



In uncemented revision total hip replacement due to polyethylene wear, the metal cup needs to be maintained when its stability is checked during surgery, only replacing the polyethylene that is cemented if anchoring is not possible. The aim of the present study was to evaluate the medium-term clinical and radiological results of a polyethylene liner cemented into an osseointegrated acetabular shell component.
Materials and methodsA retrospective analysis was performed on 15 patients in whom the surgical indication was polyethylene wear, with a mean follow-up of 6.1 years (range 3.5–9.7 years). The Harris Hip Score was used to assess the clinical results before surgery and at the end of follow-up. Anteroposterior and axial X-rays of the hip were taken to rule out complications.
ResultsThe mean Harris Hip Score improved, increasing from 64.7 points before the surgery to 80.3 at the end of follow-up. The osteolytic lesions disappeared, or at least the size did not increase, in the follow-up X-rays. One patient (6.7%) suffered 2 dislocation episodes that were treated without the need for surgery. Another patient presented with aseptic loosening of the femoral stem that required a replacement.
ConclusionsCementing the polyethylene liner, when anchoring is not possible, in an uncemented osseointegrated metal shell is a technique that offers good results in the medium term, and which may minimize the complications that may occur with the replacement of the shell component, without compromising its stability.
Ante una cirugía de revisión de artroplastia total de cadera no cementada por desgaste de polietileno está indicado mantener el cotilo metálico cuando se compruebe intraoperatoriamente su estabilidad, sustituyendo únicamente el polietileno que se cementa si el anclaje no es posible. El objetivo del presente estudio fue evaluar los resultados clínicos y radiográficos a medio plazo de la cementación de polietileno dentro de un componente acetabular metálico osteointegrado.
Material y métodoSe analizaron retrospectivamente 15 pacientes cuya indicación para la cirugía fue el desgaste de polietileno, con un periodo de seguimiento medio de 6,1 años (rango 3,5-9,7 años). El Harris Hip Score se utilizó para valorar los resultados clínicos antes de la intervención y al final del seguimiento. Se realizaron radiografías anteroposteriores y axiales de cadera para descartar complicaciones.
ResultadosLa puntuación media en el Harris Hip Score mejoró, pasando de los 64,7 puntos en el preoperatorio a los 80,3 al final del seguimiento. Las lesiones osteolíticas desaparecieron, o al menos no aumentaron de tamaño, en los controles radiográficos. Una paciente (6,7%) sufrió 2 episodios de luxación, que se trataron sin necesidad de cirugía. Otro paciente presentó aflojamiento aséptico del vástago femoral, que requirió el recambio.
ConclusionesLa cementación del polietileno, cuando no sea posible su anclaje, en un cotilo metálico no cementado osteointegrado es una técnica que ofrece buenos resultados a medio plazo, y que minimiza las complicaciones que conlleva el recambio del componente acetabular, sin comprometer su estabilidad.
Osteolysis attributable to polyethylene wear is one of the main indications for revision of uncemented total hip arthroplasty.1 Faced with worn out polyethylene liners, surgeons will only replace them when this is possible, otherwise they will also replace the acetabular cup. The replacement of an osseointegrated uncemented metal cup entails a longer surgical time, increased risk of bleeding and a considerable loss of periacetabular bone mass.2 Therefore, extraction of the acetabular cup is only recommended when the anchoring mechanism of the polyethylene implant is damaged, if the femoral head has eroded the metal cup or if the component is in the wrong position and may compromise stability.3
However, sometimes isolated replacement of the polyethylene may not be possible because a replacement is not available or is no longer produced. In such cases, cementing the polyethylene on an osseointegrated metal-back provides a valid alternative which maintains the bone reserve and decreases morbidity.4
The objective of the present study is to conduct a retrospective analysis of the clinical and radiographic medium-term results of revisions of total hip arthroplasty caused by polyethylene wear, in which the new insert was cemented because it was a non-modular prosthesis that was no longer manufactured.
Materials and methodsWe retrospectively analyzed 15 patients who underwent revision surgery of an uncemented total hip arthroplasty between December 2003 and June 2008.
The sample was comprised by 7 males and 8 females, with a mean age at the time of the primary hip replacement of 55.7 years. The diagnoses were coxarthrosis in 10 cases, avascular necrosis of the femoral head in 3 cases, and hip dysplasia in 2 cases. The mean survival of the primary implant was 14.8 years (range: 10 to 19.4 years).
The prosthesis used for the primary surgery was a Poropalcar® (IQL, grupo Biomet, Spain), composed by a femoral stem made of titanium–aluminum 4 vanadium and a “poropros” coating, with a semispherical acetabular implant of the same material and 3 flanges which favored its immediate stabilization. The polyethylene was an Arcom® model with ultrahigh molecular weight sterilized with gamma radiation in vacuum. The diameter of the femoral head was of 32mm.
The mean age at the time of the revision was of 69.9 years. The indication for surgery was due to polyethylene wear in all cases. Isolated replacement of the insert was not possible because it was no longer manufactured, so it was decided to cement a new one over the osseointegrated uncemented acetabular cup.
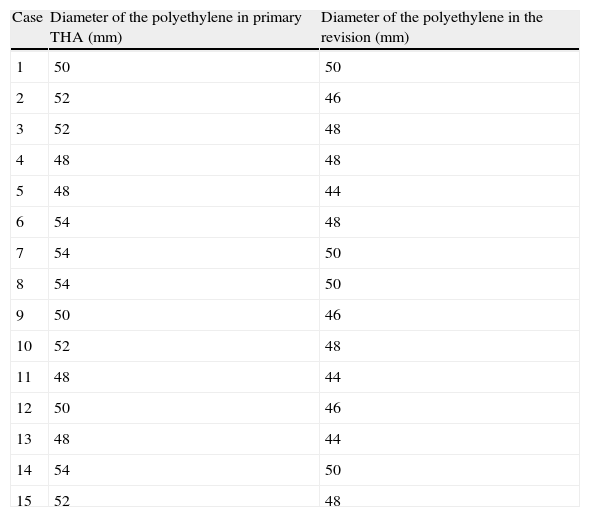
The revision procedure was performed following the same approach route as in the primary intervention; the anterolateral hip approach. First, the acetabular component was visualized and the primary polyethylene was removed, carrying out debridement of the periacetabular fibrosis at the same until the edges of the metal ring could be observed. Next, the osseointegration of the metal-back was verified by mechanical traction, and was deemed satisfactory in all cases. Next, a Müller® type cemented cup, with a size ranging from 44 to 54mm (Table 1) was implanted, applying homogeneous pressure. In most cases, this was undersized by 4mm with respect to the primary cup. In 2 patients the polyethylenes were of the same size as the acetabular cup, as they presented usury of the metal cup which ensured sufficient cement coverage, and circumferential grooves were added to favor union in the cement-polyethylene interface. This was an ultrahigh molecular weight polyethylene, with a semispherical and striated design in the area of fixation, so as to achieve a better integration with the layer of cement. The femoral head was replaced by another with a diameter of 28mm which was adapted to the 14/16 cone. Lastly, the periacetabular osteolytic defects detected in the preoperative radiographic study were examined, although they did not condition the stability of the implant in any case, and were filled with an allograft.
Size of the polyethylene used in the primary surgery and in the revision.
| Case | Diameter of the polyethylene in primary THA (mm) | Diameter of the polyethylene in the revision (mm) |
| 1 | 50 | 50 |
| 2 | 52 | 46 |
| 3 | 52 | 48 |
| 4 | 48 | 48 |
| 5 | 48 | 44 |
| 6 | 54 | 48 |
| 7 | 54 | 50 |
| 8 | 54 | 50 |
| 9 | 50 | 46 |
| 10 | 52 | 48 |
| 11 | 48 | 44 |
| 12 | 50 | 46 |
| 13 | 48 | 44 |
| 14 | 54 | 50 |
| 15 | 52 | 48 |
THA: total hip arthroplasty.
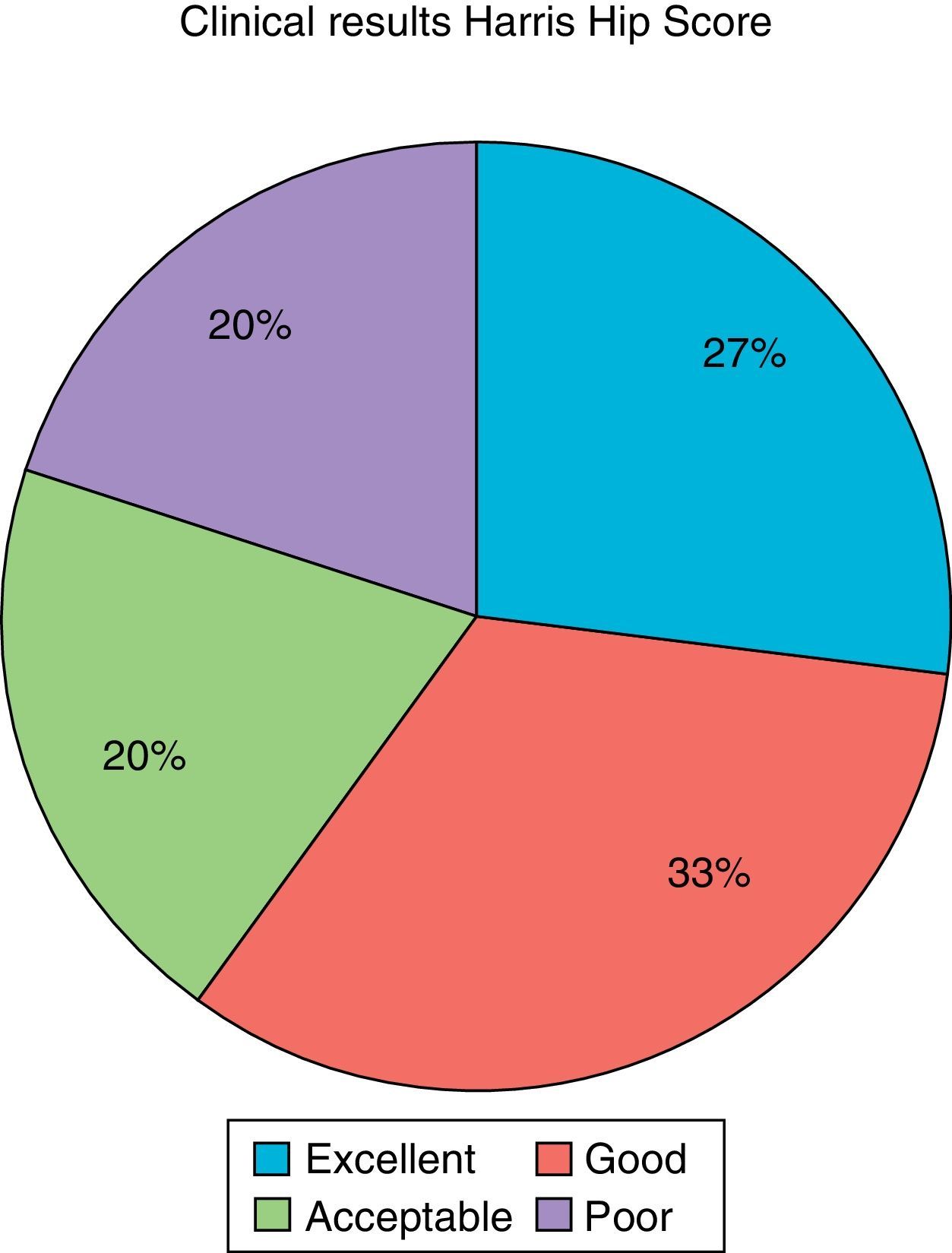
The clinical assessment was carried out through the Harris Hip Score,5 which was completed before the surgery and at the end of the follow-up period. The results were classified as poor when the score was lower than 70, acceptable when it was between 70 and 79, good between 80 and 89, and excellent between 90 and 100.
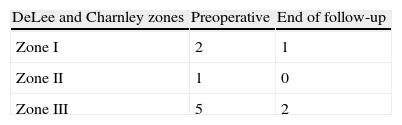
The radiographic assessment included simple radiographs in anteroposterior projection of the pelvis and axial of the hip, comparing the preoperative results with those obtained during follow-up. The presence of radiolucency lines, osteolytic lesions, polyethylene wear and loosening of the components were all analyzed. Osteolytic lesions were located according to the DeLee and Charnley areas.6
ResultsClinical and radiographic controls were carried out at 1, 3, 6 and 12 months, and annually thereafter, for a mean period of 6.1 years (range: 3.5–9.7 years). Two patients died during the follow-up period due to causes not related to the surgery, and the data from their last review were registered for the study.
At the end of the follow-up period, the mean Harris Hip Score was of 80.3 points (range: 52–95), compared with the preoperative score of 64.7 (range: 28–84). Four patients achieved excellent results, 5 were considered good, 3 were acceptable and the remaining 3 were poor. That is, 80% of the patients presented a clinical result which was at least acceptable (Fig. 1).

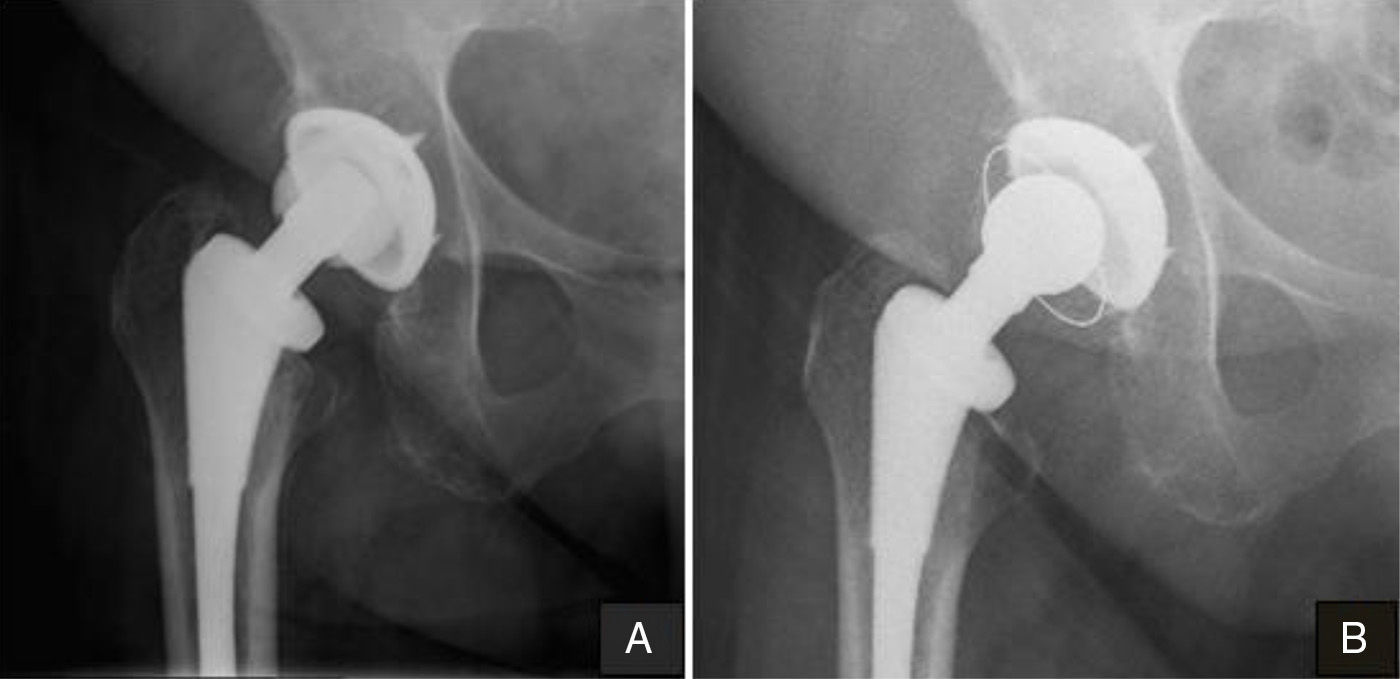
Regarding the radiographic study, no signs of polyethylene wear and no new radiolucency lines were observed. Neither were any new osteolytic lesions found, compared to the preoperative condition (Table 2), and the existing ones were resolved, or at least they did not increase in size (Fig. 2).
 Preoperative radiograph showing polyethylene wear and a periacetabular osteolytic lesion. (B) Radiograph obtained at the end of the follow-up period showing resolution of the osteolytic lesion.")
Only 1 patient required a new revision surgery due to aseptic loosening of the femoral stem, which was replaced by a Solution System® (DePuy Synthes) stem. Another patient (6.7%) presented 2 episodes of dislocation at 4 and 5 months after the intervention, which were reduced without the need for surgery, with a satisfactory clinical evolution.
DiscussionCementing the polyethylene on an osseointegrated metal cup was considered as an alternative in revision surgery for total hip arthroplasty. The only indication to use this technique in the present work was due to polyethylene wear and the lack of availability of a replacement. Other possible indications are failure of the blocking mechanism, recurrent dislocations due to malposition of the acetabular component and dissociation of the polyethylene with respect to the metal ring.7
The surgical technique described by LaPorte et al.8 emphasized the importance of ensuring osseointegration of the acetabular cup before cementing the polyethylene. These authors recommended filling the periacetabular defects with a bone graft, as long as this did not affect the stability of the implant. Otherwise, acetabular replacement should be considered.
The biomechanical analysis of this structure has been assessed in several studies. Haft et al.9 suggested that the most important factor to optimize the results was to achieve a correct union in the cement-polyethylene interface, so in a subsequent work they recommended creating perforations in smooth cups.10 Bonner et al.11 concluded that the stability of this assembly could be superior to that of conventional blocking mechanisms, as long as larger polyethylene inserts were used, and cases requiring a larger size achieved significant improvements by creating circumferential grooves. No differences were found in the present study between cases in which the polyethylene component was oversized to maintain a homogeneous cement layer compared to cases in which the same size as the acetabular cup was implanted. Neither did we find differences in terms of thickness of the cement layer. Delanois et al.12 investigated whether cementing of the polyethylene modified its natural evolution, and did not find significant differences with respect to uncemented cases.
The clinical results obtained in our work were satisfactory, similar to those reported by other authors. Wang et al.13 published a series of 23 hips with a mean follow-up period of 72.3 months and Harris Hip Score of 95.5. The mean age at the time of the revision was 61 years, notably lower than that in our sample. In the series by Yoon et al.,14 92% of the patients had good or excellent results, but with a follow-up period of 2.8 years. Lastly, Callaghan et al.15 did not find statistically significant differences between the Harris Hip Score in the preoperative and at the end of the follow-up period (mean values of 69.9 and 76.8, respectively), although they did find them in the WOMAC subscales of pain and rigidity, as well as in the physical and mental components of the SF-36 questionnaire.
Despite the scientific evidence that the incidence of migration of the components and the presence of radiolucent lines is greater with cemented acetabular components,16 this does not seem to be true when the polyethylene is cemented over the metallic cup. The majority of works examined showed that osteolytic lesions which required a bone graft disappeared, or at least did not progress,17 maintaining a radiographically stable structure.
The complications registered in our work were minimal, with only a single case of dislocation, which accounted for 6.7%, a similar percentage to that registered in other series with the same approach route.18 This rate was lower than that reported by Beaulé et al.,19 with 22%. These authors attributed the instability to the fact that 4 of their 7 cases were converted from a surface prosthesis to a total hip arthroplasty, using a small femoral head size. Likewise, Wilson et al.20 published 1 case of subluxation and early wear of the superior pole of the polyethylene due to an insufficient layer of cement in the superior pole of the implant.
This work is limited by the small sample size, as there are few cases of wear which cannot be resolved by changing the polyethylene with a standard anchor. Therefore, it is not possible to establish statistically significant relationships.
In conclusion, cementing the polyethylene, whenever it is not possible to anchor it, in an osseointegrated metal cup, is a technique that offers good medium-term results for revision surgery of total hip arthroplasty due to polyethylene wear. When conducted with precise indications, it minimizes the complications entailed by replacement of the acetabular component, without compromising stability.
Level of evidenceLevel of evidence iv.
Ethical responsibilitiesProtection of people and animalsThe authors declare that this investigation did not require experiments on humans or animals.
Confidentiality of dataThe authors declare that they have followed the protocols of their workplace on the publication of patient data.
Right to privacy and informed consentThe authors declare having obtained written informed consent from patients and/or subjects referred to in the work. This document is held by the corresponding author.
Conflict of interestThe authors have no conflict of interest to declare.
Please cite this article as: Espinosa-Ruiz A, Zorrilla-Ribot P, Salido-Valle JA. Recambio de polietileno mediante la cementación de un nuevo componente sobre el metal-back osteointegrado. Rev Esp Cir Ortop Traumatol. 2015;59:14–18.
