














Rheumatoid arthritis (RA) is a high-cost disease, which allows patients to be classified into early or established phase approaches.
ObjectiveThe purpose of this work was to perform a cost-effectiveness analysis comparing both phases with patient data at a 6-month time horizon from a third-party payer perspective.
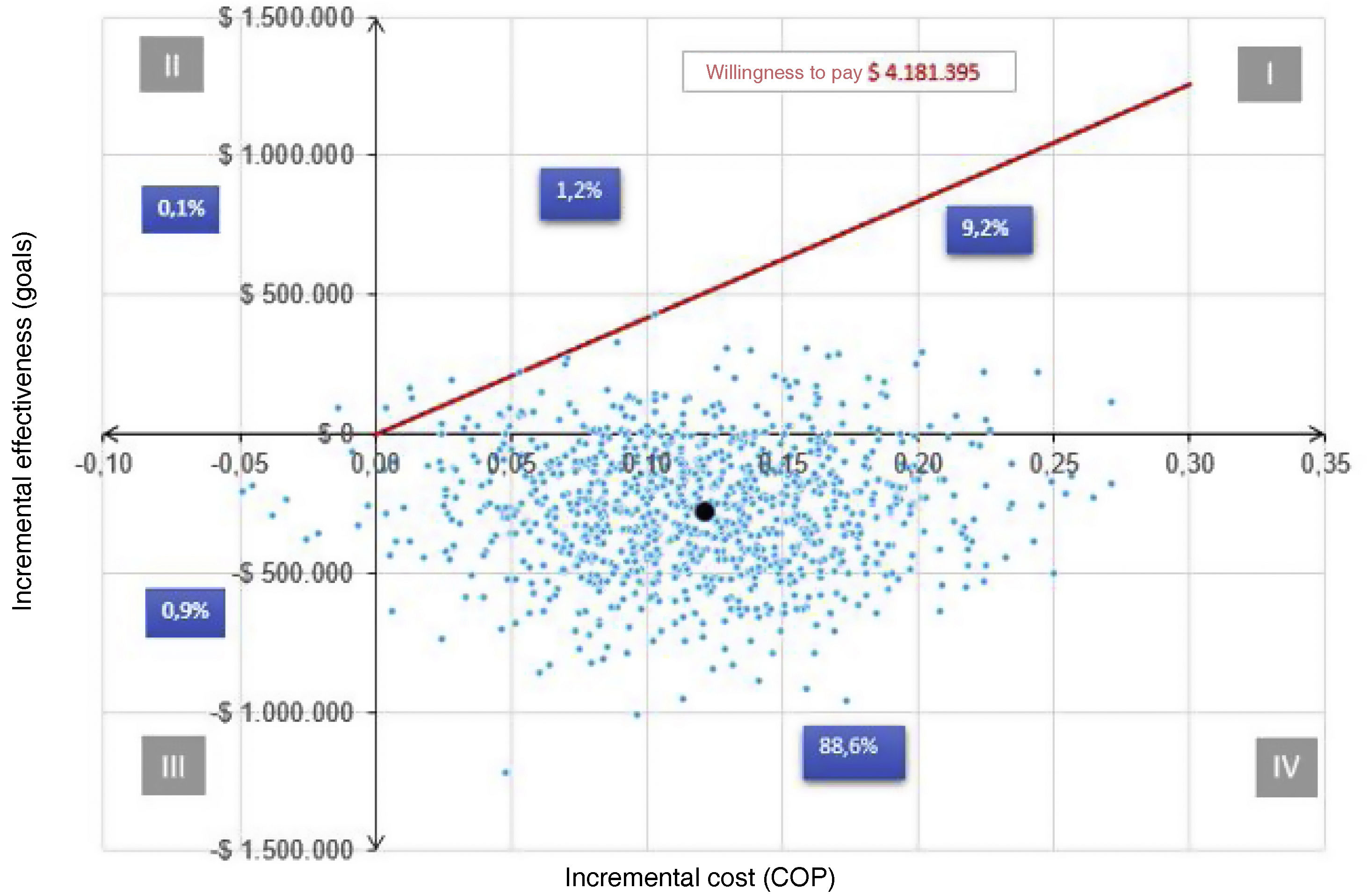
Materials and methodsThe population was delimited. The costs and effectiveness of each of the phases were estimated. A decision tree-type economic evaluation model was developed, and the Incremental Cost-Effectiveness Ratio (ICER) was calculated with the respective sensitivity analyses, both deterministic and probabilistic.
ResultsIn terms of costs, it was found that for effectiveness in goals, the cost was 85% higher in the established than in the early phase. Similarly, for non-target effectiveness, the cost was 77% higher in the established than in the early phase. On the other hand, the effectiveness results were better in the early phase compared to the established phase. Regarding the ICER, it was determined that the early phase approach saves $2,326,389 COPcte (colombian pesos current currency) per patient in goals at 6 months of treatment, compared to the established phase approach.
ConclusionThe clinical approach to early-stage rheumatoid arthritis is a less costly and more effective alternative vs. the established phase, as it generates savings for the third-party payer over a 6-month time horizon, from a third-party payer perspective.
La artritis reumatoide (AR) es una enfermedad de alto costo, que permite clasificar a los pacientes en fase temprana o establecida.
ObjetivoEl propósito de este trabajo fue hacer un análisis de costoefectividad, comparando ambas fases con datos de pacientes a un horizonte temporal de 6 meses, desde la perspectiva del tercer pagador.
Materiales y métodosSe delimitó la población. Se estimaron los costos y las efectividades de cada una de las fases. Se desarrolló un modelo de evaluación económica de tipo árbol de decisión y se calculó la razón incremental costoefectividad (RICE) con sus respectivos análisis de sensibilidad, tanto determinístico como probabilístico.
ResultadosEn términos de costos, se encontró que para una efectividad en metas el costo fue un 85% mayor en fase establecida que en fase temprana. Igualmente, para una efectividad en no metas, el costo fue un 77% mayor en fase establecida que en fase temprana. Por otra parte, los resultados de efectividad salieron a favor de la fase temprana en comparación con la fase establecida. Con respecto a la RICE, se determinó que el abordaje en fase temprana ahorra $2.326.389 COPcte (pesos colombianos moneda corriente) por paciente en metas a los 6 meses de tratamiento, en comparación con el abordaje en fase establecida.
ConclusiónEl abordaje clínico de la artritis reumatoide en fase temprana es una alternativa menos costosa y más efectiva vs. la fase establecida, ya que genera ahorros para el tercer pagador en un horizonte temporal de 6 meses, desde la perspectiva del tercer pagador.
