






To describe the journey of patients with psoriatic arthritis (PsA), and psoriasis (PsO) with special emphasis on diagnosis and treatment delays.
Materials and methodsAll patients with PsA registered between 2000 and 2016 were included. Mean lag time between first musculoskeletal symptom and diagnosis of PsA, between first musculoskeletal symptom and first physician encounter, mean lag time to first DMARD and mean lag time between PsO diagnosis and PsA diagnosis were calculated. Descriptive statistics are reported. Variables associated with a delay in PsA diagnosis >1 year were analyzed in multivariable analysis.
ResultsOne hundred and eighty nine patients were included (139 PsA and 50 PsO), mean age 60.8 years (SD: 16.3), 57% were males. Mean lag time between first musculoskeletal symptom and diagnosis of PsA was 1.9 (SD: 4.7) years. In 90 patients (97%), the diagnosis of PsO preceded the diagnosis of PsA, a mean time of 14.3 years (SD: 13.9). Forty-nine patients (35%) had a delay of PsA diagnosis ≥1 year. Of the PsA patients, 84.7% received cDMARDs as first line therapy. The mean lag time between PsA diagnosis and initiation of DMARDs was 2 years (SD: 7.6). In logistic regression analysis no variable was independently associated with a delay equal or greater than 1 year in PsA diagnosis.
ConclusionsA significant delay in consultation and diagnosis of PsA was evident in this single center study in a third of patients. None of the variables studied was associated with a delay in diagnosis greater than one year.
Describir el recorrido de los pacientes con artritis psoriásica (PsA) y psoriasis (PsO), con especial énfasis en los retrasos en el diagnóstico y en el tratamiento.
Materiales y métodosSe incluyeron todos los pacientes con PsA registrados entre el año 2000 y el año 2016. Se calculó el tiempo medio entre el primer síntoma musculoesquelético y el diagnóstico de PsA, el tiempo medio al primer encuentro con el médico, el tiempo medio del primer DMARD y el tiempo medio entre el diagnóstico de PsO y el diagnóstico de PsA. Se reportan estadísticas descriptivas y análisis multivariable para un retraso diagnóstico superior a un año.
ResultadosSe incluyeron 189 pacientes (139 PsA y 50 PsO), con una edad media de 60,8 años (DE: 16,3), el 57% del sexo masculino. El tiempo medio de retraso entre el primer síntoma musculoesquelético y el diagnóstico de PsA fue de 1,9 años (DE: 4,7). En 90 pacientes (97%), el diagnóstico de PsO precedió al diagnóstico de PsA, con un tiempo medio de 14,3 años (DE: 13,9). Cuarenta y nueve pacientes (35%) tuvieron un retraso en el diagnóstico de PsA superior a un año. El 84,7% de los pacientes con PsA recibieron FARMEc como terapia de primera línea, con un retraso medio de 2 años (DE: 7,6). En el análisis de multivariable ninguna variable se asoció de forma independiente con un retraso superior a un año en el diagnóstico de PsA.
ConclusionesEvidenciamos un retraso significativo entre la consulta y el diagnóstico de PsA en un tercio de los pacientes. Ninguna variable se asoció con un retraso en el diagnóstico superior a un año.
Psoriatic arthritis is a severe disease, 67% of patients present at clinic with erosive disease, in the first two years, 47% of patients present at least one radiographic erosion, and after 12 years of follow up, 74% of patients evidence radiographic damage.1,2 Patients with psoriatic arthritis are at increased risk of death compared with the general population. A delay in diagnosis and treatment of PsA is associated with increased disability and damage in the long term.3–6
It has been shown that there is a significant delay in the diagnosis of PsA. In a survey performed in US, Canada and Europe, an average of 5 years elapsed between sign/symptom onset and diagnosis. In the same survey the authors found that 47% of patients with psoriasis (PsO) had not seen a health care provider (HCP) within last 12 months for their PsO. Also, of the patients with PsO who had seen an HCP within last 12 months, only 55% saw a dermatologist.7,8 Around 22% of patients with PsA, had not seen a HCP in the last 12 months, and among those patients who had seen an HCP only 37% saw a rheumatologist.7,8 In another study in Denmark, mean duration from initial symptoms to diagnosis for RA, PsA and AS declined steadily from 30, 53 and 66 months (year 2000), respectively, to 3–4 months (year 2011). So it is important to understand where the delay is occurring to plan the right measures to solve the problem. More recently Odgie et al. in US found that 32% of patients answering a survey had a diagnosis delay of more than 5 years.9
In rheumatoid arthritis different origin and cultures are influencing factors in delay in consulting a general practitioner (GP), as they might have different perception of their symptoms and different knowledge of the disease.10
There is currently no data available about diagnosis delay, physicians visited for the initial symptoms, referrals delays, and finally time to first treatment in patients with PsA in Argentina, and very scarce data in Latin America.
The objective of our study was to describe the journey on average, of patients with psoriasis and psoriatic arthritis, since the start of their psoriasis, with special emphasis on diagnosis and treatment delays.
Patients and methodsThis single center study used a retrospective cohort study design. The study was performed at a large University Hospital.
All patients with PsA registered in the Rheumatology Unit data base were included. This registry includes all patients from the Hospital Italiano Health Management Organization (HI-HMO) with the diagnosis seen at the Rheumatology Unit. The electronic medical records (EMR) were manually revised, and the following data was obtained: Date of first visit to a dermatologists due to PsO symptoms, date of PsO diagnosis as reflected in the electronical medical record, date and type of first musculoskeletal symptom, physician specialty seen and date of first visit, related to musculoskeletal symptoms., date of PsA diagnosis, as reflected in the electronical medical record.
For inclusion criteria patients must have the diagnosis of PsA performed by a rheumatologist and/or of PsO by a dermatologist and be affiliated to the HI-HMO. Patients affiliated to this HMO have been shown in previous studies to be representative of Buenos Aires city population.11–13 There were no exclusion criteria.
In a similar way consecutive patient with psoriasis sent for an ultrasound study (n=50) were included and evaluated and the same data was obtained from these patients. All these patients have been evaluated for the presence of PsA, and patients with PsA were excluded from this part of the analysis.
Data sourceData was obtained from the Hospital Italiano electronic medical records. All medical encounters, laboratory tests, medical procedures, and imaging studies, are registered in the electronic medical record since year 2000.14–18 All data was entered in a newly, built database on Microsoft Access 2016, with check system for data discrepancies.
Statistical analysisBeing an observational study, sample size calculation was not performed. All PsA patients in the Unit data base were included in the statistical analysis. Descriptive statistics of patients’ characteristics was performed. Continuous variables are described as means and standard deviation (SD), or medians and interquartile ranges (IQRs), according to the variable distribution. Categorical variables are reported as proportions with their 95% confidence intervals (CIs).
Continuous variables were compared with Student t test or Mann–Whitney U test according to their distribution, and categorical variables were compared with χ2 test.
We calculated time elapsed between first musculoskeletal symptom and diagnosis of PsA, first medical appointment, first visit to a rheumatologist, and prescription of the first cDMARD (conventional Disease Modifying anti-Rheumatic Drug) and to first bDMARD (biologic Disease Modifying anti-Rheumatic Drug). Logistic regression analysis was used to evaluate variables associated with a diagnosis delay greater than one year.
STATA 14 software (StataCorp LLC, College Station, TX) was used for statistical analysis.
Ethical considerationsThis study was performed according to the guidelines of Good Clinical Research Practices in Humans, contemplated in 2007 National Health's Ministry legal provision (1490 provision) and in Personal Data Protection's law, and according to WMA declaration of Helsinki – ethical principles for medical research involving human subjects. The study project was approved by Hospital Italiano de Buenos Aires's Independent Ethics Committee prior to the study startup. As the study was retrospective, no patient's information consent was required by the ethics committee.
ResultsA total of 189 patients were included (139 PsA and 50 PsO), mean age 60.8 years (SD: 16.3), 57% were males. General characteristics are summarized in Table 1. Mean lag time between first musculoskeletal symptom and diagnosis of PsA was 1.9 (SD: 4.7) years (median: 0.45 (IQR: 0.14–1.7 years)). Mean age at time of PsA diagnosis was 52 years (SD: 14.8). In 90 patients (97%), the diagnosis of PsO preceded the diagnosis of PsA, a mean time of 14.3 years (SD: 13.9). Mean lag time between first musculoskeletal symptoms and visit to a physician because of those symptoms was 1 years (SD: 2.3) [median: 0.125 (IQR: 0.02–0.97) years]. Forty-nine patients (35%) had a delay on PsA diagnosis equal or greater than 1 year. In 44% of the cases the first specialist seen was a rheumatologist. The most common musculoskeletal symptom was arthralgia (45%), followed by arthritis (42%), enthesitis/tendinitis (5%), low back pain (3%), and dactylitis (4.3%). One hundred and twenty-seven patients (67%) received cDMARDs as first line therapy, 117 because of PsA. Among patients with PsA 84.7% received cDMARDs. No patient received bDMARD as first line therapy. Only 20% of patients with PsO were treated with cDMARDs. Drugs used are summarized in Table 2. The mean lag time between PsA diagnosis and initiation of DMARDs was 2 years (SD: 7.6) (median: 0.02 (IQR: 0–0.36) years). After first treatment failure in PsA, the most common behavior was to switch to a biologic treatment (23%) (Table 2), followed by switching to another cDMARD (27%: leflunomide: 14.4%; methotrexate: 8.6%; and sulfasalazine: 4.3%). Adding another cDMARD was infrequent: leflunomide was added in 4.4% of the cases and sulfasalazine in 1 (0.74%). Switching to other cDMARD was not done in PsO patients (Table 2). Mean lag time to receive a biologic was 6.1 years (SD: 4.7) for patients with PsA, and time to receive a biologic was 21.7 and 24.1 years respectively for the only two patients with PsO that received biologics. In logistic regression analysis, including age, sex, specialist first seen, and type of musculoskeletal symptom, none was independently associated with a delay equal or greater than 1 year in PsA diagnosis (Table 3).
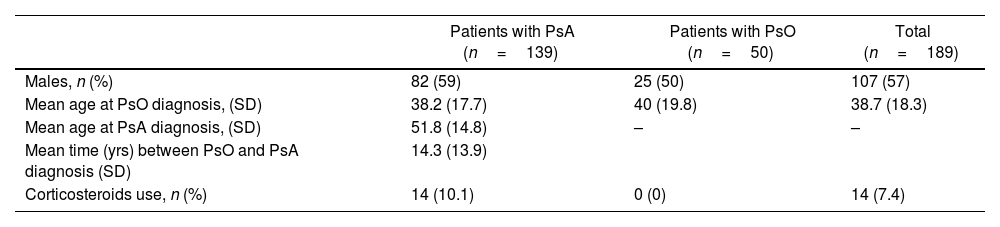
Demographic characteristics of patients included.
| Patients with PsA (n=139) | Patients with PsO (n=50) | Total (n=189) | |
|---|---|---|---|
| Males, n (%) | 82 (59) | 25 (50) | 107 (57) |
| Mean age at PsO diagnosis, (SD) | 38.2 (17.7) | 40 (19.8) | 38.7 (18.3) |
| Mean age at PsA diagnosis, (SD) | 51.8 (14.8) | – | – |
| Mean time (yrs) between PsO and PsA diagnosis (SD) | 14.3 (13.9) | ||
| Corticosteroids use, n (%) | 14 (10.1) | 0 (0) | 14 (7.4) |
PsA: psoriatic arthritis; PsO: psoriasis; yrs: years; SD: standard deviation; n: number.
First and second line treatment in patients with psoriatic arthritis (PsA), and psoriasis (PsO).
| PsA (n=139) | PsO (n=50) | Total (189) | |
|---|---|---|---|
| First line | |||
| Use of cDMARDs, n (%) | 117 (84.7) | 10 (20) | 127 (67) |
| Methotrexate, n (%) | 106 (77) | 9 (18) | 115 (61.5) |
| Sulfasalazine, n (%) | 5 (3.6) | – | 5 (2.7) |
| Leflunomide, n (%) | 5 (3.6) | – | 5 (2.7) |
| Cyclosporine, n (%) | 1 (0.73) | 1 (2) | 2 (1.1) |
| Second line | |||
| Switch to bDMARD, n (%) | 33 (23.74) | 2 (4) | 35 (18.5) |
| TNFi, n (%) | 32 (23) | 2 (4) | 34 (18) |
| Secukinumab, n (%) | 1 (1) | 0 (0) | 1 (0.53) |
| Combo bDMARD+cDMARD, n (%) | 11 (35.48) | 1 (50) | 12 (36.46) |
| Switch to methotrexate, n (%) | 12 (8.6) | 0 (0) | 12 (6.63) |
| Switch to sulfasalazine, n (%) | 6 (4.3) | 0 (0) | 6 (3.3) |
| Switch to leflunomide, n (%) | 20 (14.4) | 0 (0) | 20 (11) |
| Add sulfasalazine, n (%) | 1 (0.74) | 0 (0) | 1 (0.6) |
| Add leflunomide, n (%) | 6 (4.4) | 0 (0) | 6 (3.39) |
cDMARD: conventional Disease Modifying anti-Rheumatic Drug; bDMARD: biologic Disease Modifying anti-Rheumatic Drug; n: number; TNFi: tumor necrosis factor inhibitor.
Logistic regression analysis with diagnosis delay of PsA greater than 1 year as outcome.
| Variable | OR | 95% CI | P value |
|---|---|---|---|
| Age, years | 0.99 | 0.96–1.02 | 0.463 |
| Male sex | 1.3 | 0.53–3 | 0.604 |
| Use of cDMARDs | 2.23 | 0.6–8.1 | 0.225 |
| Use of bDMARDs | 1.4 | 0.49–3.8 | 0.541 |
| Seen by a rheumatologist | 2 | 0.8–4.8 | 0.121 |
OR: odds ratio; CI: confidence interval; cDMARD: conventional Disease Modifying anti-Rheumatic Drug; bDMARD: biologic Disease Modifying anti-Rheumatic Drug.
There is scarce information on diagnosis delay in PsA in Argentina and Latin America.19 Although we found that the median delay in diagnosis of PsA and initiation of treatment was acceptable, 35% of our patients had a delay greater than one year, way beyond the recommendations. One of the reasons for diagnosis delay is the underdiagnosis of PsA among patients with PsO attending dermatologic clinics that could reach up to 30% of the patients.20 This was unlikely the case in our study, as the medical records were reviewed in search of signs and symptoms of PsA even if the diagnosis was not consigned in the EMR.
Noticeably in our study almost all patients received the diagnosis of PsO before PsA. In the literature this figure is around 70–80%.20 There might be a selection bias in the way patients were selected to be included in our data base that could explain our larger percentage. Most of PsA and PsO patients were treated with cDMARDs, that is in accordance with current guidelines,21–23 and previous reports from other countries in LA.19 Unlikely other studies we were unable to find clinical or demographic characteristics associated with a greater delay in PsA diagnosis. This might be due to the low number of patients with a delay in diagnosis greater than one year included. This precludes us to suggest actions to improve ours delay. Nevertheless, closer relations with dermatologists and a combined dermatologist/rheumatologists clinic has been developed since this study to try to improve diagnosis and management of these patients.
In PsO patients the most frequent course of action after cDMARDs failure was to switch to bMDARD. This is also in accordance with current guidelines.21–23 The use of bDMARDs was rare in PsO patients. This might be because some dermatologists were less familiar with biologics use in our hospital, and more likely that more severe patients were included in randomized clinical trials and excluded from our study.
Our study has some limitations, it is a single center study, and data were collected retrospectively. This might induce selection and information bias and make the study less generalizable. On the other hand, the study has some strengths such as the use of a proven methodology of data collection, and a good number of patients.
In summary, a significant delay in consultation and diagnosis of PsA was evident in this single center study in almost a third of the patients. As none of the variables studied was associated with a delay in diagnosis, more studies are needed to identify potential actions that would help reducing this delay.
FundingThis study was supported by an unrestricted grant from Novartis.
Conflict of interestsE.R. Soriano received has been speaker, participated in advisory boards or received grants from Abbvie, Amgen, BMS, Glaxo, Janssen, Lilly, Novartis, Pfizer, Roche, Sandoz and UCB.
Martin Brom: currently works for Novartis. Sebastian Moyano: currently works for Lilly Spain. ML Acosta Felquer: has been speaker or participated in advisory boards for Abbvie, Janssen, and Novartis.
JE Rosa: has been speaker or participated in advisory boards for Abbvie, Amgen, BMS, Janssen, Lilly, Novartis, and Pfizer.
Supplementary material:
