




Our patient was a 79-year-old woman with a history of lymphoma in remission for 15 years, who had been scheduled for endoscopic exeresis of an internal nasal melanoma. The preoperative electrocardiogram showed a 2:1 atrioventricular block (Fig. 1A and B). She reported no previous episodes of syncope, and HR did not increase after administration of 0.01mg/kg atropine (iv). After consulting the cardiologist, it was decided to implant a permanent pacemaker, which was done within 24h, and was uneventful. Melanoma exeresis was performed 5 days later, with a good outcome.
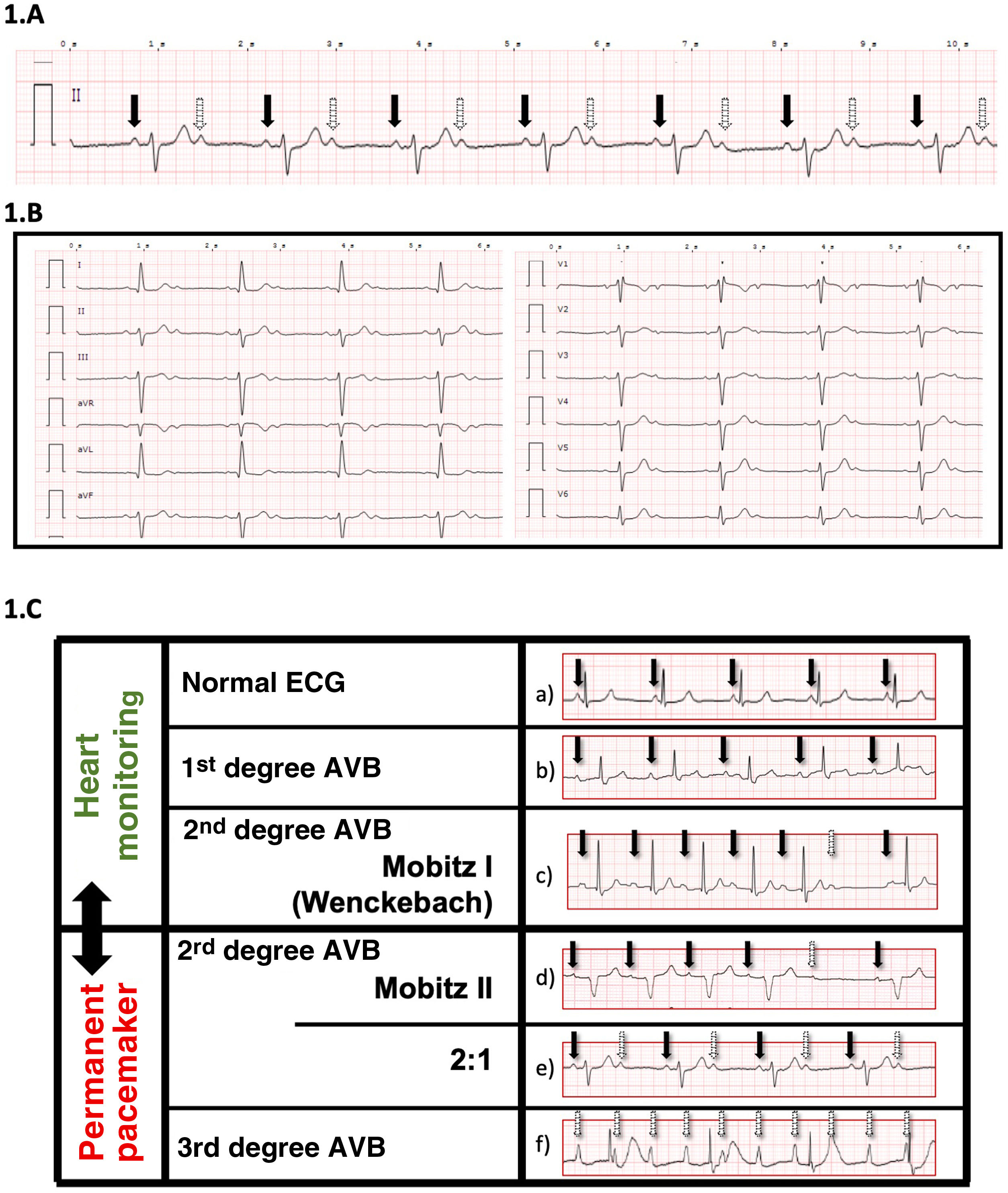
 (continuous arrow, conducting P wave; dotted arrow, non-conducting P wave); and in all bipolar leads. B) In most cases, this heart block is considered high risk for complete AVB and permanent pacemaker implantation is frequently indicated, particularly in the presence of a QRS with a bundle branch block pattern. In the event of a surgical emergency, the placement of a temporary pacemaker (electrocatheter) should be considered. Image C) shows lead DII of the ECG in different types of AVB. Pacemaker implantation prior to surgery is based on visual assessment. a) Normal ECG: all P waves conduct. PR<200 msg. b) 1st degree AVB: all P waves conduct. PR>200 msg. 2nd degree AVB: some P waves conduct. c) Mobitz I (Wenckebach): progressive lengthening of the PR interval until conduction block. d) Mobitz II: constant PR. Non-conducted P waves. e) Type 2:1: intermittent non-conducted P waves (1 conducts and another does not). Typically with HR of 40–50x’. f) 3rd degreed AVB (complete): non-conducted P wave. Usually with extreme bradycardia (30–35x’) and wide QRS. (Solid arrow, P-wave conducts; dotted arrow, P-wave does not conduct).")
ECG showing a 2:1 AVB in lead DII A) (continuous arrow, conducting P wave; dotted arrow, non-conducting P wave); and in all bipolar leads. B) In most cases, this heart block is considered high risk for complete AVB and permanent pacemaker implantation is frequently indicated, particularly in the presence of a QRS with a bundle branch block pattern. In the event of a surgical emergency, the placement of a temporary pacemaker (electrocatheter) should be considered. Image C) shows lead DII of the ECG in different types of AVB. Pacemaker implantation prior to surgery is based on visual assessment. a) Normal ECG: all P waves conduct. PR<200 msg. b) 1st degree AVB: all P waves conduct. PR>200 msg. 2nd degree AVB: some P waves conduct. c) Mobitz I (Wenckebach): progressive lengthening of the PR interval until conduction block. d) Mobitz II: constant PR. Non-conducted P waves. e) Type 2:1: intermittent non-conducted P waves (1 conducts and another does not). Typically with HR of 40–50x’. f) 3rd degreed AVB (complete): non-conducted P wave. Usually with extreme bradycardia (30–35x’) and wide QRS. (Solid arrow, P-wave conducts; dotted arrow, P-wave does not conduct).
Atrioventricular blocks can be asymptomatic, and are more common in the elderly. The routine performance of a preoperative electrocardiogram allows the medical team to diagnose this type of disorder and optimise the patient’s status to withstand surgical aggression. Second degree AV block, Mobitz II, are considered risky, and require implantation of a permanent pacemaker (Fig. 1C).
Authors/collaboratorsAll authors have participated in the conception, design and interpretation of the data. The authors have made a critical review of the intellectual content and have approved the version presented.
Please cite this article as: Tatjer I, Ruíz A, Guasch E, Sala-Blanch X. Bloqueos auriculoventriculares en el preoperatorio: a propósito de un paciente con bloqueo tipo 2:1. Rev Esp Anestesiol Reanim. 2022;69:380–381.
