



A 69-year-old male patient on his thirteenth day of admission to the postsurgical critical care unit for bilateral SARS-CoV-2 pneumonia (26 days from onset of symptoms). His history was only significant for an episode of peritonitis 20 years prior. He was on lung protective mechanical ventilation and had received several cycles of ventilation in the prone position. His PaO2/FiO2 ratio suddenly fell from 140 to 80. A point-of-care pulmonary ultrasound was performed (Fig. 1 and Appendix B supplementary table). Pleural drainage was placed on suspicion of pneumothorax secondary to barotrauma. Atelectasis persisted for 24 h, with no improvement in oxygenation and general worsening even after placement of a second pleural drain. In view of the clinical picture, we decided to limit therapeutic effort, and the patient died on day 15 of admission.
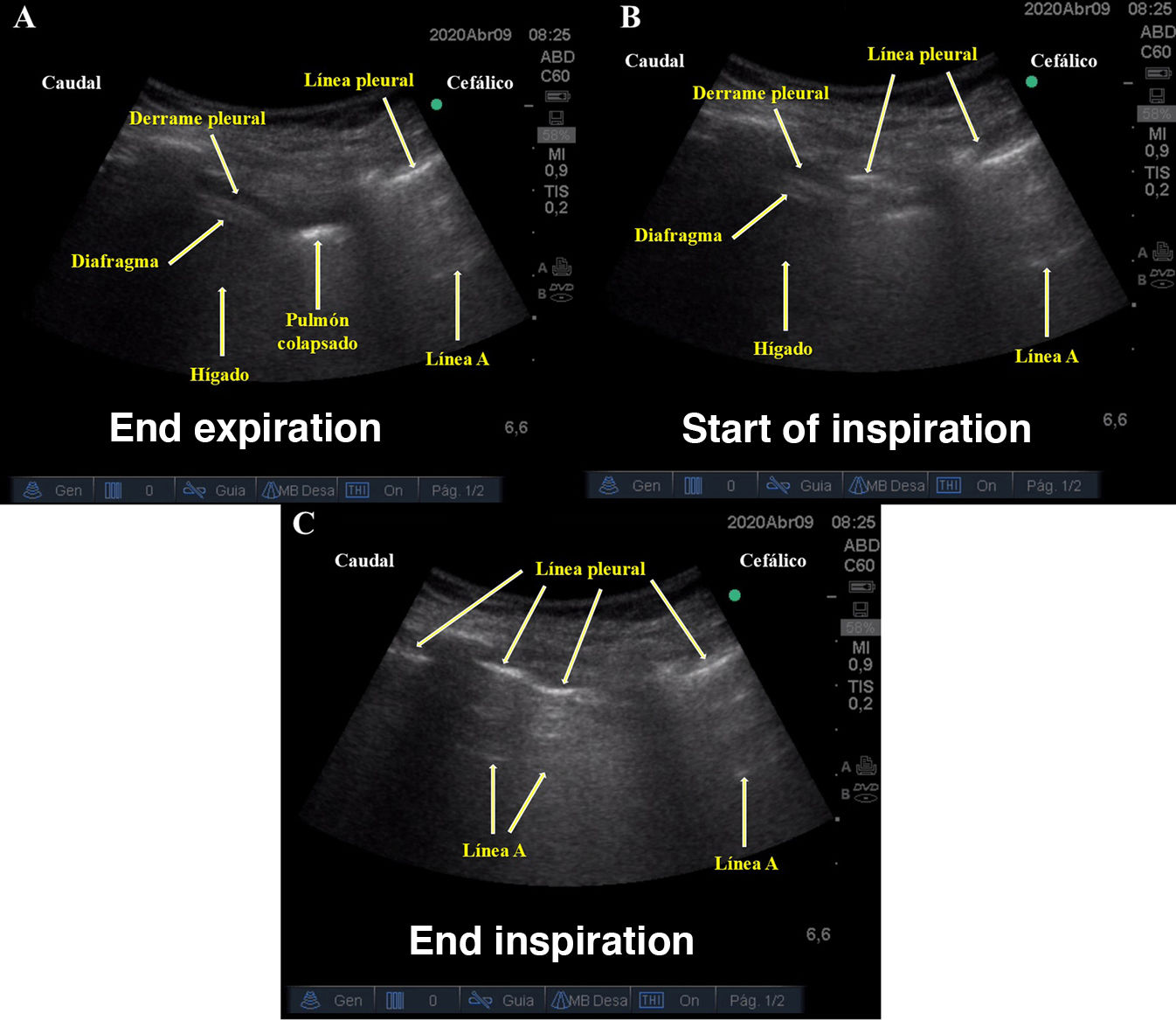
. A) End expiration: The diaphragm and liver are seen, together with an anechoic space between the diaphragm and chest wall (pleural effusion). Observe the “A” lines with no lung sliding in the uppermost intercostal space (pneumothorax). B) Start of inspiration: The “A” pattern starts to to shift downwards, erasing all subpleural ultrasound images. C) End inspiration: Only the pattern “A” is visible, with no lung sliding in the intercostal spaces. We interpret this sign as a barotrauma-induced air leak moving in sync with the respiratory cycle (Dynamic Hydro-point) (see Appendix B supplemental video).")
Variant of the hydro-point ultrasound sign during the respiratory cycle obtained using a convex transducer placed in the eighth and ninth right intercostal space on the mid-axillary line (sagittal plane). A) End expiration: The diaphragm and liver are seen, together with an anechoic space between the diaphragm and chest wall (pleural effusion). Observe the “A” lines with no lung sliding in the uppermost intercostal space (pneumothorax). B) Start of inspiration: The “A” pattern starts to to shift downwards, erasing all subpleural ultrasound images. C) End inspiration: Only the pattern “A” is visible, with no lung sliding in the intercostal spaces. We interpret this sign as a barotrauma-induced air leak moving in sync with the respiratory cycle (Dynamic Hydro-point) (see Appendix B supplemental video).
The authors declare that they have not received funding for this study.
Please cite this article as: Nieves Alonso JM, Méndez Hernández RM, Ramasco Rueda F, Planas Roca A. Punto hídrico (hydro-Point) en paciente COVID-19 ventilado con hidroneumotórax secundario a barotrauma. Rev Esp Anestesiol Reanim. 2021;68:553–554.
