




The aim of our work is to check if the use of a pre-tensed bar connected to 2 supra-acetabular Schanz pins is more stable in a pelvic with a tile C1 injury.
Material and methodsWe used synthetic pelvis (N = 5) with a unstable vertical injury, stabilized with both the standard and the pre-tensed system. They both were submitted to axial loading. We measured applied forces and the position of markers that were positioned in the sacroiliac and symphysis joints. We determined the relative movements between injured surfaces, rigidity, resistance and when each system failed.
ResultsWhen using the pre-tensed fixator, the rigidity was much higher in the sacro-iliac joint(P=.043) being 3.45 times higher, being also 2.06 times higher in pubic symphysis (P=.043). The resistance against failure was 2 times higher too (P=.043).
DiscussionThe increased axial stability with the pre-tensed external fixator accords with its ability to make active compression in both posterior and anterior elements of the pelvic ring, which was previously demonstrated. This result supports the preliminary clinic outcomes that were obtained.
ConclusionsThe pre-tensed external fixator increases the axial stability of the pelvic ring's posterior elements in a synthethic pelvis with a Tile C1 injury, without decreasing it's capacity to achieve an anterior stability.
Comprobar si la aplicación de fijación externa mediante barra curva conectada a clavos de Schanz supraacetabulares confiere mayor estabilidad al anillo pélvico con una lesión tipo Tile C1 cuando se realiza el montaje con la barra pretensada que con el montaje estándar (sin pretensar).
Material y métodosPelvis sintéticas (n=5) con lesión verticalmente inestable estabilizada con ambos montajes se sometieron a carga axial progresiva. Se midieron las fuerzas aplicadas y las variaciones en las posiciones de marcadores situados en la articulación sacroilíaca y la sínfisis y se registraron con un sistema óptico. Se determinaron los desplazamientos relativos entre las superficies lesionadas, la rigidez, la resistencia y el modo de fallo de cada montaje.
ResultadosCon el fijador pretensado, la rigidez del montaje en la articulación sacroilíaca resultó muy superior a la del montaje convencional (p=0,043), multiplicándola por 3,45, siendo 2,06 veces mayor en la sínfisis. La resistencia ante el fallo también fue superior, multiplicándola por 2 (p=0,043).
DiscusiónEl aumento de estabilidad a carga axial con el fijador externo pretensado concuerda con su capacidad de producir compresión activa simultánea en los elementos posteriores y anteriores del anillo pélvico, demostrada previamente. Este resultado soporta los excelentes resultados clínicos preliminares obtenidos como tratamiento provisional.
ConclusionesEl fijador externo pretensado aumenta la estabilidad axial de los elementos óseos posteriores del anillo pélvico con lesión tipo Tile C1 en modelo sintético, sin disminuir la capacidad de estabilización anterior propia de la fijación externa anterior.
External fixation continues to be a fundamental tool in the treatment of fractures and dislocations of the pelvis,1,2 especially in the polytrauma patient and in the patient with haemodynamic instability, by closing the injured pelvic ring or controlling the expansion of intrapelvic haematoma. In addition, stabilisation of bone fragments also controls cancellous bone bleeding, allows pain control and mobilisation of the patient.3
The conventional external fixators most commonly used in the emergency department, or the internal subcutaneous bar fixators, are capable of stabilising and reducing the displacement of the anterior pelvic elements, with better performance in injuries with horizontal instability, such as in open book injuries (Tile type B1), as they allow closure of the pelvic ring. However, they fail to reduce or provide sufficient stability to the posterior pelvic elements.4–6
To improve posterior stability, the C-clamp was introduced, which exerts compression directly on the posterior elements, although its application is not without complications.7 In addition, it has the disadvantages of having a high volume and weight, which makes it difficult to handle the patient, limiting its use. Other anterior placement systems capable of producing simultaneous compression of the anterior and posterior elements have been described, such as the use of a femoral distractor as an anterior pelvic compressor,8 which has similar disadvantages to the C-clamp, or the use of an X-frame9 to apply a conventional fixator, which achieves notable compression, although the system is unable to retain it when the bulky frame is removed.
Increased compression of the pelvic ring has been associated with improved stability10,11 and closing the ring is more effective in expanding the intrapelvic haematoma. An alternative designed for this purpose is the pre-tensed external fixator,12 which is a novel modification of the standard assembly of a simple conventional fixator with a curved carbon fibre bar. This system exerts active compression on both the sacroiliac (SI) joint and the pubic symphysis.
This compression is achieved by first pre-tensioning the carbon fibre bar, which is then connected to 2 Schanz nails in the supraacetabular position, and once this connection is made, the tensioner is released, tending the bar by elastic deformation to recover its original position and, therefore, performing a compression of the system. The efficacy of the system was established in a previous biomechanical study in synthetic pelvises,12 where superior compression forces of the pre-tensioned fixator were measured with respect to the conventional assembly, in ratios of 21:1 in the symphysis and 14:1 in the sacroiliac joint, in a model of injury with vertical instability (Tile C type). Preliminary clinical results presented in a small series of 13 patients with unstable pelvic fractures are promising, with excellent or good radiological results in the 12 survivors13 and no significant complications of displacement or infection. It seems logical to think that the compression of the pelvic ring achieved by this type of solution may contribute to greater stability under axial loading, although this point has not yet been established.
The aim of this study is to analyse whether in a pelvic injury model with vertical instability, the compressive forces produced by the pre-tensed external fixator on the articular surfaces improve the axial load stability of the pelvic ring, and also to evaluate the resistance to failure of the system. The working hypothesis is that the application of the pre-tensed external fixator confers greater axial load stability to the pelvic ring with Tile C lesion than the conventional non-pre-tensed assembly.
Material and methodsTo test the working hypothesis, a comparative biomechanical study was designed on a test bench. Five intact synthetic pelvises (model 1301-1, Sawbones®, Vashon, WA, USA) made of polyurethane foams of different densities in their outer and inner layers, reproducing the cortical and cancellous components of the bony elements, were used. The use of synthetic models has been described in previous biomechanical studies of pelvic ring fractures,10,11,14 and is considered a valid substitute for comparative studies against cadaveric specimens as it allows control of the possible dispersion in the results due to factors such as geometric or bone density variations, and which, on the other hand, are also scarcely available.
Specimen preparationDisruption of the left sacro-iliac joint and symphysis was performed in all specimens in an analogous manner to reproduce a vertically unstable dislocation model, type C1 of Tile.4
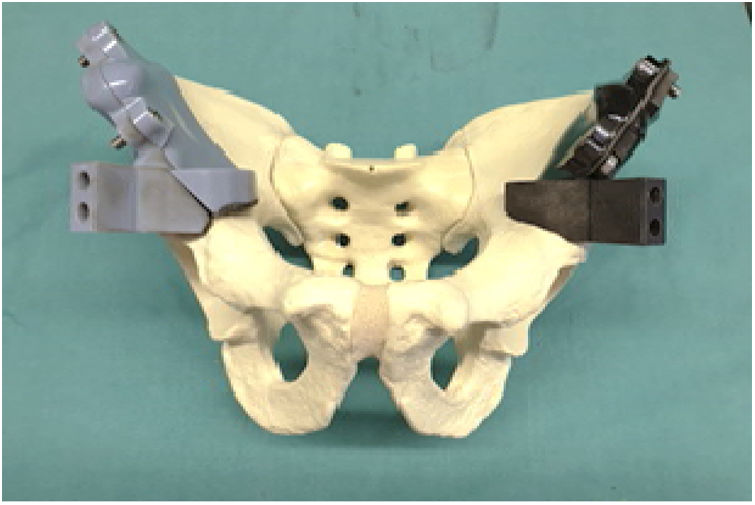
The connections to the pelvis of all external fixation systems compared in this study were made by means of two stainless steel Schanz pins (Ø 6mm×260mm, DePuy Synthes, J&J S.A, Madrid, Spain), each introduced a length of 120mm in supraacetabular position8 of the corresponding hemipelvis. For their placement, in order to minimise as much as possible the differences in their arrangement between specimens, insertion guides manufactured in plastic by 3D printing were used (Fig. 1), starting from a specific design based on the images obtained by CT of a radio-opaque pelvis model of identical geometry (model 1301-96, Sawbones®). Likewise, obtaining the geometry of the bearing surface of the guide on the iliac blade by Boolean subtraction of the geometry of the bone makes it possible to precisely adjust the guide in position and ensures the repeatability of the direction of insertion of the nails between specimens.
External fixation assemblies
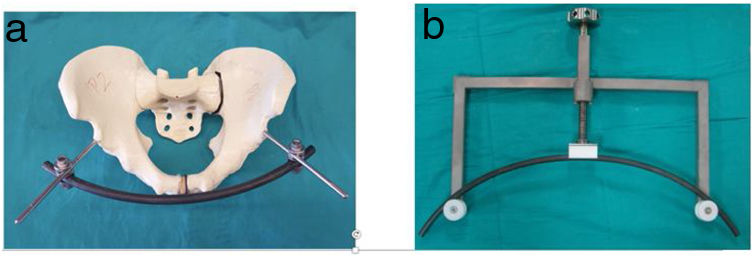
Once the Schanz pins were inserted, the specimen fractures were completely reduced and, manually exerting compression on the iliac blades to maintain the reduction, one of the 2 external fixators to be compared was connected to the pins (Fig. 2): (1) carbon fibre curved bar with conventional assembly according to the procedure described by Gänsslen et al.,11 and (2) pre-tensed carbon fibre curved bar.
 Curved bar with standard and pre-tensed assembly. (b) Curved bar tensioner used in assembly 2. The pretension level was that of a vertical displacement of 45mm from the top point of the bar to the centre line of the tensioner support sheaves, prior to connection to the Schanz nails.")
Study groups. (a) Curved bar with standard and pre-tensed assembly. (b) Curved bar tensioner used in assembly 2. The pretension level was that of a vertical displacement of 45mm from the top point of the bar to the centre line of the tensioner support sheaves, prior to connection to the Schanz nails.
The curved rods of the fixators were always connected in an inferior position with respect to the nails and using on each side a self-adjusting clip-on ball joint (SN 393.978, DePuy Synthes, J&J S.A, Madrid), whose axis was perpendicular and external to that of the nail and at a distance of 50mm from the bone.
In both set-ups (Fig. 2) the same model of curved carbon fibre rod (Ø 11mm×540mm, SN 394.79, DePuy Synthes, J&J S.A, Madrid) was used. However, in the second one, before connecting the bar to the pelvis, an elastic deformation of 45mm was applied (Fig. 2), using a tensioner previously designed for this purpose in the Clinical Biomechanics laboratory of the Mechanical Engineering area of the University of Malaga.11 The connection to the pins was made by keeping the bar pre-tensioned until the patellae were fixed and then releasing the deformation progressively so that the elastic recovery of the bar would produce compression of the pelvic ring.
All pelvises were tested with the 2 fixation systems, always applying the conventional assembly first to minimise the influence on the results of the study of possible looseness induced in the nail-bone interface of the model after the active compression that this system transmits to the pelvis through the Schanz nails. Once the test with the conventional assembly was completed, the bar was disassembled and the grip of the nails was inspected, checking that they had not yielded by manual traction, in order to verify their correct grip on the bone before proceeding with the second assembly. All nails were inserted by the same person.
Axial load testsFor the axial load test, the uniaxial testing machine developed at the Laboratorio de Biomecánica Clínica de Andalucía (Escuela de Ingenierías Industriales, UMA) was used. As in previous published studies,14–16 the reproduction of a loading scenario in monopodal support was selected because it induces a greater degree of pelvic instability than standing.15
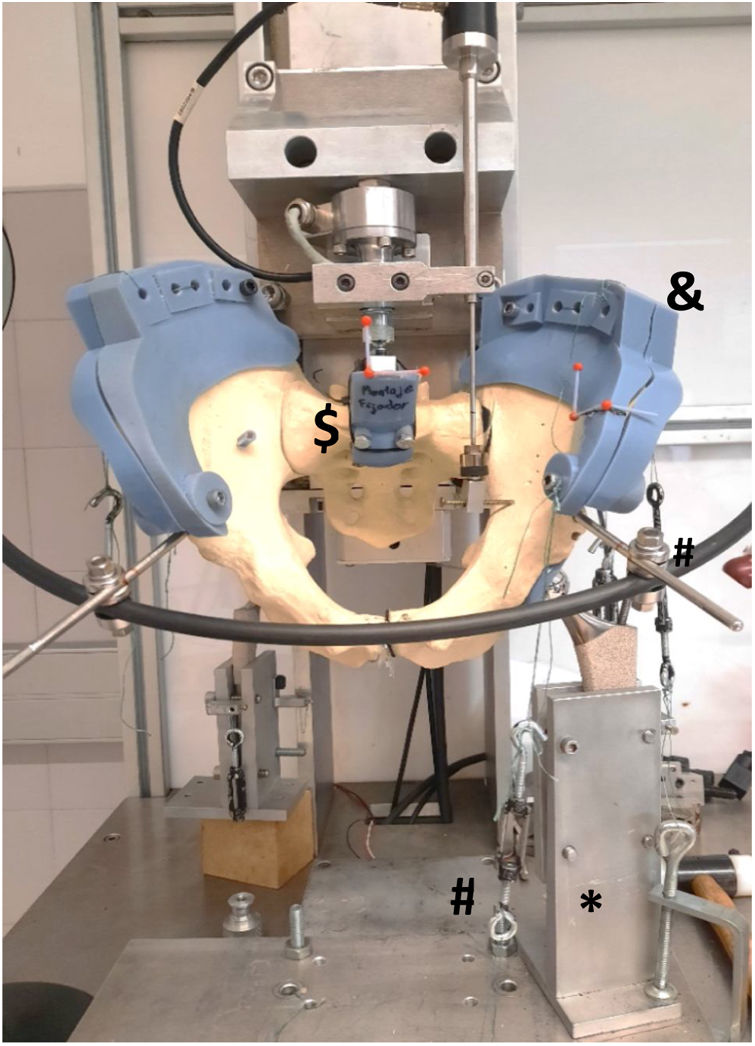
For this purpose, the specimen was supported on the spherical head (28mm diameter) of the titanium stem of a hip prosthesis (Accolade 2, Mahwah, New Jersey, USA) fixed to the base of the machine, 15 anteversion-oriented and 15 adduction-oriented. To simulate the ball-and-socket joint of a hip prosthesis, support at the acetabulum level was performed on a specially designed piece designed to fit closely in the left cup (side affected by the pelvic lesion), using the surface geometry of the acetabulum previously reconstructed in digital format from the CT images of the specimen.
Once the specimen was supported, it was oriented with the proximal surface of the sacrum forming 45° with the transverse plane to reproduce at the start of the test the anatomical positioning of the pelvis in an upright position. The vertical load was applied by interposing a wedge between the proximal surface of the sacrum and the horizontal loading surface (Fig. 3) which was attached to the head by means of a ball-and-socket joint to allow rotation in any axis, avoiding the transfer of moments to the pelvis. To control its rotation, the specimen was stabilised by replicating the action of the abductor muscles using a system of tensioners and ultra-high molecular weight polyethylene yarns (Avient, Dyneema®, USA) with a nominal load capacity of 255N. The threads were connected between points of the base and the blade separated by the fractures, in the direction representative of the action of each muscle group: sartorius and gluteus maximus and gluteus maximus and medius. To ensure reproducibility of the actions between specimens, the threads were connected using plastic parts with specific holes, designed and manufactured by 3D printing for a precise fit in the bone (Fig. 3).

After assembly on the testing machine, a loading protocol was applied consisting of an initial compressive load of 5N maintained for 10s, followed by increasing load at a constant spindle feed rate of .5mm/s. The applied loads were measured with the machine's built-in load cell with a maximum measuring range of 2kN and an accuracy of class 0.1 (model U2B, HBM, Darmstadt, Germany). The test ended when the head displacement reached 30mm.
The evolution of the displacements of the different bone segments with the applied load was quantified using a 3D optical measurement system synchronised with the load cell signal. The system is composed of 2 colour cameras (VCXU-124C, Baumer, Fillinges, France) that allow recording at 28fps and a resolution of 4096×3000 pixels, a control software and an image tracking programme, both developed in-house. The displacements were measured by tracking 4mm radius plastic spherical markers coated with ultraviolet (UV) paint. By synchronising the 2 cameras and after an appropriate calibration, it is possible to obtain the spatial trajectory (3D) of each marker by applying a triangulation algorithm to the images recorded simultaneously by both cameras at each instant.
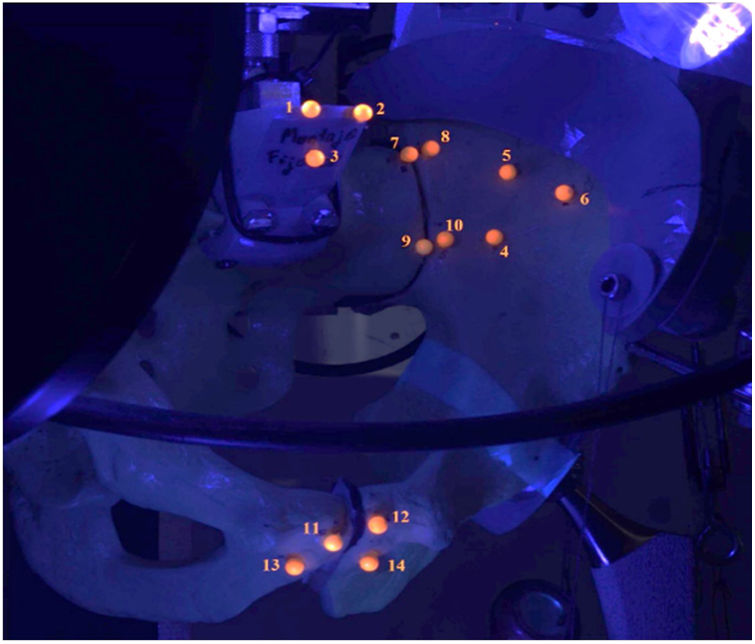
To measure the relative displacements between the bone elements on either side of the injured joints, pairs of spherical markers were used at the same top and bottom positions for all specimens. To minimise the influence on the comparison of the results obtained with the different fixators, their position was standardised by placing the markers of a pair on the same perpendicular to the fracture line, each one in a different bone segment and at a distance of 5mm from it (Fig. 4).

Markers fixed to each bone segment and prepared for monitoring. The illumination with ultraviolet light can be seen. Sacroiliac joint: 7–8=upper pair, 9–10=lower pair. Symphysis: 11–12=upper pair, 13–14=lower pair. Markers 1, 2, 3 and 4, 5, 6 define auxiliary coordinate systems fixed to the sacrum and the fractured blade, respectively.
Using the data collected during the test for each specimen-fixator combination, the relative displacements between the pairs of markers on each side of both joint lines were calculated to analyse the resulting stability of the pelvic ring. For each monitored position, load vs. relative displacement evolution curves were plotted. From these, fixation failure was determined as the first to occur of the following 2 events:
- -
A significant decrease in the slope of the load vs. relative displacement curve of some pair of markers.
- -
A relative displacement of 15mm between the 2 markers of one of the 4 pairs analysed.
From analysis of these curves the following were determined:
- -
The maximum force (Fmax) or force at failure achieved by each fixture.
- -
The secant stiffness at Fmax, calculated at each monitored position as the ratio between Fmax and the relative displacement measured at Fmax.
Given the non-linearity observed in the behaviour of the assembly, the force measured for relative displacements of 1, 2.5, 5, 7.5, 7.5, 10 and 15mm, in all pairs of markers, were also identified as characteristic parameters of the strength.
Statistical analysisTo analyse the differences found between the different test groups, the statistical analysis package IBM SPSS Statistics v.20 (International Business Machines Corporation, USA, 2011) was used. The significance level was set at p=.05. Differences in stiffness and strength between fastening systems were tested using a paired Wilcoxon signed ranks test, a non-parametric repeated measures test suitable for studies with small sample sizes.
ResultsEvolution of the vertical load with relative displacementsDue to the difficulty in detecting the centre of each marker during the fixation process and the irregularity of the bone surfaces, particularly in the lower symphysis, the resulting position of the markers varied slightly from that intended. The initial distance between the markers of each pair was determined by processing an image captured after preparation of the specimen, prior to mounting the fixators. The mean values (standard deviations) calculated for these distances were 10.63 (1.84) and 13.80 (3.01) for the upper and lower positions respectively at the symphysis and 10.87 (2.02) mm and 11.36 (2.64) mm at the sacroiliac joint.
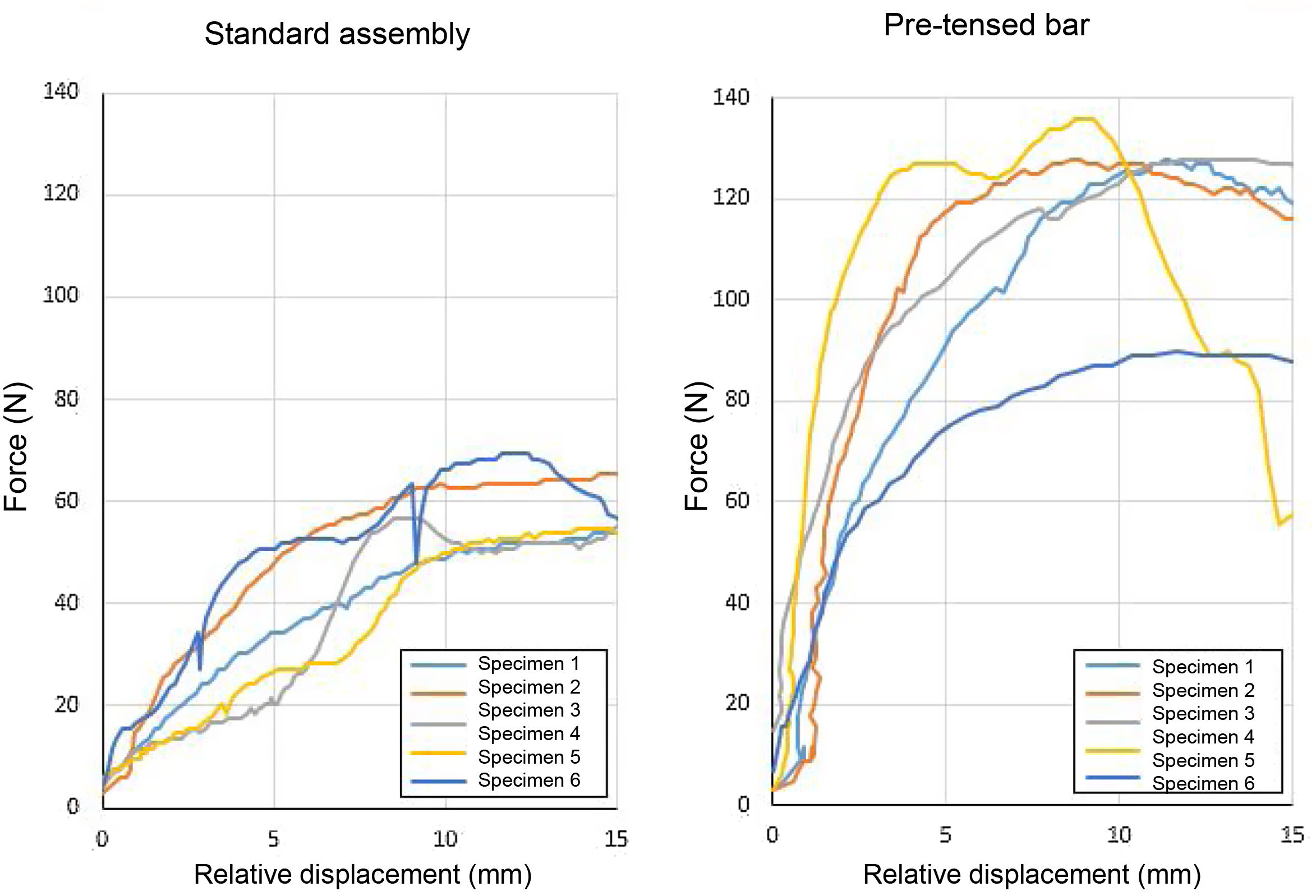
Qualitative observation of the vertical load vs. relative displacement evolution curves between the two pairs of markers monitored at each injured joint showed for all specimens a significantly greater initial slope in the pre-tensed assembly, indicating higher stiffness, and 2 times higher mean peak forces (Fig. 5). With both assemblies, failure was defined as a noticeable decrease in slope of the curves before the end of the test and at the same vertical load level for all monitored

Force evolution curves with relative displacement between the control points in the upper position on each side of the fracture of the sacro-iliac joint. The yellow curve corresponds to the specimen that, with the pre-tensed assembly, suffered a sudden dislocation after reaching peak force. This dislocation originated in the symphysis and led to a sharp drop in the force supported by the fixation.
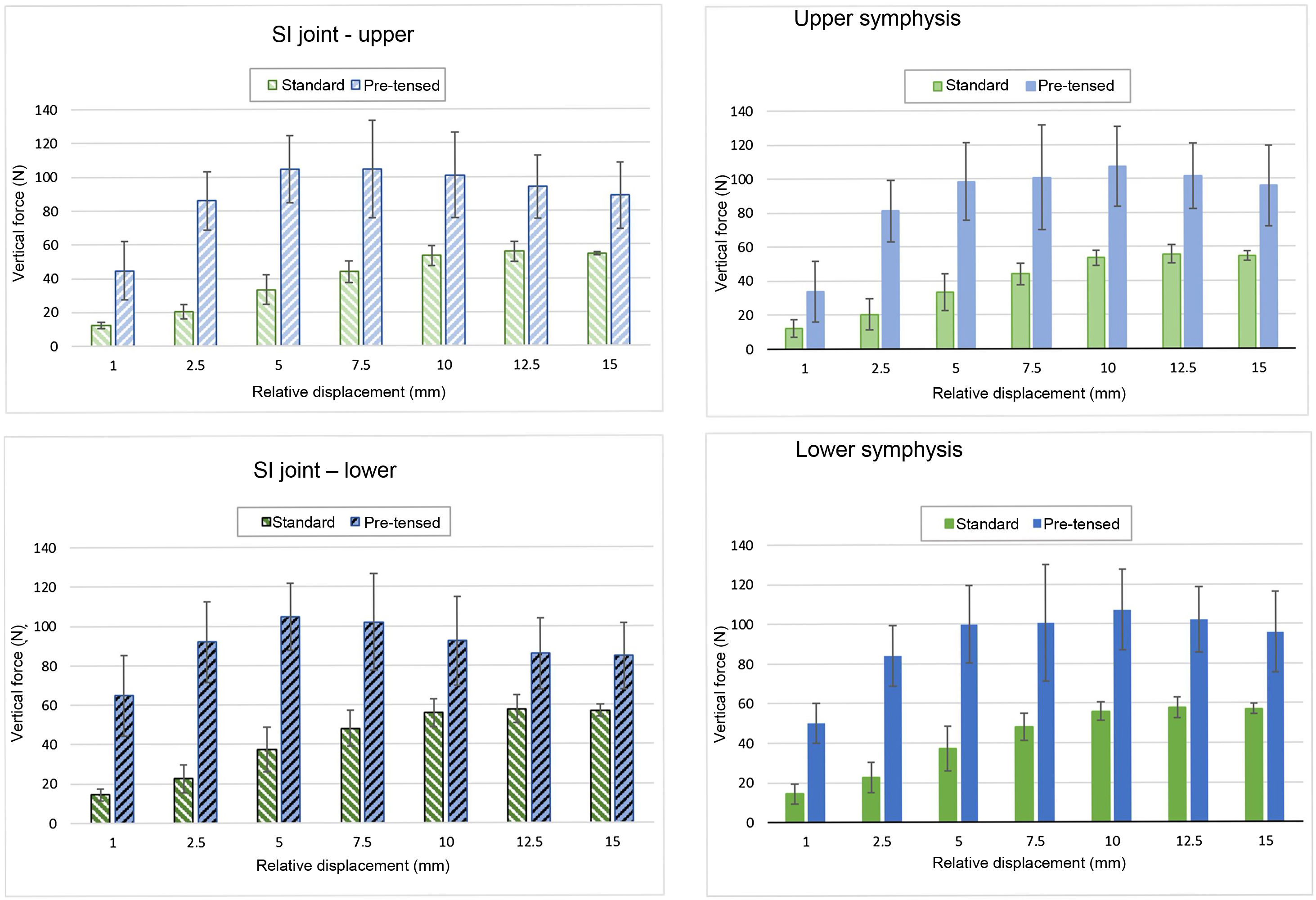
The evolution of the F values with respect to relative displacement between the articular surfaces shows similar patterns for the sacroiliac joint and the symphysis, but different for each curved bar assembly (Fig. 6). Interestingly, one of the specimens showed the highest stiffness and the event occurred after reaching the highest failure Fmax measured in all tests, corresponding to the yellow line in Fig. 5. With the standard mounting, the displacement resistance, i.e., stiffness, between the articular surfaces is very low initially, increasing progressively up to approximately 50N for 7.5mm, where the tendency towards stabilisation changes. In this way, loads above 55N can produce displacements of a value greater than 10mm, and even exceed the 15mm considered as the failure threshold in this study. On the other hand, with the pre-tensed curved bar, average loads of the order of the same 55N produce less than 1mm of average displacement. Moreover, from that initial millimetre, the mean stiffness increases rapidly until it reaches a local maximum around 10mm at the symphysis and 5mm at the SI joint, decreasing thereafter.

Comparing the axial load required to produce different levels of relative displacement (Fig. 6) showed that an average force of 2–5.8 times greater in the SI and 2.2–4.2 times greater in the symphysis was required to generate the same relative displacements, between 1 and 10mm, when using the pre-tensed bar than with the conventional assembly.
Fmax resisted by the systemPre-tensing the bar produces a significant increase in the failure resistance of the assembly (p=.043), with an average value of Fmax of approximately twice that obtained with the standard assembly (Table 1).
Fmax, displacement relative to Fmax and secant stiffness at Fmax for the analysed curved bar assemblies: conventional vs. pre-tensed.
| Assembly | Conventional | Pre-tensed | ||||||
|---|---|---|---|---|---|---|---|---|
| Fmax (N) | ||||||||
| Mean | 55.27 | 109.56a | ||||||
| SD | 4.48 | 20.31 | ||||||
| 95% CI | 51.95 | 58.59 | 94.52 | 124.61 | ||||
| Superior | Inferior | Superior | Inferior | |||||
| Mean | 9.28 | 9.12 | 5.28a | 4-69a | ||||
| SD | 2.07 | 2.02 | 1.42 | 1–68 | ||||
| 95% CI | 7.75 | 10.81 | 7–62 | 10.62 | 4–23 | 6.33 | 3–45 | 5–93 |
| K stiffness (N/mm) (Fmax/Displ. rel.) | ||||||||
| Mean | 6.33 | 6.42 | 21.85a | 25.7a | ||||
| SD | 1.69 | 1.64 | 6.17 | 8.21 | ||||
| 95% CI | 5.07 | 7.58 | 5.20 | 7.63 | 17.28 | 26.42 | 19.39 | 31.56 |
| SI-control point joint relative displacement for Fmax (mm) | ||||||||
| Superior | Inferior | Superior | Inferior | |||||
| Mean | 7.83 | 7.96 | 7.16 | 6.91 | ||||
| SD | 2.22 | 2.76 | 3.39 | 3.14 | ||||
| 95% CI | 6.19 | 9.47 | 5.92 | 10.01 | 4.65 | 9.68 | 5.67 | 8.16 |
| K stiffness (N/mm) (Fmax/Displ rel.) | ||||||||
| Mean | 7.81 | 8.29 | 16.12 | 19.32 | ||||
| SD | 2.70 | 4.10 | 8.08 | 8.39 | ||||
| 95% CI | 5.80 | 9.81 | 5.25 | 11.33 | 10.131 | 22.11 | 13.11 | 2.54 |
It should be mentioned that, in one of the specimens with pre-tensed fixator, excessive joint displacements produced by applying loads in excess of Fmax resulted in sudden dislocation of the bony elements at injury, due to the active compression exerted by the elastic recovery of the bar.
Stiffness at FmaxStiffness at Fmax was higher with the pre-tensed bar at the 2 dislocated joints (Table 1). With the 2 mounts, the mean stiffness was slightly lower at the upper point of both joints, with 2.06-fold increases at the symphysis and 3.45-fold increases at the SI joint with the pre-tensed bar compared to the standard mount, although the difference only reached statistical significance at the SI joint (p=.043).
When comparing the relative stiffness of the SI joint to the symphysis in the same set-up; in the conventional set-up the stiffness at Fmax in the symphysis was 1.23 times higher than in the SI joint. Whereas with the pre-tensioned external fixator the most stable joint was the SI joint, with an average stiffness 1.35 times greater than the pubic symphysis.
DiscussionThe main finding of this study is that the pre-tensed external fixator confers far superior vertical stability to that of the conventional mount on the posterior bony elements of a synthetic model of the pelvic ring with Tile C1 vertical instability.
The mean resistance to failure of the pre-tensed assembly was twice that of the conventional fixator and the minimum stiffness increased by a factor of 3.45 at the SI joint and 2.06 at the symphysis. Although the increase was only significant at the injured SI joint, the results corroborated that the pre-tensed fixator has the ability to increase posterior stability without decreasing the generally accepted anterior stabilisation ability of conventional mounting. This ability is attributable to the compression induced by the elastic recovery of the bar described in a previous study by Queipo de Llano et al.,12 in which in a similar synthetic model and with the bar connected at the same distance from the bone (50mm) and for the same level of pretension (45mm), compression forces of 71.1N at the SI joint and 48.3N at the symphysis were measured, higher than those of the conventional assembly in both joints (6.1N and 2.3N, respectively). Taking the average of the stiffness values calculated in the present study for the upper and lower control points, 23.67N/mm at the SI joint and 17.72N/mm at the symphysis, it is observed that there is a consonance between the higher stiffness obtained at the SI joint and the higher compression force previously measured at that joint, which points towards the existence of a relationship between both parameters.
In a biomechanical study similar to ours, performed with synthetic pelvises and type III AP pelvic injury, Vigdorchik et al.10 found no difference in axial load stability at the sacroiliac joint with the use of the INFIX system compared to a 3.5mm symphyseal plate and a conventional external fixator, although they did find that the plate was the stiffest assembly at the symphysis, followed by the INFIX system and the conventional external fixator. In another biomechanical study Vigdorchik et al.16 measured the
forces at the sacroiliac joint, as well as the stability of an anterior internal fixator (ASPIF) using an external device to compress the SI joint beforehand, compared to using a femoral distractor AO in compression8 and a conventional external fixator. Similar compression forces were measured at the SI joint (p<.001) in the anterior internal fixator (18.9N) and femoral distractor (18.6N) groups, but significantly lower with the external fixator (2.5N, p<.001). The pubic symphysis was less displaced with the femoral distractor than with the anterior internal fixator (5.5mm versus 4.1mm; p<.05). It should be clarified that the internal fixator (ASPIF) per se does not compress the SI joint, unless an external element is used to apply it, as was done in their study. However, it seems clear that compression at the SI joint causes additional stability to the axial load. This result coincides with ours in relation to the greater stiffness obtained with the pre-tensed fixator, a system capable of producing active compression in the posterior elements, compared to the conventional assembly. It is therefore logical to assume that by exerting a compression force 3.8 times greater, the pre-tensed external fixator will have a significantly higher posterior stabilisation potential than the subcutaneous bar.
Clinically, the pre-tensed fixator has the advantages of simplicity and speed of application over more complex compression systems, which makes it ideal for use in the emergency department due to its ability to maintain active compression of the sacroiliac joint and symphysis. The excellent preliminary clinical results obtained as a provisional treatment13 are supported by the stability demonstrated in this study which, if confirmed, would allow its use as a definitive treatment in certain clinical circumstances or when definitive internal fixation is not possible.
Although this study has performed the first axial load measurement of the pre-tensed external fixator, obtaining favourable results compared to the application of the conventional fixator, the work has certain limitations, such as the small sample size and the use of synthetic pelvises. However, as already mentioned, the use of synthetic pelvises is a widespread practice in comparative studies of pelvic ring stability14,16–18 that is able to control the dispersion in the results given by the use of cadaveric specimens. Furthermore, the use of synthetic pelvises of identical geometry has allowed us to develop 3D guides for the placement of Schanz nails with minimal variability, eliminating the influence of this factor on the results. Also, with this type of model it is not possible to faithfully reproduce the action of the soft tissues or musculature, although we tried to simulate the action of the main muscle groups acting in a monopodal loading scenario using a system of pulleys and cables. Finally, with the type of injury tested, it is advisable to apply anterior and posterior fixation systems simultaneously, so that, if the fixator is chosen as the definitive treatment, it may be advisable to add a posterior fixation element, which can be carried out at a later stage. The aim of the work was not to analyse the possibility of applying the pre-tensed fixator in isolation, but to analyse its individual contribution to the stabilisation of the assembly, testing it in the most unfavourable possible scenario in which there is no overlap with the contribution of other systems.
ConclusionsTo conclude, the outcomes of our study show that the pre-tensed external fixator increases the axial stability of the posterior bony elements of the pelvic ring with Tile C1 type lesion in a synthetic model, without diminishing the anterior stabilisation capacity of anterior external fixation.
Level of evidenceLevel of evidence i.
FundingOur research has been funded thanks to the grant awarded by the SECOT foundation. GRANT FOR INITIAL RESEARCH PROJECTS IN ORTHOPAEDIC SURGERY AND TRAUMATOLOGY, 2019. Awarded by the SECOT Foundation (Spanish Society of Orthopaedic Surgery and Traumatology) Spain.
Conflict of interestsFrancisco Javier Durán Garrido, Maximiano Lombardo Torre, Borja Delgado Rufino and Alejandro Peña Trabalón have no conflicts of interest to declare.
Alfonso Queipo de Llano and Ana Pérez de la Blanca are the inventors of patents ES 201230223 and ES 201230228 of the pre-tensed external fixator.
We would like to give special thanks to the SECOT Foundation, without whose help this research would not have been possible, as well as to the School of Engineering of the University of Malaga, whose collaboration has been essential in carrying out our research.
