




To know the result of the Girdlestone resection arthroplasty (ARG) in the treatment of the infected hip arthroplasty.
Secondary aimsTo analyze the effectiveness in the control of pain and infection, the functional outcome and to contrast factors correlated with the final result.
Patients and methodsCase series with a total of 17 patients. The control of the infection was assessed according to the presence or absence of sinus, and the clinical status using EuroQol 5D scale, residual pain and limb length discrepancy.
OutcomesThe most common infecting germ at the time of removal of the arthroplasty was Staphylococcus CN and one patient presented infection by Candida albicans. In 2 patients the draining sinus persisted. The residual dysmetria was 5.24cm. In the EQ-5D scale, the most affected dimensions were mobility, need for help for self-care and ability to carry out activities of daily life. 8 patients maintained, pain levels worse than 4 in the VAS. The variables of dysmetria were correlated inversely with health index (−0.54) and self-perceived general health status (−0.45).
ConclusionsThe Girdlestone resection arthroplasty is an alternative in the treatment of the infected hip arthroplasty. Patient perception is inversely corelated to residual dysmetria. The dysmetria is greater in women and in ages over 65 years.
Conocer el resultado de la artroplastia resección de Girdlestone (ARG) en el tratamiento de la artroplastia infectada de cadera.
Objetivos específicosAnalizar la efectividad en el control del dolor y la infección, los resultados funcionales y el contraste de factores que se correlacionen con el resultado final.
Pacientes y MétodosSerie de casos con un total de 17 pacientes. Se valoró el control de la infección según la presencia o no de sinus drenante, y su estado clínico mediante escala EuroQol 5D, el dolor residual y la discrepancia de longitud.
ResultadosEl germen infectante mas frecuente en el momento de la retirada de la artroplastia fue elStaphyloccocus CN y un paciente presentaba infección por Candida albicans. En 2 pacientes persistía sinus drenante. La dismetría residual era de 5.24cm. En la escala EQ-5D, las dimensiones mas afectadas fueron movilidad, necesidad de ayuda para autocuidado y capacidad para realizar actividades de la vida diaria. 8 pacientes mantenían niveles de dolor superiores a 4 en la EVA. Se encontraron correlacionadas inversamente las variables de dismetría con index de salud (-0.54) y estado general de salud autopercibido (-0.45).
ConclusionesLa artroplastia resección de Girdlestone es una alternativa en el tratamiento de la artroplastia infectada de cadera. La satisfacción del paciente está inversamente relacionada con la dismetría residual. La dismetría es mayor en mujeres y en edades superiores a 65 años.
Hip arthroplasty is recognised as one of the most cost-effective procedures in the therapeutic arsenal of orthopaedic surgeons. As treatment for degenerative pathology this procedure is able to substantially improve patient quality of life. As treatment for hip fracture it allows patients to return to basic everyday life activities early, thereby preventing life-threatening long periods in bed for the patient.
No surgical intervention is risk-free. Infection is one possible consequence. Implanting an inert material within an organism leads to the additional risk of infection, as it is unable to defend itself against the aggression of microorganisms, leading to a situation with devastating results.
Depending on the characteristics of an infection, diagnostic guides have been prepared together with others that recommend treatments that run from cleaning the focus of the infection while preserving the implant to removing the material if infection persists.1
Removing the components of a prosthesis as the final treatment option is included in the orthopaedic armoury to treat hip arthroplasty infection when the attempt to control an infection and re-implant the prosthesis has failed.2
The results reported in the past are affected by the shortening or persistence of an infection when cement residues remain in the bone implant site. Other factors which cause dissatisfaction are the use of aids for walking or restricted joint mobility.3 Although there is a significant reduction in the functional quality of walking for patients, cases in which walking styles have been recovered through corrective walking guidelines in young people have been recorded.4
The overall aim of this work is to show the result of Girdlestone resection arthroplasty (GRA) in the treatment of infected total hip arthroplasty in the Hospital Clínico Universitario Virgen de la Victoria, Malaga.
The specific objectives of this study are to analyse the efficacy of pain and infection control and the functional results obtained, as well as to verify the existence of factors which correlate with the final result.
Patients and methodsA descriptive study was undertaken of the cohort of patients operated in the Hospital Clínico Universitario Virgen de la Victoria, Malaga, who had received a GRA to treat an infected total hip arthroplasty in the period from 2005 to 2013.
A total of 17 patients treated by GRA were analysed. In the case of these patients the decision had been taken not to proceed with new surgical interventions due to their clinical state or incapacity to control the infection.
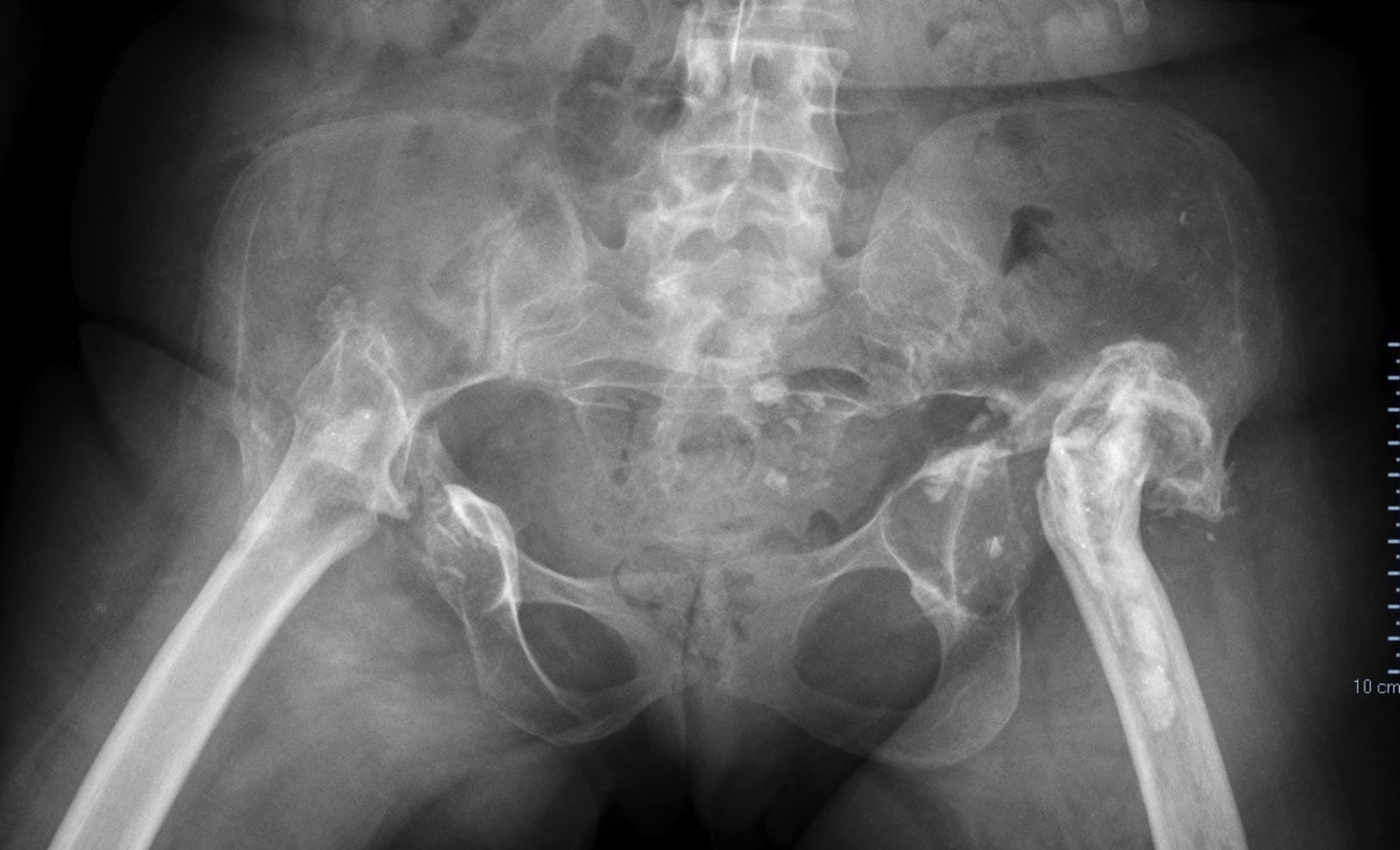
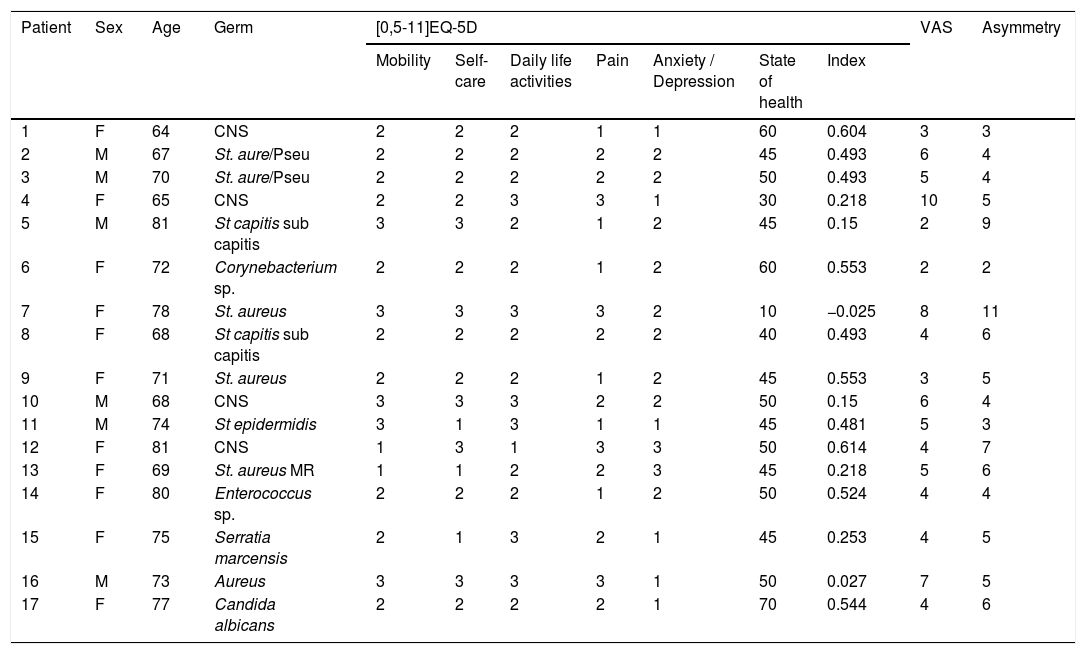
The group was composed of a total of 11 women and 6 men (Table 1). Their average age was 72.76 years (64–81 years) with an average follow-up time after GRA of 28.88 months, with a maximum of 72 months and a minimum of 6 months, respectively. One patient had been treated in both hips (#16−17) (Fig. 1).
Description of the patients and results.
| Patient | Sex | Age | Germ | [0,5-11]EQ-5D | VAS | Asymmetry | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mobility | Self-care | Daily life activities | Pain | Anxiety / Depression | State of health | Index | ||||||
| 1 | F | 64 | CNS | 2 | 2 | 2 | 1 | 1 | 60 | 0.604 | 3 | 3 |
| 2 | M | 67 | St. aure/Pseu | 2 | 2 | 2 | 2 | 2 | 45 | 0.493 | 6 | 4 |
| 3 | M | 70 | St. aure/Pseu | 2 | 2 | 2 | 2 | 2 | 50 | 0.493 | 5 | 4 |
| 4 | F | 65 | CNS | 2 | 2 | 3 | 3 | 1 | 30 | 0.218 | 10 | 5 |
| 5 | M | 81 | St capitis sub capitis | 3 | 3 | 2 | 1 | 2 | 45 | 0.15 | 2 | 9 |
| 6 | F | 72 | Corynebacterium sp. | 2 | 2 | 2 | 1 | 2 | 60 | 0.553 | 2 | 2 |
| 7 | F | 78 | St. aureus | 3 | 3 | 3 | 3 | 2 | 10 | −0.025 | 8 | 11 |
| 8 | F | 68 | St capitis sub capitis | 2 | 2 | 2 | 2 | 2 | 40 | 0.493 | 4 | 6 |
| 9 | F | 71 | St. aureus | 2 | 2 | 2 | 1 | 2 | 45 | 0.553 | 3 | 5 |
| 10 | M | 68 | CNS | 3 | 3 | 3 | 2 | 2 | 50 | 0.15 | 6 | 4 |
| 11 | M | 74 | St epidermidis | 3 | 1 | 3 | 1 | 1 | 45 | 0.481 | 5 | 3 |
| 12 | F | 81 | CNS | 1 | 3 | 1 | 3 | 3 | 50 | 0.614 | 4 | 7 |
| 13 | F | 69 | St. aureus MR | 1 | 1 | 2 | 2 | 3 | 45 | 0.218 | 5 | 6 |
| 14 | F | 80 | Enterococcus sp. | 2 | 2 | 2 | 1 | 2 | 50 | 0.524 | 4 | 4 |
| 15 | F | 75 | Serratia marcensis | 2 | 1 | 3 | 2 | 1 | 45 | 0.253 | 4 | 5 |
| 16 | M | 73 | Aureus | 3 | 3 | 3 | 3 | 1 | 50 | 0.027 | 7 | 5 |
| 17 | F | 77 | Candida albicans | 2 | 2 | 2 | 2 | 1 | 70 | 0.544 | 4 | 6 |
EQ-5: Euroqol-5D; CNS: coagulase-negative Staphylococcus; F: female; M: male; VAS: Visual Analogue Scale; SAMR: methicillin-resistant Staphylococcus; sp: species; St: Staphylococcus; sun: subspecies.

The following independent variables were examined: age, sex, number of previous procedures, the time elapsed after resection arthroplasty and the type of contaminating germ.
The following dependent variables were considered:
- -
Control of the infection. This took into account the normalisation of biochemical infection parameters (C reactive protein with a discrimination index of <3) and symptoms of the presence of a fistula.
- -
Pain evaluation. This was undertaken using the Visual Analogue Scale (VAS) to quantify the pain present at the time analysis took place.
- -
Quality of life. The EuroQOL-5D tool was used for this. This questionnaire was designed to evaluate quality of life in connection with health.5
- -
Patient assessment of the outcome. For this they were asked “how would you describe your condition after the operation in comparison with how you were beforehand?” Their answer was considered categorical as better, the same or worse than their last operation.
- -
Residual asymmetry. This was measured in cm and obtained by teleradiography once the result was considered to have consolidated, and their footwear was supplemented.
- -
Joint mobility. This was evaluated by examination of the degree of movement in passive flexoextension, ab/adduction and internal-external rotation.
- -
The use of walking aids.
A descriptive study was undertaken with the expression of absolute values and percentages for the categorical variables. Continuous variables are shown as medians with their limiting values and standard deviation.
Statistical correlation analysis between the variables of perceived state of health, EQ index and final condition evaluation by the patient was used to verify the results, in comparison with the independent variables of age, sex, asymmetry and control of the infection as defined by the presence or absence of a residual fistula. This correlation was understood to be very high when r stands at from 0.9 to 1.0; an r of from 0.7 to 0.9 was understood to be highly correlated; a moderate degree of correlation corresponds to an r level from 0.5 to 0.7; a low correlation corresponds to an r of from 0.3 to 0.5, and a lineal correlation was held to exist if this magnitude was lower than 0.3. Kendall’s τ test was used for this analysis, and statistical significance was set at P<.05.6
ResultsPrior to the GRA the patients had been subjected to an average of 3 (1–5) surgical procedures to try to control the infection. These exclude soft tissue interventions while retaining the arthroplasty. Only the interventions that involved replacing at least one of the components were counted, or failed replacement procedures in one or two stages.
At the moment of analysis all of the patients were living in their initial family environment, and none of them had been admitted to a home for the elderly.
The type of contaminating germ at the moment of performing the GRA was mainly coagulase negative Staphylococcus (CNS), 7 patients, while in 4 cases the infection was caused by Staphylococcus aureus (S. aureus), of which 2 were in association with Pseudomona aeruginosa. Two patients had an aetiology of Staphylococcus capitis and another had Corynebacterium sp. One case (#16−17) had infection by S. aureus in one hip and a fungal infection by Candida albicans (C. albicans) in the other.
Description of the resultsRadiological analysis. After the arthroplasty resection procedure, foreign material was present in 7 patients after the GRA. There were cement residues in 5 of them, and in 2 of them cerclages had been implanted to hold the fragments after the extended trochanteric osteotomy performed to extract the prosthetic material (Fig. 2).

The average residual asymmetry was 5.24cm (2–11).
The infection was considered to be uncontrolled in two patients with a persistent drainage fistula. The isolated germs in these patients varied, and at the time the implants were removed C. albicans was found, with one case of Corynebacterium sp. PCR remained high in both cases and the patients continued antibiotic treatment.
Respecting pain control, which was assessed using the VAS, a median score of 4 was found, with a value of 4 in the 1st quartile and 6 in the 3rd quartile.
The range of mobility evaluation found 68.48° (45°–90°) flexion; 0° extension; 35.91° (10°–60°) external rotation; 3.18° (0°–20°) internal rotation; 24.1° abduction (0°–45°); 13.64° (0°–45°) adduction.
Functional evaluation: EUROQOL-5D. Due to the small number of patients analysed, it was decided to reduce the 3 categories in each dimension into 2 categories; no problem or one problem/completely disabled.
- -
100% of the patients said that they had a problem with mobility, self-care or performing everyday activities.
- -
Respecting pain evaluation, only 6 patients considered that they were completely pain-free.
- -
Six of the patients considered that they had no problem in terms of anxiety -depression.
- -
The average score on the self-perceived health evaluation scale was 46.47 (10–70) (SD 15.39), with a median score of 45, a 1st quartile of 45 and a 3rd quartile of 50.
- -
The average score on the state of health index was 0.373 (0.614, 0.027). One negative observation was found (-0.025) (SD 0.20).
All of the patients required walking aids. Four of them used walking sticks and the other 13 used a walking frame. None of them was able to walk without assistance. Four patients in the latter group were exclusively active in the home.
Lastly, when asked whether they felt better, worse or the same as before the procedure, 4 of the patients felt worse, 5 felt the same and 8 felt better.
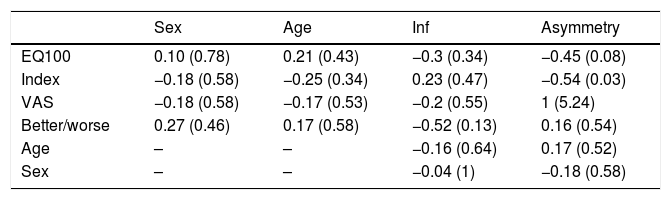
Statistical analysis to evaluate the relationship between variables found an inverse lineal correlation between the asymmetry variables and the corresponding EuroQoL-5D score, -0.54 (P=.03), as well as an association between asymmetry and self-perceived general health, −0.45 (P=.08) (Table 2).
Correlation between variables.
| Sex | Age | Inf | Asymmetry | |
|---|---|---|---|---|
| EQ100 | 0.10 (0.78) | 0.21 (0.43) | −0.3 (0.34) | −0.45 (0.08) |
| Index | −0.18 (0.58) | −0.25 (0.34) | 0.23 (0.47) | −0.54 (0.03) |
| VAS | −0.18 (0.58) | −0.17 (0.53) | −0.2 (0.55) | 1 (5.24) |
| Better/worse | 0.27 (0.46) | 0.17 (0.58) | −0.52 (0.13) | 0.16 (0.54) |
| Age | – | – | −0.16 (0.64) | 0.17 (0.52) |
| Sex | – | – | −0.04 (1) | −0.18 (0.58) |
EQ: Euroqol; Inf: infection; VAS: Visual Analogue Scale.
Although it was no statistically significant, a weak correlation was found between age and the self-perceived quality of life score (-043) so that the older patients were at the time of the operation, the more they were dissatisfied. The weak direct correlation between degree of asymmetry and patients considering themselves to be better or worse than before surgery was no statistically significant, either (0.61). To conclude, the greater the degree of asymmetry, the more patients were dissatisfied.
DiscussionGRA7 is a treatment option for infected THA in those cases when the infection cannot be controlled by treatments that aim to eradicate it and re-establish functional recovery by changing the prosthesis in one or two stages. It is indicated in patients with certain conditions of biological poverty, such as cerebrovascular accidents, dementia, infections caused by germs that are particularly hard to treat, patients with chronic infections and those with the risk of repeat infection, or when the conditions around the joint such as osteopenia, relapsing luxation, etc., make it impossible to predict satisfactory recovery of the patient.8,9
In spite of the final situation of the hip, as shown by X-ray imaging, results have been reported in which the infection was controlled in a high percentage of cases, with functional results that are considered to be acceptable.10,11
The circumstances which led to decision-making were agreed with the patient, given the impossibility of controlling the infection with the proposed solutions involving a change in one or two stages, and the loss of bone stock and weakening of the soft tissues. These considerations gave rise to the estimation that the functional result would not be better than would be obtained with the proposed procedure, while controlling the infection would be more difficult.
The patients had previously been subjected to 3 interventions, so that when deciding on treatment control of the infection to regain health was given priority over functional weakening. The possibility of repeating procedures that would challenge the skill of the surgeon as well as the biological resistance of the patient was therefore rejected, and this was also due to their defenceless condition due to the state of the soft tissues and the conditioning factor of the functionality and stability of the arthroplasty.
A widely proven and easily applied scale was used to evaluate the results: EuroQol-5D, complemented by a specific scale for the quantification of residual pain and evaluation of the contract between the previous and posterior state of the patient.
The purpose of this work was to discover the functional state of the patients subjected to GRA in our department, to assess whether good results were obtained so that it could be considered an alternative option in treating infection, or if it should only be considered as a last resort when treating THA infection.
The first study objective was to verify the degree to which infection was controlled in these patients, understood in terms of the absence of a drainage fistula. This was not always achieved in our patients. Of the 17 patients, 2 continued to drain purulent material from some point of the surgical wound. The local lesion, retention of necrotic bone residues unable to defend themselves against infection and the occasional presence of remains of the osteosynthesis material used to unite bone remnants and the osteotomy which was sometimes necessary to keep the shape of the bone and thereby permit a controlled support and restrict the movement of the stump against the base, mean that it was not always possible to control this factor. Osteosynthesis material and cement residues that were not removed during surgery remained in both patients. The contaminating germs found were C. albicans and Corynebacterium sp. When this occurred it was decided to continue with antibiotic treatment to thereby control the drainage. Our results in this respect are inferior to those reported by other authors, as they controlled the infection in all cases, although they do not refer to the type of contaminating germ.12
The second objective was to evaluate the level of well-being and pain control of these patients. Although this treatments is proposed in the literature as a means of ensuring pain relief, in our patients the improvement was partial. They maintained an average level of 4.82 on the VAS scale, leading to the need for continuing analgesic treatment. Although it was not statistically significant, higher levels of pain were found in the women, the younger patients and those in whom it had not been possible to control the infection. All of the patients needed some form of assistance for walking, unlike the report in some publications that 50% of the patients were able to walk without any assistance.13
The third objective was to analyse functional state in terms of the shortening of the limb and independence. After the operation these patients were allowed to sit up, move and commence walking early, without periods of bed rest or cutaneous traction. Even so, the limb was shortened to varying degrees. A direct correlation was found with patient age and sex, understanding the latter to lead to weaker soft tissues and therefore less capacity to control the displacements of the bone stump. Although this correlation was also found with age, this was at the limit of significance. When this relationship was checked as an independent variable for the final result in terms of pain, although a direct correlation was found this too was at the limit of significance. However, a strong correlation (0.61) was found when asymmetry was considered to be an explicative variable for patients considering themselves to be the same or worse. Lastly, asymmetry was found to be inversely related to the index and the EQ.
As is the case in other reports, GRA is a treatment option that acceptably controls infection and pain symptoms, at the cost of poor functional results.14
Study limitationsThis study is retrospective and it covers a small number of patients. It was not possible to overcome this limitation as the study was developed over 8 years and for the first cases no evidence was found that the test had been applied which considered the results from the point-of-view of the patient.
ConclusionsWe can summarise the results obtained by performing a GRA as:
Partial control of the infection.
Total pain control in these patients was not achieved.
The final result in terms of patient perception of whether or not they feel better after the intervention is directly associated with residual asymmetry.
Residual asymmetry is greater in women and patients above the age of 65 years.
Level of evidence III.
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: Zamora-Navas P, Estades-Rubio FJ. Calidad de vida tras artroplastia resección de Girdlestone. Rev Esp Cir Ortop Traumatol. 2021;65:24–30.
