



The Achilles tendon acts by transmitting the force created by the contraction of the sural triceps to the calcaneus. This allows the elevation during the gait cycle. A sudden contraction in elderly patients may generate avulsion fracture of the posterior tubercle of the calcaneus due to poor bone quality or rupture of the tendon, with one of these two structures yielding in most cases. We report the case of a 72-year-old woman who suffered a low energy right heel trauma while stepping off the bus. She was diagnosed an avulsion fracture of the posterior tubercle of the calcaneus. When performing ORIF procedure of the fracture, an associated rupture of the Achilles tendon is diagnosed. Both pathologies are treated in the same surgical act. We recommend using a second imaging study along with the x-ray in order to anticipate associated injuries and adequate surgical planning in elderly patients.
El tendón de Aquiles actúa transmitiendo la fuerza creada por la contracción del tríceps sural al calcáneo. Esto es fundamental para la elevación en el ciclo de la marcha. Una contracción brusca en pacientes mayores puede generar avulsión del tubérculo posterior del calcáneo debido a su mala calidad ósea o ruptura del tendón, cediendo en la mayoría de los casos una de estas dos estructuras. Presentamos una paciente de 72 años que al descender bruscamente de un transporte público presenta dolor en retropié. Se le diagnostica una fractura-avulsión del tubérculo posterior del calcáneo. Durante su cirugía de osteosíntesis se observa dicha fractura asociada a ruptura-arrancamiento del tendón de Aquiles. Se resuelven en un tiempo quirúrgico ambas patologías. Se recomienda en pacientes mayores asociar un segundo método diagnostico a la radiografía a fin de prever lesiones asociadas y poder realizar una resolución quirúrgica adecuada.
The Achilles tendon acts by transmitting the force created by the contraction of the sural triceps to the calcaneus. This is essential for elevation of the heel in the gait cycle. A sudden contraction in elderly patients may generate avulsion fracture of the osteopenic calcaneus or to Achilles tendon rupture.
Avulsion fractures of the posterior tubercle are rare, accounting for 1.3%–2.7% of all calcaneus fractures.1 The extremely infrequent combination of a fracture with an Achillles tendon rupture in the same episode has to our knowledge been previously reported in a single case in a patient with a history of Type 2 diabetes mellitus.2
The aim of this study was to present the case of an elderly patient with no remarkable history who suffered from concomitant avulsion fracture of the posterior calcaneal tubercle and rupture of the Achilles tendon, and the surgical treatment this entailed.
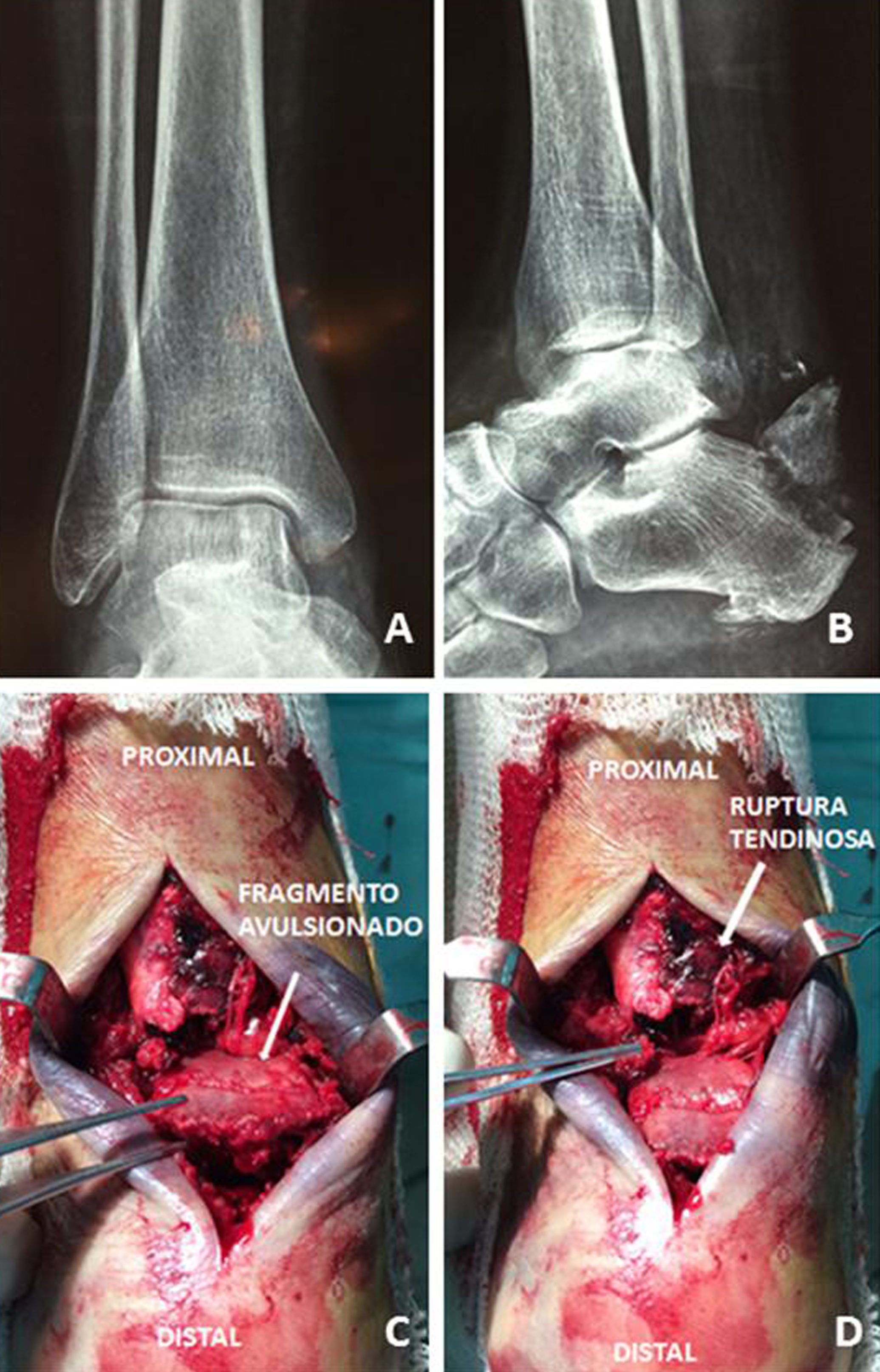
Clinical caseA 72-year old patient who was quickly stepping off a bus presented with pain in the right hindfoot. The mechanism of the injury involved forced dorsal flexion of the ankle. She presented at the Emergency Department in a wheelchair, stating she was unable to walk after the episode, with signs of pain and swelling in the right Achilles region and hindfoot. The patient referred to periodical clinical controls and did not suffer from any endocrine- metabolic or rheumatic comorbidities, nor was she taking any medication on a regular basis. Pulses and sensitivity were present on physical examination. The Thompson-Doherty manoeuvre proved positive. In x-rays of the ankle and foot in anterior posterior and lateral projections an avulsion fracture of the posterior calcaneal tubercle was observed (Fig. 1Fig. 1A-B).
ResultsInitial resolution. Fracture of the posterior calcaneal tubercle and proximal complete rupture of the Achilles tendon (C and D).")
The emergency service immobilized the foot with a long-leg plaster cast and referred the patient for therapy to achieve favourable evolution of soft tissues. No other diagnostic method was requested. Surgical treatment (open reduction and osteosyntheis with screws) was indicated for the fracture and the medical insurance company was requested to supply two cancellous bone screws of 4.5 mm with washers.
Surgical procedureThe patient underwent surgery eight days after the injury. Surgery was performed under spinal anaesthesia with the patient in a prone position, with no ischaemia cuff. A longitudinal approach was used on the medial edge of the Achilles tendon extending distally to expose the injury. After dissecting the soft tissues, the avulsion fracture of the posterior calcaneal tubercle was observed together with the complete rupture of the Achilles tendon proximally (Fig. 1 C–D).
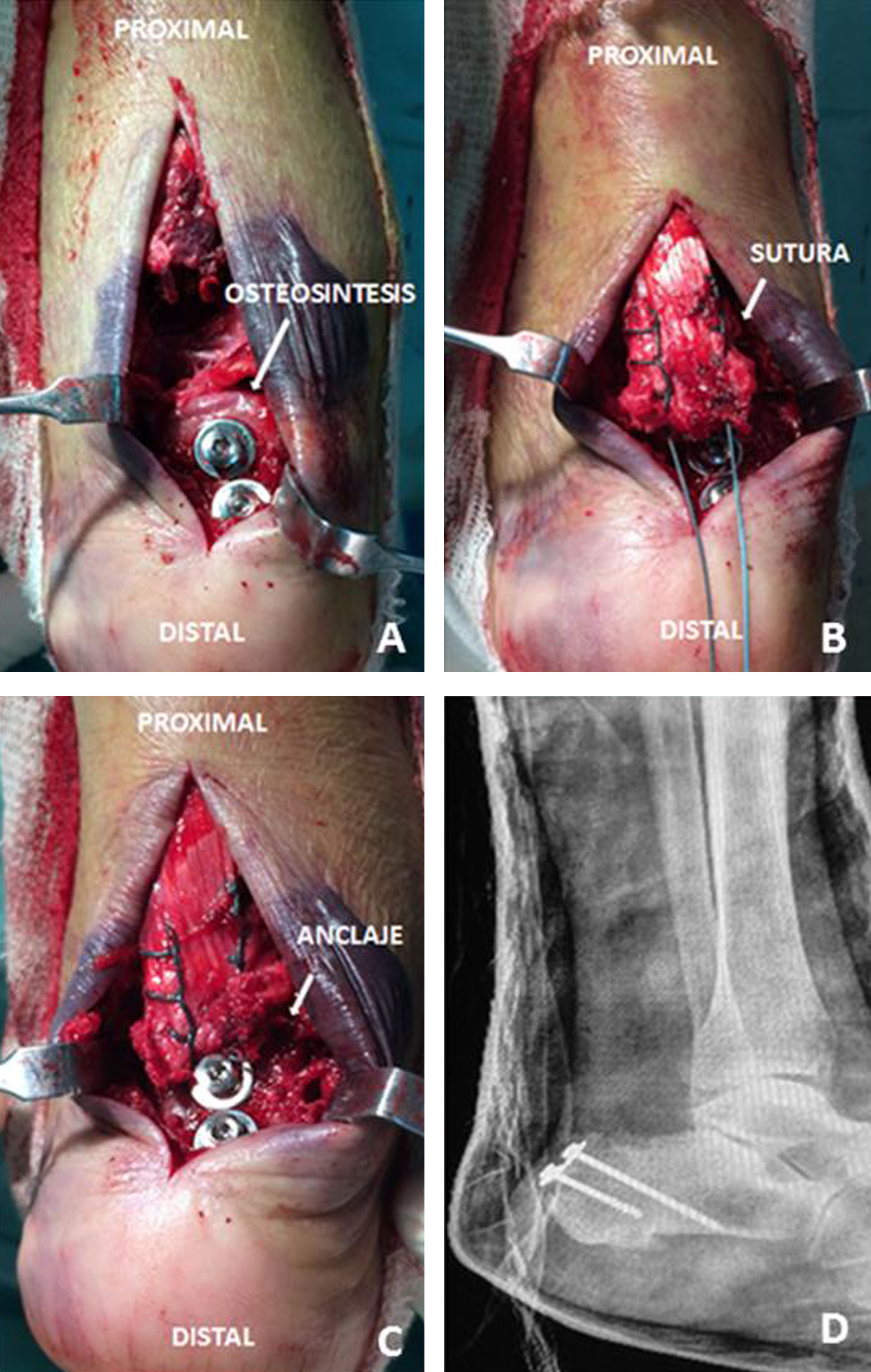
Osteosynthesis of the fragment with 4.5 mm non cannulated screws with washers (Villalba Hnos®, Fray Mamerto Esquiú 4548, B1678DAH Caseros, Buenos Aires, Argentina) was performed. The Achilles tendon injury was repaired with Krackow type suture with Ethibond Excel 2−0 (Ethicon®, 1003 U.S. 202, Raritan, NJ 08869, USA) fixed distally to the osteosynthesis material (Fig. 2). It was immobilized with long-leg plaster with the foot in equinus position.
Postoperative period distally anchored to the osteosynthesis materials (A, B, C and D).")
There were no complications of the surgical wound. Immobilization with plaster with foot in equinus position was maintained for four weeks and a Walker type boot was subsequently used. Controlled active and passive mobility exercises were indicated. The fracture consolidated and there was no need to extract the osteosynthesis material. Progressive partial support was authorised from 12 weeks onwards.
The patient recovered walking around near the house without limping, with a proven negative Thompson-Doherty manoeuvre, the ability to stand on tiptoes And a VAS scale score of 2 points, with mild or occasional pain. The AOFAS assessment system of the ankle and hindfoot was used, with a score of 74 points.
DiscussionAvulsion fractures of the posterior calcaneal tubercle are classified according to Beavis et al.3 into three types: in type I a proximal fragment of mainly cortical bone is avulsioned from the tubercle; type II is the classically described “beak” fracture and type III corresponds to a distal avulsion to the pre-Achilles bursa with minimum bone fragment. The case we presented corresponded to a type I lesion with a relatively large fragment, in which case interfragmentary4 screws for fixation are appropriate. Tension-band wires, re-attachment with hook wire and their combination are treatment alternatives for cases in which the bone fragment is not of sufficiently good stock for fixation with screws, or to increase their osteosynthesis.4,5
Achilles tendon rupture from low energy trauma in elderly patients is usually associated with pre-existing endocrine-metabolic comorbidities (mainly diabetes mellitus2,6 and kidney failure7), rheumatic8 and/or medical treatments (corticosteroids, fluoroquines).9 Treatment possibilities range from conservative management to enlargement tenoplasties, direct percutaneous or open surgical repair, with the indications for each of these procedures being prone to controversy.10
The combination of these two injuries was previously reported in a patient aged 58 with a history of diabetes mellitus.2 Our case in a patient without any known pathological history highlights the need to maintain a high level of vigilance of Achilles injury in avulsion fractures of the posterior calcaneal tubercle. Although the patient here presented with satisfactory outcomes, the characteristics of fixation were conditioned by the availability of the repair material, requested for dealing with the fracture. In environments where the operating theatre does not have a wide range of repair materials available (e.g. hook wire for tendon repair) but where the provision of material in keeping with the preoperative plan has to be requested in advance, we would suggest completing the diagnostic radiologic study with a scan of the Achilles region.
Level of evidenceLevel of evidence IV.
Ethical responsibilitiesProtection of people and animalsThe authors declare that the procedures followed complied with the ethical regulations of the committee responsible for human experimentation and the World Medical Association and Declaration of Helsinki.
Data confidentialityThe authors declare they have complied with the protocols of the place of work on the publication of patient data.
Right to privacy and informed consentThe authors obtained the informed consent of the patients and/or subjects referred to in the article. This document is held by the corresponding author.
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: Villalba JF, Desperes M, Lias A, Presentación de caso: fractura avulsión del tubérculo posterior de calcáneo con rotura de tendón de Aquiles en un tiempo. Rev Esp Cir Ortop Traumatol. 2020;64:434–438.
