




To expose our experience in the diagnostic and surgical treatment of neurogenic heterotopic ossification of the hip.
Material and methodsWe designed an observational retrospective descriptive study including 20 patients (30 hips) with neurogenic heterotopic ossification of the hip secondary to spinal cord injury attended in our institution in the last 10 years, with a minimum of one year follow-up. Medical files and imaging studies were reviewed. The study variables analyzed were: type and localization of neurogenic heterotopic ossification, pre–post excision range of motion, level and aetiology of spinal cord injury, ASIA score, smoking history, surgical approach and complications associated with surgery.
ResultsA total of 20 patients were treated with resection of heterotopic ossification in 30 hips. 16 patients presented ASIA A spinal cord injury and 4 ASIA B spinal cord injury. Preoperatively all the patients had severe ankylosis in the hip that made sitting in a wheel chair and activities such as repositioning and hygiene difficult. The average postoperative motion at the follow-up evaluation was 90° in flexion, 20° of internal rotation and 40° of external rotation. Immediately after surgery all the patients followed a specific intensive physiotherapy regime for the hip and celecoxib 200mg was administrated daily orally for a month to prevent recurrence of heterotopic bone formation. None of the patients reviewed suffered a recurrence of heterotopic bone formation.
ConclusionsSurgical excision of hip ossification in order to achieve functional ROM of the hip is the best treatment for patients with neurogenic heterotopic ossification of the hip.
Exponer nuestra experiencia en el diagnóstico y tratamiento quirúrgico de la anquilosis de cadera secundaria a osificación heterotópica periarticular.
Material y métodosEstudio descriptivo, longitudinal, de cohortes, retrospectivo, de 20 pacientes consecutivos (30 caderas) afectos de osificación heterotópica periarticular secundaria a lesión medular en los últimos 10 años, con un seguimiento mínimo de un año. Se realizó una revisión de las historias clínicas y pruebas de imagen, se valoró el tipo y localización de la osificación heterotópica periarticular, la movilidad pre- y postoperatoria, tipo, nivel y causa de la lesión medular según escala ASIA, tiempo desde la lesión medular hasta la cirugía, existencia de hábito tabáquico, abordaje quirúrgico utilizado y complicaciones asociadas a la cirugía.
ResultadosSe evaluaron un total de 20 pacientes (30 caderas): 16 pacientes presentaron un lesión medular completa ASIA A y 4, ASIA B. Todos los pacientes presentaban una anquilosis completa de la cadera que limitaba la sedestación en silla de ruedas, la higiene y los cambios posturales. La movilidad posquirúrgica media fue de 90° de flexión, 20° de rotación interna y 40° de rotación externa. En todos los pacientes se realizó fisioterapia intensiva en la articulación intervenida en el postoperatorio inmediato así como la administración de 200mg de celecoxib cada 24h durante un mes con el fin de prevenir la recidiva de la osificación. En ningún caso de la serie tuvimos recidivas de la osificación.
ConclusionesEl tratamiento quirúrgico mediante exéresis de la osificación hasta conseguir un rango de movilidad adecuado es el tratamiento de elección para los pacientes con anquilosis de cadera.
Periarticular heterotopic ossification (PHO) is a metaplastic formation of new bone in the connective tissue and muscular surrounding the joints affected by an injury of the central nervous system.1
It largely affects people with spinal cord injury, although it can also appear in patients with traumatic brain injury and in coma. Prevalence varies between 10% and 53%, depending on the different series.2
Despite exhibiting a high incidence in spinal cord injured individuals, its pathogenesis remains unknown.3
It can affect any joint, although the hip is the one most often involved, followed by the knee, shoulder, and elbow.4
In most cases, PHO manifests as a tumour affecting the joint and having little functional repercussions or impact on joint mobility in patients who use. As a result, it does not require surgical treatment and is merely supervised at the yearly check-ups in our hospital.
When joint ankylosis occurs that affects the hip, it is difficult for the sufferer to sit in their wheelchair, sacral pressure sores appear, as well as problems for intimate hygiene and transfers. In these cases, in which the spinal cord injured individuals’ quality of life is affected tremendously, the most effective treatment is the surgical excision of the periarticular ossification, thereby improving the patient's functionality and clinical symptomatology.5 It has typically been held that relapse of the ossification was the rule and, as a result, many orthopaedic surgeons have been reluctant to operate on these patients. In our series and with the regulated use of 200mg of celecoxib after the surgery, he have not seen a single case of relapse.
The aim of our study is to present the experience of a national reference hospital for patients with spinal cord injury in the surgical planning and management of these patients, as well as the complications of the surgery and how to attempt to avoid them.
Material and methodsDescriptive, longitudinal, retrospective, cohort study of 20 consecutive patients (30 hips) with PHO secondary to spinal cord injury and cared for at national reference hospital for spinal cord injuries in the last 10 years, with a mean follow up of 4 years and minimum of one year. The corresponding author was present at all the surgeries.
Clinical histories, surgical protocol, and imaging studies were all reviewed. The type and location of the PHO, pre- and postoperative mobility, type, level and cause of the spinal cord injury according to the ASIA scale, time between spinal cord injury and the surgery, whether the subject was a smoker or not, the surgical approach used, and complications associated with the surgical intervention were all assessed.
The patients were referred from the rehabilitation department or by orthopaedic surgeons from their reference hospitals due to limited mobility of one or both hips, the appearance of a painless tumour, and radiological findings compatible with PHO.
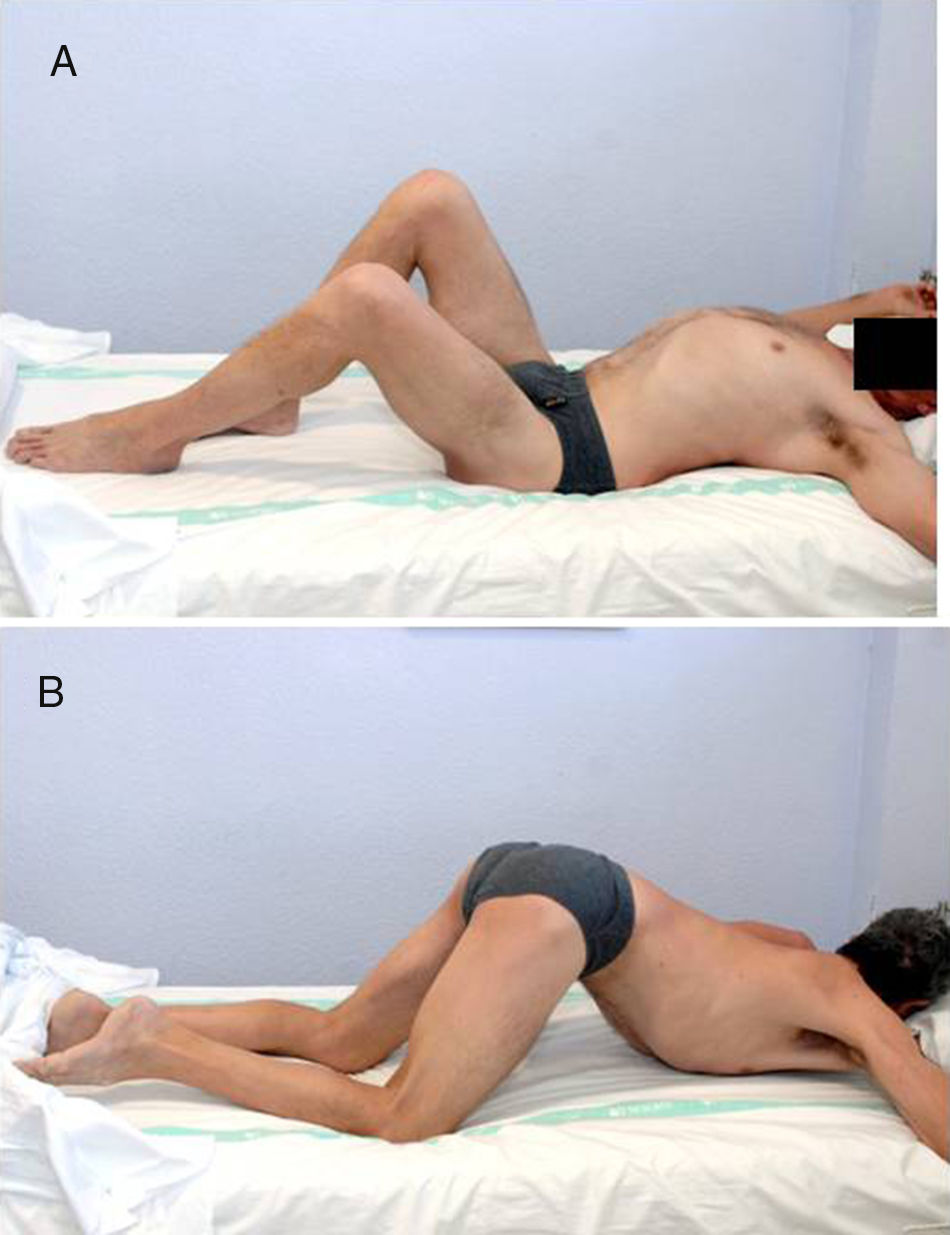
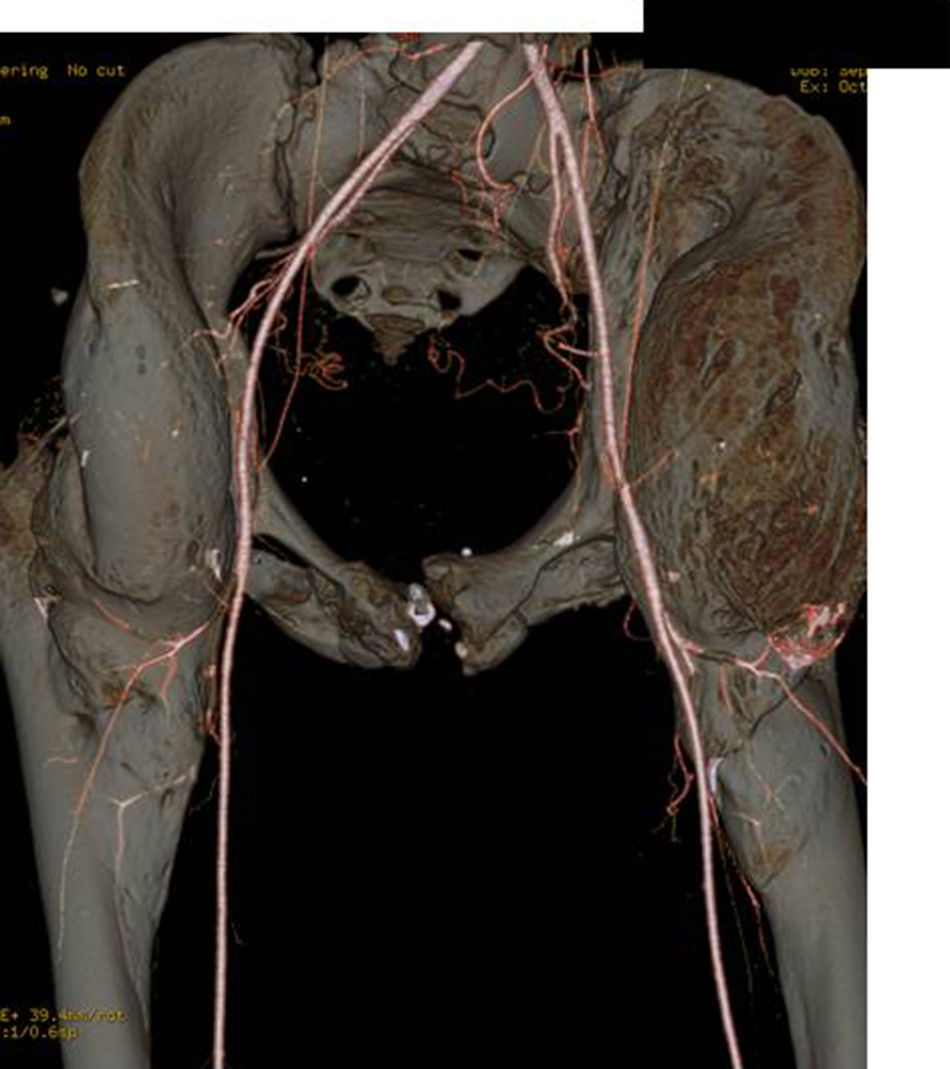
The ASIA classification was used to categorize the patients with spinal cord injury. The ASIA classification is a standard classification of spinal cord injuries published by the American Spinal Injury Association and sets forth the basic definitions of the terms used in assessing spinal cord injuries; likewise, it establishes a 5-level classification determined by the absence or preservation of motor and sensory function, indicative of the severity of the injury in question and its possible prognosis. It presents 5 scales, from A to E. A corresponds to a patient with a spinal cord injury in whom neither motor nor sensory function is preserved in segments S4–S5. Scales B–D are incomplete spinal cord injured patients and scale E indicates that both sensory and motor functions are normal. In total, 16 patients exhibited a complete spinal cord injury (ASIA A) and 4 displayed incomplete spinal cord injuries (ASIA B). All presented ankylosis of one or both hips that limited sitting in a wheelchair, personal hygiene, and was a risk factor for the appearance of pressure sores in the sacral area, given that the person was unable to change positions adequately (Fig. 1). They underwent evaluation that included physical examination, simple radiograph, magnetic resonance imaging, or CT (Fig. 2AFig. 2). In those patients in whom the PHO was suspected of encompassing the artery femoral, an angio-CT was performed for the purposes of surgical planning. The 3-D reconstruction of the PHO with the angio-CT allows for better surgical planning and choosing the most suitable approach in each case (Fig. 3).
 49-Year old patient with an ASIA B spinal cord injury following a traffic accident 8 years ago. Place in supine position, he presents ankylosis secondary to periarticular ossification (PHO) of both hips. The right hip displays greater involvement, with 85° flexion that limits his sitting in a wheelchair. (B) In the prone position, we can see ankylosis in both hips.")
(A) 49-Year old patient with an ASIA B spinal cord injury following a traffic accident 8 years ago. Place in supine position, he presents ankylosis secondary to periarticular ossification (PHO) of both hips. The right hip displays greater involvement, with 85° flexion that limits his sitting in a wheelchair. (B) In the prone position, we can see ankylosis in both hips.
 AP X-ray of the hips in which we can see PHO in the left hip that encompasses the entire joint in a patient with an ASIA A spinal cord injury that occurred 10 years ago. (B) P X-ray of the hips at 3 years following PHO resection.")

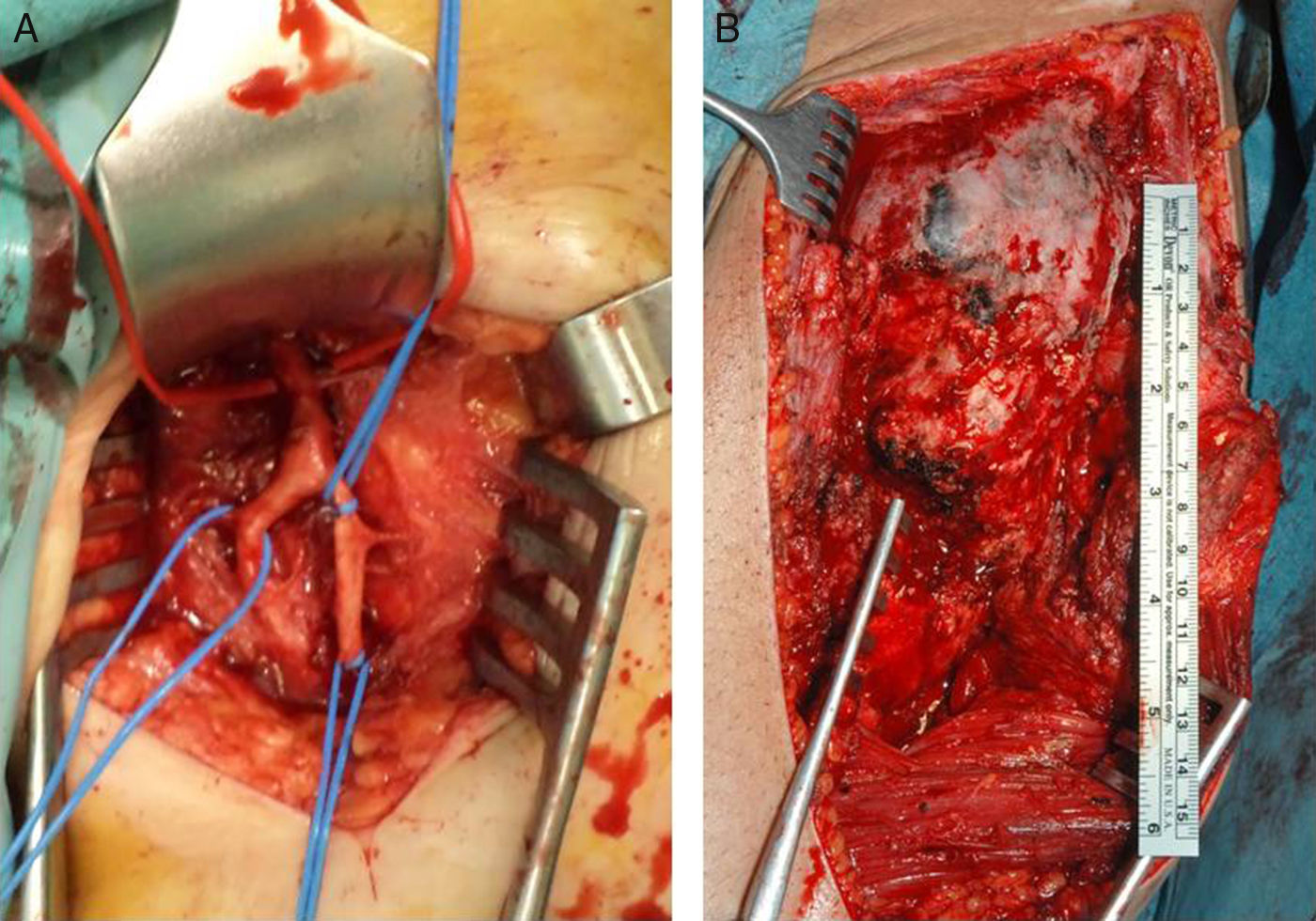
In most cases, the PHO is located on the anterior aspect of the hip, forming a bridge between the iliac wing and the anterior aspect of the femur that, generally, spares the coxofemoral joint, leaving it intact. There may be lateral, posterior, and medial expansion, which can displace or even encompass the femoral vascular bundle. This must be taken into account in case there is a need for the collaboration of vascular surgeons (Fig. 4).
 Superficial and deep femoral arteries in close contact with the PHO, located prior to resection of the PHO of the left hip. (B) Macroscopic images of the PHO of the left hip following the Smith-Petersen anterior approach.")
In all but 4 patients, a resection was performed as wide as possible of the PHO, sparing the joint. In 4 patients, who had previously undergone surgery at other centres with a partial resection of the PHO, a Girdlestone was performed.
Surgical techniqueThe patient is placed supine on a radiotransparent table, with a support underneath the gluteus that elevates the hip in question. The limb must be included within the field to allow mobility of the limb once the PHO is resected. In bilateral cases, we prefer to perform the surgery with one week intervening between each hip, given the abundant bleeding in the immediate postoperative period. In only one case with a small PHO, both hips were surgically treated on the same day.
In vast majority of the cases in which most of the PHO is located anteriorly, we use a Smith-Petersen type anterior approach to the hip. We reserve the lateral approach with the patient lying on their side for those cases in which the tumour expands more externally.
An incision is made from the antero-superior iliac spine and extended distally to the proximal third of the femur to the level of the lesser trochanter and proximally following the iliac wing to the site of ossification, taking care that the abdominal musculature is not detached. The ossification displaces the musculature of the thigh anteriorly; consequently there may be an interval between the sartorius and the anterior rectus through which to access the tumour, again, being careful to avoid injuring the femoral nerve. Once over the site of ossification, a blunt dissection is made using a periosetotome and the PHO is exposed as much as possible, especially at the medial level, where the vascular bundle is located (Fig. 4). If it has been encompassed, the common femoral artery and veins must be located and controlled, should there be an intraoperative injury. In long-term spinal cord injured patients, these vessels are very fragile, the tear easily, and their repair is complex. It is important to locate and ligate the medial circumflex femoral artery that enters the lesser trochanter and is generally hypertrophic, as it feeds the tumour. This will go a long way to decreasing bleeding when resecting the PHO. The tissue we are going to find tends to be stonelike and we can see interposed fibrotic areas. There may be significant bleeding from the perforating arteries that can be controlled with electrocautery or through the use of bone wax (Table 1).
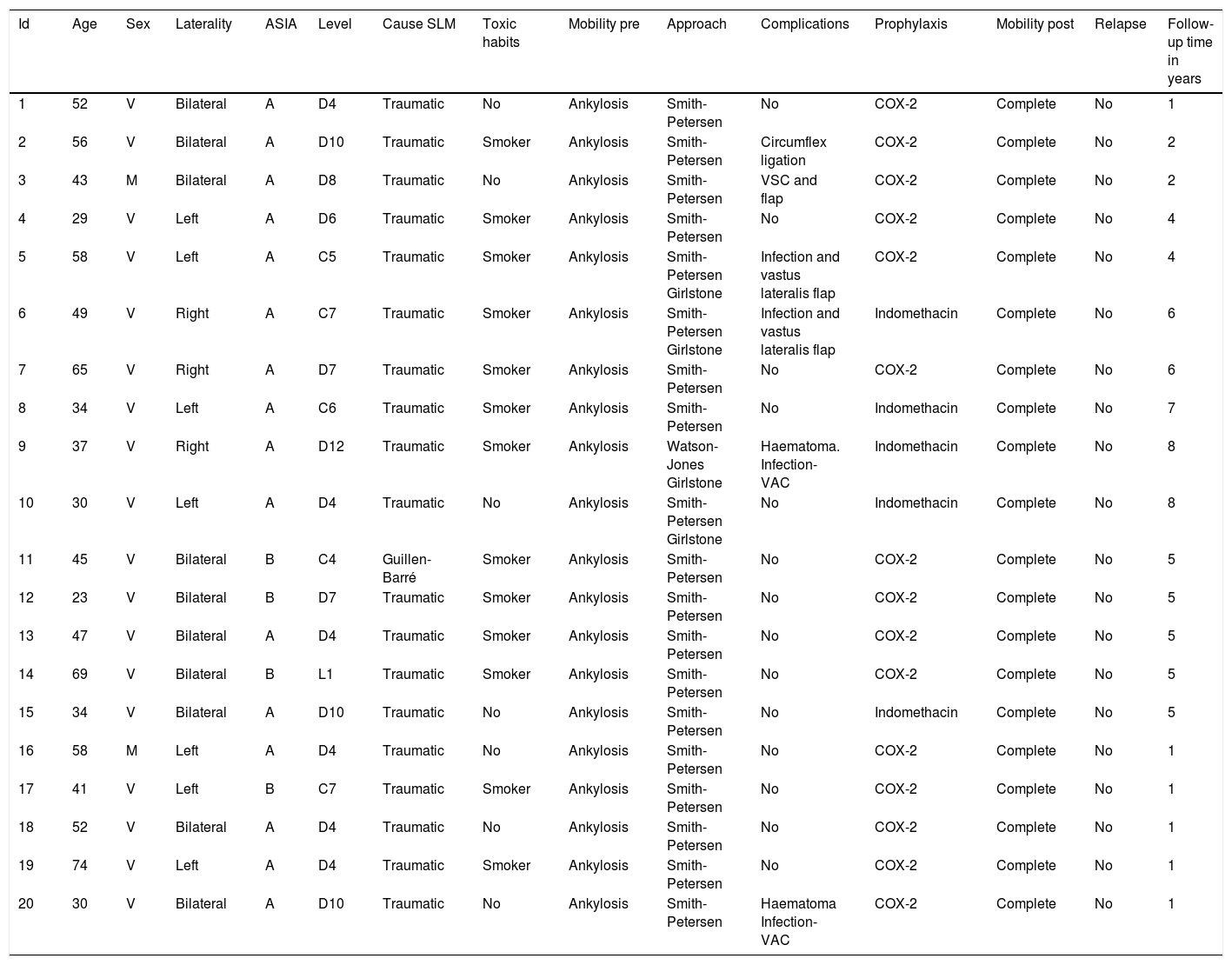
Series of cases of periarticular ossification of the hip included in the study.
| Id | Age | Sex | Laterality | ASIA | Level | Cause SLM | Toxic habits | Mobility pre | Approach | Complications | Prophylaxis | Mobility post | Relapse | Follow-up time in years |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 52 | V | Bilateral | A | D4 | Traumatic | No | Ankylosis | Smith-Petersen | No | COX-2 | Complete | No | 1 |
| 2 | 56 | V | Bilateral | A | D10 | Traumatic | Smoker | Ankylosis | Smith-Petersen | Circumflex ligation | COX-2 | Complete | No | 2 |
| 3 | 43 | M | Bilateral | A | D8 | Traumatic | No | Ankylosis | Smith-Petersen | VSC and flap | COX-2 | Complete | No | 2 |
| 4 | 29 | V | Left | A | D6 | Traumatic | Smoker | Ankylosis | Smith-Petersen | No | COX-2 | Complete | No | 4 |
| 5 | 58 | V | Left | A | C5 | Traumatic | Smoker | Ankylosis | Smith-Petersen Girlstone | Infection and vastus lateralis flap | COX-2 | Complete | No | 4 |
| 6 | 49 | V | Right | A | C7 | Traumatic | Smoker | Ankylosis | Smith-Petersen Girlstone | Infection and vastus lateralis flap | Indomethacin | Complete | No | 6 |
| 7 | 65 | V | Right | A | D7 | Traumatic | Smoker | Ankylosis | Smith-Petersen | No | COX-2 | Complete | No | 6 |
| 8 | 34 | V | Left | A | C6 | Traumatic | Smoker | Ankylosis | Smith-Petersen | No | Indomethacin | Complete | No | 7 |
| 9 | 37 | V | Right | A | D12 | Traumatic | Smoker | Ankylosis | Watson-Jones Girlstone | Haematoma. Infection-VAC | Indomethacin | Complete | No | 8 |
| 10 | 30 | V | Left | A | D4 | Traumatic | No | Ankylosis | Smith-Petersen Girlstone | No | Indomethacin | Complete | No | 8 |
| 11 | 45 | V | Bilateral | B | C4 | Guillen-Barré | Smoker | Ankylosis | Smith-Petersen | No | COX-2 | Complete | No | 5 |
| 12 | 23 | V | Bilateral | B | D7 | Traumatic | Smoker | Ankylosis | Smith-Petersen | No | COX-2 | Complete | No | 5 |
| 13 | 47 | V | Bilateral | A | D4 | Traumatic | Smoker | Ankylosis | Smith-Petersen | No | COX-2 | Complete | No | 5 |
| 14 | 69 | V | Bilateral | B | L1 | Traumatic | Smoker | Ankylosis | Smith-Petersen | No | COX-2 | Complete | No | 5 |
| 15 | 34 | V | Bilateral | A | D10 | Traumatic | No | Ankylosis | Smith-Petersen | No | Indomethacin | Complete | No | 5 |
| 16 | 58 | M | Left | A | D4 | Traumatic | No | Ankylosis | Smith-Petersen | No | COX-2 | Complete | No | 1 |
| 17 | 41 | V | Left | B | C7 | Traumatic | Smoker | Ankylosis | Smith-Petersen | No | COX-2 | Complete | No | 1 |
| 18 | 52 | V | Bilateral | A | D4 | Traumatic | No | Ankylosis | Smith-Petersen | No | COX-2 | Complete | No | 1 |
| 19 | 74 | V | Left | A | D4 | Traumatic | Smoker | Ankylosis | Smith-Petersen | No | COX-2 | Complete | No | 1 |
| 20 | 30 | V | Bilateral | A | D10 | Traumatic | No | Ankylosis | Smith-Petersen | Haematoma Infection-VAC | COX-2 | Complete | No | 1 |
In general, we will always find a free space between the PHO and the coxofemoral articular capsule. Before initiating resection of the PHO, this space must be located and a periosteotome, hook, or similar instrument should be inserted so as to prevent injury to the femoral head and neck.
The PHO need not be resected en bloc, but can be gradually excised using a chisel or saw until the anterior bridge is broken and an intraoperative range of motion of at least 90° of flexion and 20° of abduction is achieved, sparing the femoral head and neck (Fig. 2B). In PHO displaying medial extension, the tumour often comes up against the ischio-pubic branch and limits mobility. Resection of the PHO in this are must be performed very carefully, controlling the femoral vessels.
We use bone wax and Floseal® to control postoperative bleeding in a bloody cancellous bone bed.
The main postoperative problem is the formation of a haematoma in the cavity left by the PHO, with the corresponding risk of infection. Therefore, insofar as possible, the musculature must be spared and used to cover the defect adequately. To avoid this, two free flow surgical drains are left in place for the first 24h and later, continuous suction drains are left in place.
Antibiotic prophylaxis is usual in orthopaedic procedures with one preoperative dose that is maintained for 24h. Patients with spinal cord injury have a higher incidence of infection as they are generally colonized due to pressure sores and urinary catheterization.
Bleeding is abundant; thus, most patients will require blood transfusion, if not in the immediate postoperative period, certainly in the course of the first few postoperative day, as the drains contribute considerably to bleeding.
Rehabilitation begins 48h after surgery. It consists of passive mobilization with the aim of maintaining or increasing the range of motion achieved in the operating room.
In the first 4 patients of the series, 25mg of indomethacin per day were used as prophylaxis, which were later changed to 200mg of celecoxib: one tablet every 24h orally for one month, given that it displayed the same effect and was less aggressive for the stomach as preventive treatment for relapse of ossification.
On the other hand, information about satisfaction were collected by means of the hospital's own self-report questionnaire, which was given and filled in following completion of rehabilitation.
Statistical analysisThe statistical analysis was performed using the IBM SPSS Statistics 22 for healthcare sciences (SPSS Inc., Chicago, IL, USA). The results have been expressed as the mean±standard deviation. Descriptive statistics include frequency, mean, and standard deviation for quantitative variables such as age, duration of disease, and mean hospital stay.
ResultsThe series comprises 20 patients (18 males and 2 females), with a mean age of 46 years (range of 23–74 years). In 19 patients (95%), the spinal cord injury was caused by trauma and in one patient, it was due to medical cause (Guillen-Barré) (Table 1).
Eighty percent (80%) of the patients had complete spinal cord injuries (type A on the ASIA scale). The remaining 20%, were categorized as ASIA B. At the time of injury, 65% of the patients were smokers.
The mean time between the spinal cord injury and surgery for resection of PHO was 11 years.
In 10 cases (50%), both hips were involved; in 7 patients (35%), only the left hip was affected and in 3 patients (15%), only the right one. At diagnosis, 100% of the patients exhibited hip ankylosis that limited the sitting in a wheelchair.
The Smith-Petersen approach to excision of ossification of the hip was used in 95% of the cases and the remaining 5% were performed using a Watson-Jones lateral approach. In 16 patients (80%), the coxofemoral joint was able to be conserved in the PHO excision and in the 4 remaining cases (20%), a Girdlestone of the femoral head was necessary.
The mean recorded postoperative mobility was 90° flexion, 20° abduction, 20° internal rotation, and 40° external rotation.
Postoperative physical therapy was performed 48h after surgery in all cases; likewise, all cases received prophylaxis with 200mg celecoxib: one tablet every 24h orally for one month to prevent relapse of the ossification.
In 70% of the cases, no complications were recorded during the postoperative period. We had postoperative complications in 6 patients (30%). The complications recorded were: deep infection due to coagulase-negative germs (Staphylococcus epidermidis) in 3 cases, which required surgical cleaning, negative pressure VAC, and intravenous antibiotherapy adjusted to suit the antibiogram, and would closure using a flap harvested from the vastus lateralis (2 cases) and fascia lata (one case). In 2 cases, there was a collection of blood that required drainage secondary to superficial infection by S. aureus and S. epidermidis and specific antibiotherapy. One case of intraoperative injury of the deep femoral artery was recorded that called for repair and ligation of the colateral vessels. In this case, there was avascular necrosis of the femoral head, probably secondary to the ligation of the arteries that irrigate the femoral head.
All the patients, including the ones in whom there were complications, were satisfied with the result of the surgery; they would repeat the surgery, and expressed their satisfaction given the improvement it brought about in their quality of life and in their autonomy for their usual activities.
DiscussionPHO is a common complication in spinal cord injured individuals, although only few cases result in an ankylosis that requires surgical intervention.
The predisposing factors reported include complete spinal cord injury (ASIA A) and spinal cord injuries caused by trauma, spasticity, and urinary infection. The presence of pulmonary injury due to associated thoracic trauma, pneumonia, the presence of tracheotomy, and smoking at the time of injury have also been proposed as predisposing factors. As a result, a relationship between pulmonary involvement and the appearance of OPA has been postulated.6
The initial symptoms are non-specific and include erythema, sweating, pain, and early limitation of the mobility in the affected joint. Differential diagnosis in the early phase must include joint infection or deep vein thrombosis. The laboratory parameters, such as increased alkaline phosphatase are not specific. Increased urinary excretion of prostaglandin E2 in 24-h urine are included as early, specific indicators of ossification.7,8
In early diagnosis by imaging, ultrasound is the most efficacious test, as it can detect the earliest formation of bone tissue before radiographic findings, with a sensitivity of close to 89% in some series.9–11 Once PHO has formed, it can be evaluated by simple X-ray, CT, and MRI.
Radiographically, we used the Brooker classification for periarticular ossification of the hip. Nevertheless, its application in patients with spinal cord injury is limited, given that it is a classification that was designed for heterotopic ossification following implantation of a total hip prosthesis.12
The CT, and particularly the angio-CT with 3-D reconstruction, is highly efficacious for surgical planning, since it enables us to precisely assess the location and extension of the ossification,13 as well as verifying whether the femoral vessels are encompassed or displaced by the tumour. At present, we use it routinely in all patients who are to undergo surgery: the 3-D reconstructions are an important tool for proper presurgical planning, given the different possibilities to approach the hip depending on the site of ossification.14
The medical treatment for periarticular ossification consists of primary and secondary prevention. NSAIDs have been documented in preventing ossification periarticular. Several clinical trials have shown that the use of COX-2 NSAIDs and indomethacin lowered the incidence of PHO following spinal cord injury if administered within the first 3 weeks of the injury.15–17 The evidence indicates that NSAIDs are more effective in preventing PHO in spinal cord injured patients than bisphosphonates.18 Radiotherapy can be a useful tool in the prevention of OPA.19 Nonetheless, Teasell et al., in a systematic review of the literature conducted regarding therapies to prevent PHO in spinal cord injured patients, reflect that the existing evidence in the literature as to the use of radiotherapy in these patients to prevent progression of PHO is level 4 and more studies are needed to draw more conclusions.20
Our results are similar to those published in the literature and reflect that virtually all patients with PHO are patients with complete spinal cord injury (ASIA A).9,14
Of our patients, 13 were smokers when spinal cord injury occurred. These results are similar to those put for by Wittenberg,4 Citak6 and Coelho,17 in that they reveal smoking to be a predisposing factor for periarticular ossification.
Consistent with the bibliography, surgical treatment by means of resection of the PHO is the best treatment option in terms of autonomy for patients using a wheelchair. In our series, surgical excision is indicated when the patient presents articular ankylosis causing difficulty in sitting in the wheelchair, with the subsequent comorbidities, such as pressure sores in the ischiatic area. Like other and in light of the literature reviewed, the loss of mobility that precedes ankylosis is the prime factor when deciding on surgical intervention.21–24 The results obtained in our series as regards the range of motion obtained are similar to the results published by Meiners and Rubavi.5,25
In the present study, complications consisted of 3 deep infections due to coagulase-negative germs. In 2 cases, blood collected that required that a drain be placed and there was one case of intraoperative injury to the femoral artery that called for repair and ligation of the colateral vessels. In this case, there was avascular necrosis of the femoral head. These complications have been reflected in the literature; in our series the incidence is very similar to the mean, as reported by Yang et al.26
At 10 years of follow up, the incidence of relapse in our series is 0, which is significantly lower than the relapse published in the literature by Sautter and Moore.23 The regulated postoperative prophylaxis with 200mg of celecoxib for one month and immediate rehabilitation may be associated with the non-existence of relapse in our study.27 Like other authors,14 we do not use radiotherapies adjuvant treatment to avoid relapse, since: first of all, given the low evidence seen in the literature with respect to relapse with the use of this treatment modality; secondly, because of the zero presence of relapse with the use of 200mg of celecoxib, and thirdly, because, it is impossible to predict the possibility of a new formation of PHO or which joint it might affect. Therefore, given that radiotherapy is not an innocuous treatment, we choose not to use it.
The results obtained in this work indicate that surgical treatment by means of resection of the periarticular ossification and the use of COX-2 inhibitors for one month with early postoperative physical therapy offer outcomes that are satisfactory for the spinal cord injured person in a wheelchair.
As limitations of our study, it is worth noting that it is a retrospective study with a limited sample, given its low prevalence.
As strengths, our series is larger in size and has a longer mean follow-up period that most earlier publications; the data have been prospectively collected, with one of the authors present at all the surgeries and during patient follow up. The work has been conducted in a group of consecutive patients, in a highly homogenous clinical setting that is specialized in the integral treatment of spinal cord injuries, without the presence of selection bias.
As a conclusion, we believe that surgical resection of PHO, given the total absence of relapse of the ossification following excision surgery, is effective and enhances the quality of life in patients with spinal cord injury and who use a wheelchair. The degree of satisfaction is very high and all the patients would choose to undergo surgery again, despite the associated complications. In our hands and with the postoperative administration of Celecoxib 200mg for one month, we have not had a single case of relapse.
Level of evidenceLevel of evidence IV.
Ethical responsibilitiesProtection of people and animalsThe authors declare that no experiments on humans or animals were carried out for this study.
Data confidentialityThe authors state that they have followed their hospital's protocols regarding the protection of patients’ data.
Right to privacy and informed consentThe authors state that this article contains no patient data.
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: Romero-Muñoz LM, Barriga-Martín A, DeJuan-García J. Cirugía de la anquilosis de cadera por osificación heterotópica secundaria a lesión medular. Rev Esp Cir Ortop Traumatol. 2018;62:458–466.
