms and signs, the lack of knowledge of the disease, as well as the non-existence of specific laboratory tests and curative treatment, make the BD a rare, disabling and incapacitating disease, of difficult diagnosis, that causes a considerable decrease in the perception of the quality of life of the patients who suffer from it. That is why, taking into account the low frequency with which this condition occurs, the great diversity of signs of symptoms, the non-specificity of the complementary exams for its diagnosis and the scarce existence of reports of this entity, it was decided to undertake this work in order to describe the clinical epidemiological behavior of BD in our environment, which will provide important elements when it comes to suspect and diagnose this condition.
MethodsAn observational, longitudinal, retrospective, and descriptive study was conducted, prior informed consent, in a group of 8 patients with diagnosis of BD, according to the criteria of the International Study Group for Behçet's disease, who were diagnosed and followed-up at the National Rheumatology Centre belonging to the “10 October” Clinical Surgical Hospital, Havana, Cuba, between January 2007 and December 2014, including only those patients with at least one year of follow-up, in order to identify the socio-demographic and clinical characteristics with which the disease occurred.
The review of the medical records of the patients included in the study allowed to obtain the clinical epidemiological variables, using a form designed for the research.
The data were processed and tabulated in an automated manner using the SPSS-PC statistical package in its version 18.5 for Windows. The results were analyzed through descriptive statistics, calculating measures of central tendency and dispersion for the continuous quantitative variables and estimating frequencies and percentages for the qualitative variables. The 95% confidence intervals were estimated to complete the point estimation of the above mentioned measures.
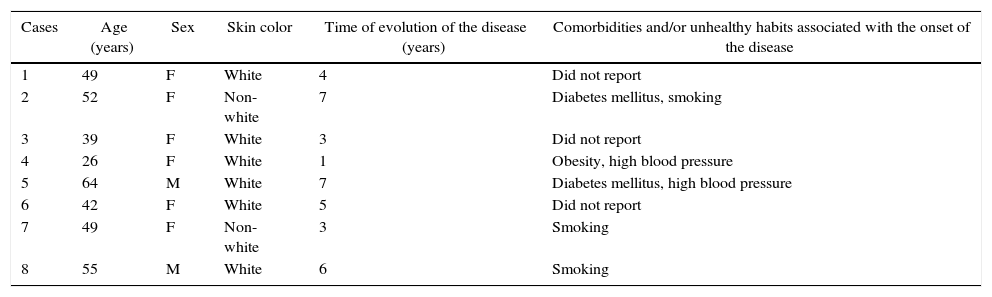
ResultsThe average age±standard deviation of the group of patients studied was 47±17 years, with an age of onset of the symptoms of 42.5 years and an average evolution of the disease of 4.5 years. There is a greater representativeness of women (75%) and of the white skin color (75%). Five of the 8 patients with diagnosis of BD (62.5%) referred comorbidities or unhealthy habits at the beginning of the disease (Table 1).
Distribution of patients with Behçet's disease according to socio-demographic characteristics. National Rheumatology Centre, 2007–2014.
| Cases | Age (years) | Sex | Skin color | Time of evolution of the disease (years) | Comorbidities and/or unhealthy habits associated with the onset of the disease |
|---|---|---|---|---|---|
| 1 | 49 | F | White | 4 | Did not report |
| 2 | 52 | F | Non-white | 7 | Diabetes mellitus, smoking |
| 3 | 39 | F | White | 3 | Did not report |
| 4 | 26 | F | White | 1 | Obesity, high blood pressure |
| 5 | 64 | M | White | 7 | Diabetes mellitus, high blood pressure |
| 6 | 42 | F | White | 5 | Did not report |
| 7 | 49 | F | Non-white | 3 | Smoking |
| 8 | 55 | M | White | 6 | Smoking |
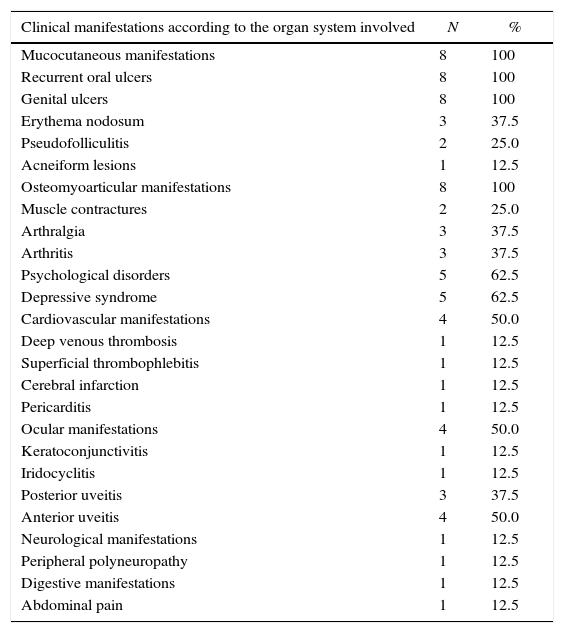
The most representative clinical manifestations were mucocutaneous (100%) and osteomyoarticular (100%), followed by psychological disorders, which occurred in 62.5%. In an individual manner, oral (100%) and vaginal (100%) ulcers and the depressive syndrome (62.5%) were those of greater representativeness (Table 2).
Distribution of patients with Behçet's disease according to the presence of clinical manifestations and the organ system involved. National Rheumatology Centre, 2007–2014.
| Clinical manifestations according to the organ system involved | N | % |
|---|---|---|
| Mucocutaneous manifestations | 8 | 100 |
| Recurrent oral ulcers | 8 | 100 |
| Genital ulcers | 8 | 100 |
| Erythema nodosum | 3 | 37.5 |
| Pseudofolliculitis | 2 | 25.0 |
| Acneiform lesions | 1 | 12.5 |
| Osteomyoarticular manifestations | 8 | 100 |
| Muscle contractures | 2 | 25.0 |
| Arthralgia | 3 | 37.5 |
| Arthritis | 3 | 37.5 |
| Psychological disorders | 5 | 62.5 |
| Depressive syndrome | 5 | 62.5 |
| Cardiovascular manifestations | 4 | 50.0 |
| Deep venous thrombosis | 1 | 12.5 |
| Superficial thrombophlebitis | 1 | 12.5 |
| Cerebral infarction | 1 | 12.5 |
| Pericarditis | 1 | 12.5 |
| Ocular manifestations | 4 | 50.0 |
| Keratoconjunctivitis | 1 | 12.5 |
| Iridocyclitis | 1 | 12.5 |
| Posterior uveitis | 3 | 37.5 |
| Anterior uveitis | 4 | 50.0 |
| Neurological manifestations | 1 | 12.5 |
| Peripheral polyneuropathy | 1 | 12.5 |
| Digestive manifestations | 1 | 12.5 |
| Abdominal pain | 1 | 12.5 |
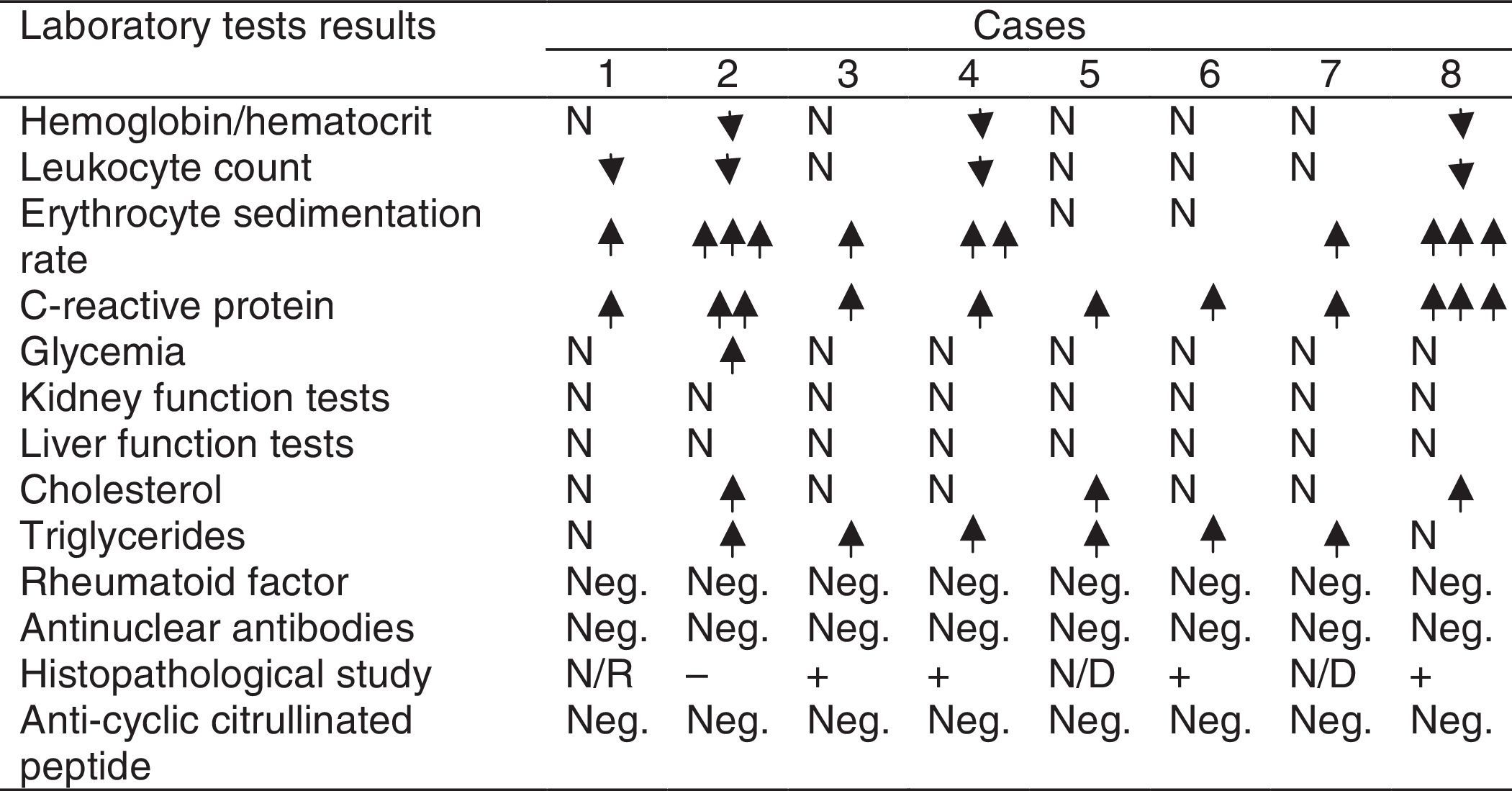
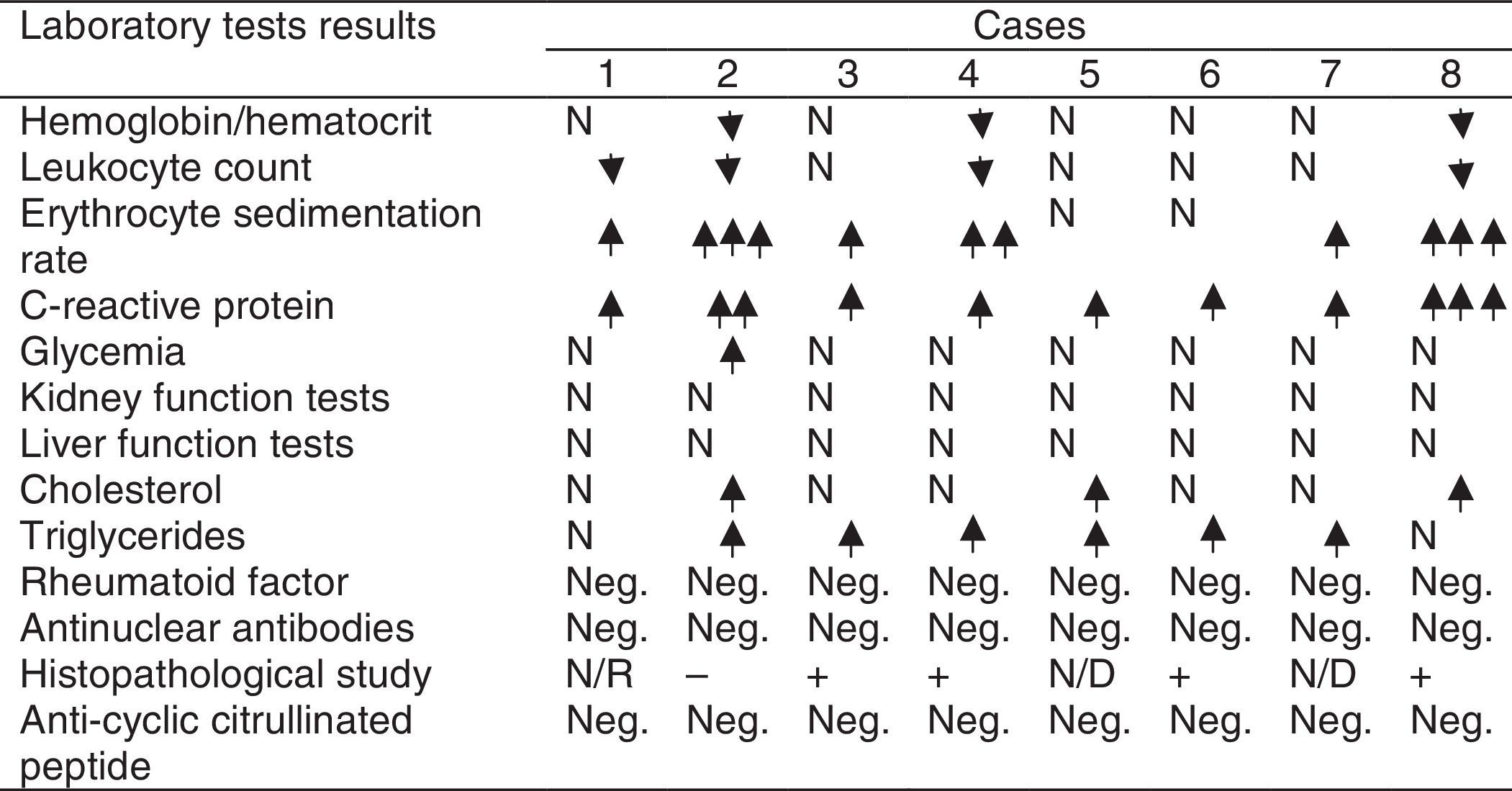
The most significant laboratory findings were the elevation of C-reactive protein (100%), accelerated erythrocyte sedimentation rate (75%) and hypertriglyceridemia (75%); followed by leukopenia (50.0%) and anemia (37.5%) (Table 3). The anatomopathological studies evidenced data of the histopathological alterations described in BD in 4 out of 5 patients (80%) from whom the specimen was collected.


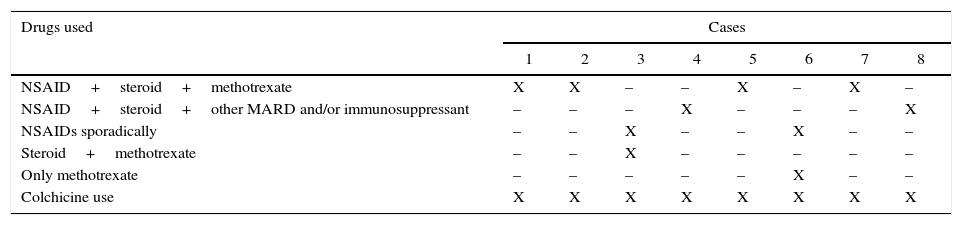
Colchicine (100%), steroids (87.5%) and methotrexate (87.5%) were the drugs most commonly used by the patients, either individually or in combination, to treat their disease (Table 4).
Distribution of patients with Behçet's disease according to the therapeutic scheme used at the time when the study was conducted. National Rheumatology Center, 2007–2014.
| Drugs used | Cases | |||||||
|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
| NSAID+steroid+methotrexate | X | X | – | – | X | – | X | – |
| NSAID+steroid+other MARD and/or immunosuppressant | – | – | – | X | – | – | – | X |
| NSAIDs sporadically | – | – | X | – | – | X | – | – |
| Steroid+methotrexate | – | – | X | – | – | – | – | – |
| Only methotrexate | – | – | – | – | – | X | – | – |
| Colchicine use | X | X | X | X | X | X | X | X |
BD is described as a systemic, chronic, inflammatory and recurrent disease characterized by affecting vessels of any caliber. In this study is reported a median age of onset of symptoms of 42 years, behaving slightly above the peak of frequency with which its appearance is reported in other studies, which include it between 20 and 40 years; there was a predominance of the female gender, white skin color and increased presence of comorbidities or unhealthy habits, results that coincide with those described in the literature.2,20,21
López de Maturana et al. and Baixauli et al. describe a predominance in male patients; a study conducted in Colombia in 2009, in a cohort of 20 patients with BD, reports a female predominance of 3:1 in comparison to men; other reports from Germany, Brazil and the United States also show a female predominance; in this research is seen that women are more affected, which coincides with these reports in the literature.5,20,21 Likewise, it was identified a high presence of comorbidities or associated unhealthy habits, which has been reported by other authors.22
As predominant clinical manifestations are described the recurrent oral ulcers (3 or more appearances in one year), genital ulcers and osteomyoarticular manifestations, which were reported in all patients. Oral ulcers are reported by other authors such as Toro Giraldo et al. as the most common clinical manifestation and the most frequent sign of onset of BD, being reported in 97% of patients studied by them, thus confirming their clinical significance at the time of suspicion of this disease.21,23 Regarding the genital ulcers, they have been reported with a frequency of occurrence ranging between 72% and 94% of cases, being considered the initial symptom of the disease in 1 out of every 10 patients.20,24–27 Other cutaneous affections reported with less frequency of occurrence include pseudofolliculitis, acneiform lesions and erythema nodosum, which is in line with other works that report a similar frequency of occurrence.2,3,20,23,25
Articular manifestations (arthritis, arthralgia and muscle contractures) were reported by all the studied patients. This result is consistent with the reports of Castillo-González et al., López de Maturana et al. and Ozkan et al., among others, which underscore the articular affection in BD, although they are not part of its diagnostic criteria.2,5,28,29
Psychological disorders (62.5%) were frequently reported by the patients, which could be related to the esthetic affectation, the diminished perception of the quality of life and the degrees of functional disability generated by BD. Depression was the most representative psychological disorder. No reports are found in the literature relating to the incidence of psychological disorders in patients with this disease.25
Among the systemic manifestations most commonly reported stand out the ocular and cardiovascular affectations; both occurred in half of the studied patients. The ocular manifestations, reported as serious by other authors, were led by the presence of anterior and posterior uveitis, and to a lesser extent by the appearance of keratoconjunctivitis and iridocyclitis. Other studies report percentages of affectation ranging between 29.1% and 76.2%. The Colombian study reported a higher incidence of anterior uveitis in men and of retinal vasculitis in women.21,25–28
Other manifestations reported in this research include the presence of neurological manifestations, given by peripheral polyneuritis, but in low percentages. This data is consistent with the reviewed literature, which presents low percentages of occurrence thereof.3,20,21,24 Gastrointestinal manifestations were present only in one case, but they have been reported in up to half of the patients with BD.20,24,30–32 The laboratory findings show high percentages of elevation of C-reactive protein, acceleration of the erythrocyte sedimentation rate and hypertriglyceridemia, which can be observed in other rheumatic conditions, perhaps due to the presence of the sustained inflammatory process and the resulting oxidative stress.21 No studies showing results in this regard are reported.
Like in other reports, colchicine, steroids and methotrexate are the drugs most frequently used, either individually or combined, for the treatment of BD.21,24,33–35 BD occasionally tends to have a benign course, otherwise it can affect different organs which will compromise the future evolution of the patient; that is why it is considered of vital importance to bring to light the clinical and socio-demographic characteristics of this affection with the aim of increasing the level of knowledge thereof by the medical and paramedical staff, as well as by the patients themselves.
ConclusionsIn our environment, BD occurred more frequently in women and in patients older than 40 years. The appearance of general symptoms, oral and genital ulcers, as well as the presence of involvement of the osteomyoarticular system, are the clinical manifestations that showed a higher incidence. Elevation of the C-reactive protein levels, acceleration of the erythrocyte sedimentation rate and hypertriglyceridemia were the most significant laboratory findings. The treatment with steroids, methotrexate and colchicine is the most commonly used therapeutic combination.
Ethical disclosuresProtection of human and animals subjectsThe authors declare that no experiments were performed on human beings or animals for this research.
Confidentiality of dataThe authors declare that they have followed the protocols of their workplace on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the informed consent from patients and/or subjects referred in the article. This document is held in the possession of the corresponding author.
Conflict of interestThe authors declare that they have no conflict of interest.
Please cite this article as: Solis Cartas U, Barbón Pérez OG, Bascó EL, Muñoz Balbín M, Molinero Rodríguez C, Solis Cartas E. Comportamiento clínico epidemiológico de la enfermedad de Behçet. Rev Colomb Reumatol. 2016;23:79–84.
