



To evaluate the quality of life in patients with knee and hip osteoarthritis through self-assessment and those made by the physician.
Materials and methodsAn observational and cross-sectional multicenter study in which 628 traumatologists or rheumatologists evaluated 1849 patients with knee and/or hip osteoarthritis, aged ≥50 years old, and representative of 49 Spanish provinces. Each researcher evaluated three patients and also completed the SF-12v2 health questionnaire. The patients completed the WOMAC and SF-12v2 questionnaires.
ResultsThe patients were 68.5±9.5 years old, 61.5% had knee osteoarthritis, 19% had hip osteoarthritis, and 19.5% in both locations. Older patients and those who had both knee and hip osteoarthritis had a poorer quality of life, according to patients and researchers. Physical health perceived by the researchers was better than patients reported (36.74±8.6 and 35.21±8.53; respectively, p<0.001), and the mental health score was similar between physicians and patients. Kellgren/Lawrence scale and test Timed Up & Go predict better the quality of life, assessed by WOMAC and SF-12v2 questionnaires.
DiscussionThis is the Spanish study on quality of life in osteoarthritis of the knee and hip of larger amplitude and number of patients.
ConclusionThese results could be considered as reference values of Spanish population aged ≥50 years with knee or hip osteoarthritis.
Evaluar la calidad de vida de pacientes con artrosis de rodilla y cadera a través de autovaloraciones y las realizadas por el médico.
Material y métodoEstudio observacional, transversal y multicéntrico en el que 628 traumatólogos o reumatólogos evaluaron a 1.849 pacientes con artrosis de rodilla y/o de cadera con edad mínima de 50 años, distribuidos en 49 provincias españolas. Cada investigador evaluó a tres pacientes y cumplimentó el cuestionario de salud SF-12v2. Los pacientes respondieron los cuestionarios WOMAC y SF-12v2.
ResultadosLos pacientes tenían de 68,5±9,5 años de edad, el 61,5% tenía artrosis de rodilla, el 19% de cadera y el 19,5% en ambas localizaciones. Los pacientes de más edad y los que tenían artrosis de rodilla y de cadera presentaban peor calidad de vida, según la opinión de los pacientes y los investigadores. La salud física percibida por los médicos fue mejor que la manifestada por los pacientes (36,74±8,6 y 35,21±8,53; respectivamente, p<0,001) y la puntuación del componente mental de salud asignada por los pacientes y los médicos fue similar. La Escala de Kellgren/Lawrence y el test Timed Up & Go pronostican mejor la calidad de vida evaluada con los cuestionarios WOMAC y SF-12v2.
DiscusiónEste es el estudio español sobre calidad de vida en artrosis de rodilla y cadera de mayor envergadura por amplitud y número de pacientes.
ConclusionesEstos resultados podrían ser considerados como valores de referencia de población española de 50 años o mayores con artrosis de rodilla y/o de cadera.
Quality of life is defined as “an individual's perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns”.1 Health-related quality of life (HRQoL) covers, among other factors, pain, functional capacity and emotional well-being.2
Osteoarthritis (or arthrosis) significantly decreases the quality of life of patients who suffer it. It is the most prevalent arthropathy throughout the world and knee and/or hip involvement is the most common reason for walking disability among the elderly, from all races and geographical areas. In industrialized countries, 80% of the population aged over 65 suffers osteoarthritis,3 with a higher prevalence being observed in the group aged between 70 and 79 years, and 33.7% of cases affecting the knee.4
The prevalence of osteoarthritis of any joint among the general Spanish population is of 24%, with a male:female ratio of 3:1 among those older than 60 years.5 The prevalence of symptomatic knee osteoarthritis among patients aged over 20 years is of 10.2%, whilst radiological osteoarthritis could reach 34%. Coxarthrosis is relatively frequent after the ages of 50–55 years. According to the series, at this age it can be appear in between 20% and 30% of the population. If we take into account the fact that the hip fulfills a key role in the balance and support of the body, coxarthrosis can be considered as one of the most disabling types of osteoarthritis.
Clinically, osteoarthritis is characterized by joint pain, morning rigidity for a period <30min, limitation of mobility, crepitus, joint instability, functional disability, occasional hemorrhage and a variable degree of local inflammation. The symptoms are insidious and remit with rest. Once the disease advances, pain can be constant when any physical activity is performed and persist for several hours afterwards. Pain, which is accompanied by functional disability, has a mechanical origin, is triggered by use of the joint, especially after it has been inactive, decreases with exercise, reappears when the activity is prolonged and improves with rest until its disappearance.
The progression of osteoarthritis causes a limitation of the activity of the affected joint which, if persistent, will become a permanent functional disability, with all the negative consequences for the patient, whose daily life and work activity, and therefore quality of life will be affected. Osteoarthritis cannot be cured definitively, so treatment strategies aim to reduce the pain and improve the function of the affected limb.
There are no Spanish reference data which estimate the quality of life of patients with osteoarthritis, so the objective of this study was to assess the quality of life of patients with knee and hip osteoarthritis through self-assessments and to determine the perception of physicians about the quality of life of these patients.
Material and methodsThis was an observational, cross-sectional, multicenter study, whose initial calculated population was of 2100 patients who fulfilled the following inclusion criteria: age 50 years or over, having been diagnosed with knee and/or hip osteoarthritis prior to the study through radiological assessment, and who attended consultation at the various Autonomous Regions of the Spanish territory between October 15th 2011 and May 15th 2012.
Out of the 700 physicians who worked at hospitals or health centers specializing in Rheumatology or Traumatology, who considered themselves to have knowledge and experience in knee and hip osteoarthritis and who were invited to participate in the study, 628 responded within the time established previously and according to the protocol. The coordinators of the study contacted the specialists based on geographical criteria, in order to ensure a proportional representation of the entire country. The recruitment of patients was carried out by researchers in a random manner. Each researcher had to recruit 3 patients on different days, the first who attended consultation and fulfilled the inclusion and exclusion criteria. We excluded patients with terminal disease and those unable to understand the instructions of the questionnaires and give their consent, as well as those who suffered any pain not related to knee and/or hip osteoarthritis, with a VAS over 30. After collecting the demographic data from each patient, they completed a questionnaire and also indicated the following clinical variables: location of the osteoarthritis, level of radiological involvement of the joint according to the scale by Kellgren/Lawrence,6 time of evolution of pain, history of falls with and without fractures within the last year, location of fractures, result of the Timed Up & Go test7 and presence of other rheumatologic diseases.
After providing their informed consent in writing, each patient completed the Western Ontario and McMaster Universities Osteoarthritis Index, version LK 3.0 (WOMAC)8,9 and the Medical Outcomes Survey Short Form, version 2 (SF-12v2)10–12 questionnaires. The physicians completed the SF12v2 questionnaire according to their perception of the quality of life of each patient and without knowing their responses.
The WOMAC questionnaire is the most frequently used self-administered specific instrument to asses both the symptoms and functional capacity of patients with knee and/or hip osteoarthritis.8 It contains 24 items covering 3 dimensions: pain, stiffness and functional capacity in general. The lowest score represents less pain and rigidity and better functional capacity. Following the instructions of the authors of the translation and adaptation of the WOMAC questionnaire,8 all doubtful responses due to a position of a mark outside the box were resolved by selecting the closest one. In some exceptional cases in which the mark was equidistant between 2 boxes, we selected the highest score. We considered as non-valid scales the lack of a response by patients to 2 pain items, 2 rigidity items or 4 functional capacity items. When patients left 1 pain item, 1 rigidity item and between 1 and 3 functional capacity items blank, we substituted the missing datum from the item by the average value of the completed items.
The SF-12v2 questionnaire comprises 12 items assessing 8 dimensions defined from the SF-36 questionnaire. The responses are Likert type scales with 3–6 options assessing the intensity or frequency. The responses given by patients and by researchers were standardized and recoded to obtain 2 summary components: physical (SCP) and mental (SCM), through the application of an algorithm which transformed the scores of each individual and standardized them to make them comparable. This action was carried out by QualityMetric Incorporated (USA), a company which applied the original algorithm of the authors of the questionnaire, since it is the only valid and available one for the 2.0 version of the SF-12.
The data were digitalized into a protected, secure and normalized database. Once registered, the data collection sheets were kept in specific archives. We carried out a statistical analysis of the total sample, divided by age into 3 groups: 50–59, 60–69 and ≥70 years and also according to the location of the osteoarthritis: knee and hip. For the numerical variables, we calculated central tendency, dispersion and distribution measurements. For the nominal and categorical variables, we calculated the frequency, created contingency tables and calculated the Pearson's Chi.2 We used score estimation and by 95% confidence intervals (CI) (type I error of 5%) in order to obtain both the sociodemographic profile of the patients and the distribution of the characteristics of osteoarthritis. We assessed the correlation between the scores of the responses of patients to the WOMAC and SF-12v2 questionnaires and those obtained by physicians in the SF-12v2 questionnaire. The analysis of the WOMAC questionnaire included the calculation of the mean values for each of the 3 dimensions: pain, rigidity and functional capacity and their comparison with the means of the scores of the subgroups by age and location of the osteoarthritis using a 1-factor ANOVA and a post hoc test to identify the significant intergroup differences.
In order to detect the factors associated to variability of the WOMAC and SF-12v2 scores, we carried out a stepwise, multiple regression analysis. The independent variables were selected by fixing an initial significance level of 0.10 and 0.05 to include them in the definitive model. We also assessed the multicolinearity of the final model. The statistical analysis was conducted using the software package SPSS 13.0 for Windows. A level of statistical significance of 0.05 was applied in all the tests conducted.
ResultsThe total number of patients included in the final sample was 1849 corresponding to 48 provinces and 16 Spanish Autonomous Regions. We excluded 35 patients who did not fulfill the age stipulated in the study protocol. Of these, 57.1% were females, with a mean age of 69.9±9.4 years (95% CI: 69.3–70.5). The mean age of the males in the sample was 67.8±9.4 years (95% CI: 67.1–68.6). Up to 45.4% of the sample had completed primary studies, 19.3% had no studies and the rest had completed mandatory secondary education, vocational training or above. A total of 46.9% had retired a mean 10.0±7 years earlier (95% CI: 9.6–10.5).
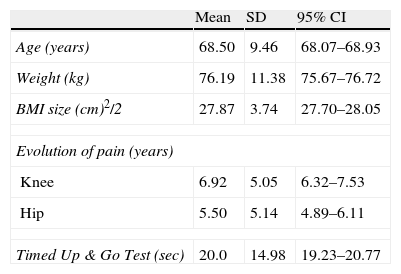
A total of 61.5% of the patients suffered osteoarthritis in the knee, 19% in the hip and 19.5% in both locations. According to the Kellgren/Lawrence scale, 20.2% and 34.4% of patients presented severe or moderate osteoarthritis, respectively. In 23.1% cases, the radiological osteoarthritis involvement was moderate or minimal and in the remaining 22.3% it had been assessed radiologically, but the corresponding value to the Kellgren/Lawrene scale was absent. A total of 75.8% patients lived with someone, and during the past year 20.4% had been admitted to hospital, 22.6% had suffered a fall, resulting in fracture in 34% of cases. In total there were 50 fractures in 209 patients (11.3%). Moreover, 34 (1.84%) and 7 (0.38%) patients suffered 2 and 3 fractures, respectively. The location of these fractures was: Colles (37.3%), hip (24.4%), vertebral (12.9%) and knee (8.7%). The addition of humeral, tibial or fibular, foot and hand fractures corresponded to 16.7%. A further 26.7% presented diagnosis of osteoporosis and between 4% and 8% of patients also suffered polymyalgia, arthritis or fibromyalgia. Table 1 presents other clinical characteristics of the studied sample.
Characteristics of the studied sample.
| Mean | SD | 95% CI | |
| Age (years) | 68.50 | 9.46 | 68.07–68.93 |
| Weight (kg) | 76.19 | 11.38 | 75.67–76.72 |
| BMI size (cm)2/2 | 27.87 | 3.74 | 27.70–28.05 |
| Evolution of pain (years) | |||
| Knee | 6.92 | 5.05 | 6.32–7.53 |
| Hip | 5.50 | 5.14 | 4.89–6.11 |
| Timed Up & Go Test (sec) | 20.0 | 14.98 | 19.23–20.77 |
95% CI: 95% confidence interval; BMI: body mass index; SD: standard deviation.
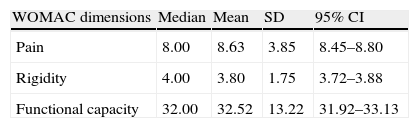
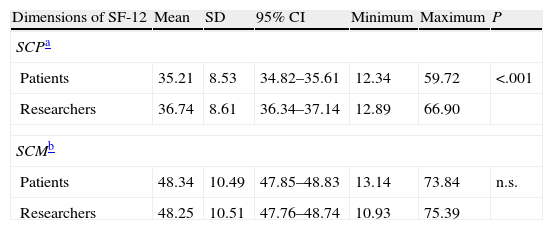
In total, 99.24% of patients responded to the WOMAC questionnaire; the scores are shown in Table 2. The rate of response of patients to the SF-12v2 questionnaire was of 95.89%, whilst the figure for researchers was 96.32%. The mean HRQoL scores obtained through the SF-12v2 were lower compared to the reference value for the US, which is 50. The perception by patients of their health status differed from that of their physicians in the dimensions: physical function, body pain and general health, which is reflected in the SCP (Table 3).
Score in the WOMAC questionnaire for knee and hip osteoarthritis completed by patients.
| WOMAC dimensions | Median | Mean | SD | 95% CI |
| Pain | 8.00 | 8.63 | 3.85 | 8.45–8.80 |
| Rigidity | 4.00 | 3.80 | 1.75 | 3.72–3.88 |
| Functional capacity | 32.00 | 32.52 | 13.22 | 31.92–33.13 |
95% CI: 95% confidence interval; SD: standard deviation; WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index, version LK 3.0.
Distribution of scores from the SF-12v2 health questionnaire responded by patients and researchers.
| Dimensions of SF-12 | Mean | SD | 95% CI | Minimum | Maximum | P |
| SCPa | ||||||
| Patients | 35.21 | 8.53 | 34.82–35.61 | 12.34 | 59.72 | <.001 |
| Researchers | 36.74 | 8.61 | 36.34–37.14 | 12.89 | 66.90 | |
| SCMb | ||||||
| Patients | 48.34 | 10.49 | 47.85–48.83 | 13.14 | 73.84 | n.s. |
| Researchers | 48.25 | 10.51 | 47.76–48.74 | 10.93 | 75.39 | |
95% CI: 95% confidence interval; SD: standard deviation.
The WOMAC scores were significantly correlated with those of the SF12-v2 in the dimensions assessing physical health, both from the perception of patients (pain: r=−0.627, P<.001; rigidity: r=−0.586, P=<.001 and functional capacity: r=−0.736, P<.001) and of researchers (r=−0.514, P<.001; r=−0.493, P<.001 and r=−0.595, P<.001, respectively).
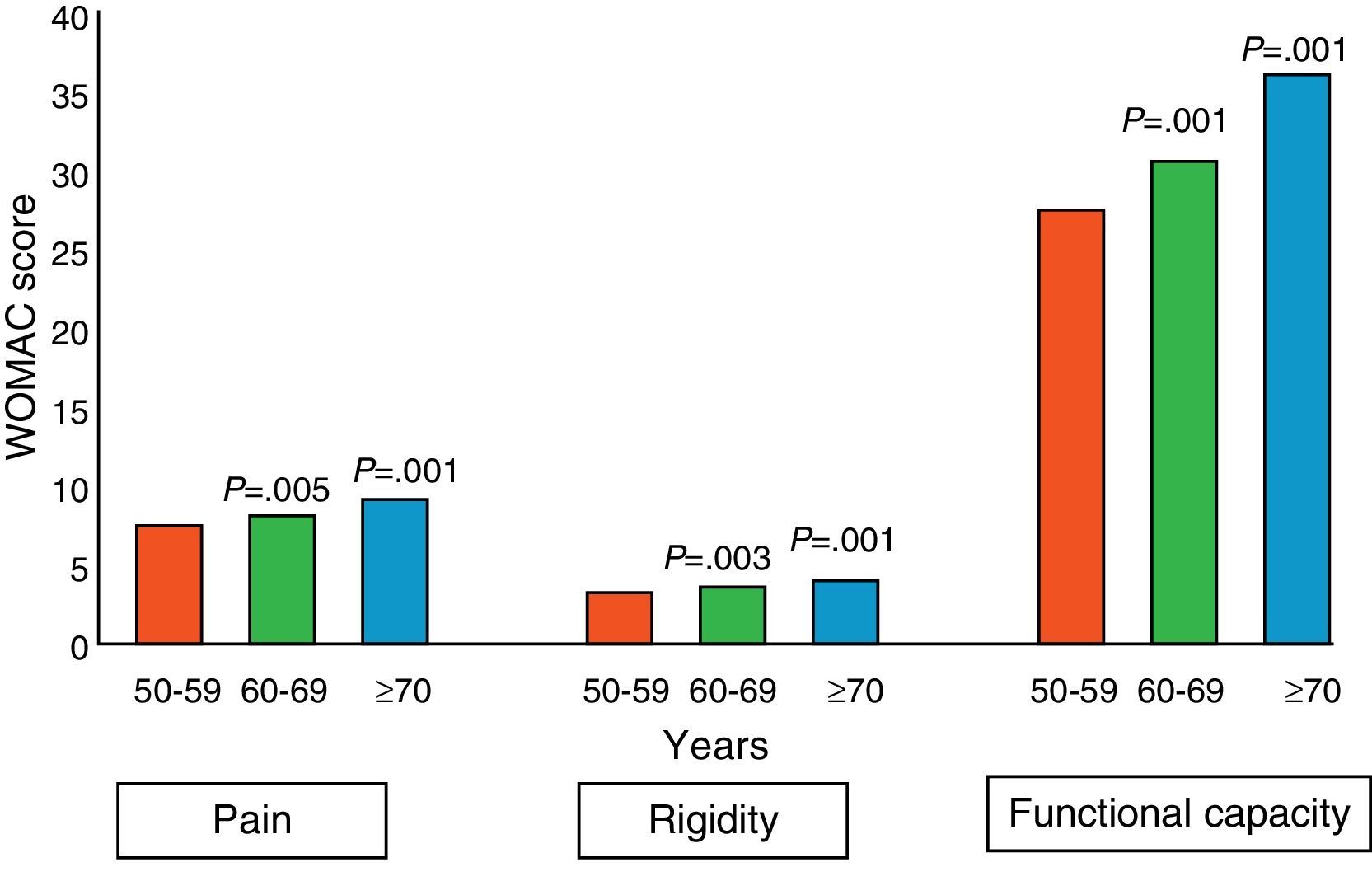
The analysis of the sample grouped by ages showed that the frequency of fractures associated to falls was 12% in the group aged between 50–59 years, 21.2% in the group aged between 60–69 years and 66.8% among patients aged ≥70 years. The WOMAC scores worsened significantly as age increased (Fig. 1). Both patients and researchers assigned worse scores in physical and mental health assessed through the SF-12v2 to the group of patients aged 70 years or over, (P<.001, in relation to the other two, younger age groups) and also a worse score in the physical component for patients aged between 60 and 69 years (P<.05) than the group aged under 60 years.

When analyzing the sample grouped by the location of osteoarthritis into 3 groups: knee, hip and both knee and hip, we found a frequency of fractures of 40.6% among patients with knee osteoarthritis, 20.8% among those with hip osteoarthritis and 38.6% among patients with osteoarthritis in both locations. The scores of the 3 dimensions assessed by the WOMAC revealed a significant difference between the 3 groups, with the worse assessment found in the group of patients with osteoarthritis in both locations. According to the assessment of patients through the SF-12v2 questionnaire, osteoarthritis in both locations worsened physical and mental health when compared to the presence of osteoarthritis in a single joint (P<.001). The same result was obtained through the responses of researchers, but, in addition, their scores showed a significant difference (P<.05) between patients with knee osteoarthritis and patients with hip osteoarthritis in the dimensions of body pain, general health and social function, which corresponded to the physical component.
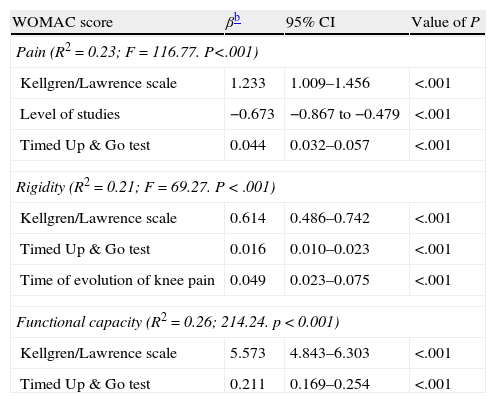
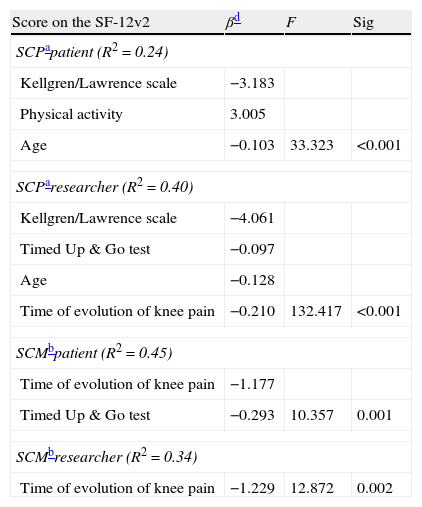
The result of the multivariate analysis of the association between the WOMAC scores and the characteristics of patients is presented in Table 4. Both the Kellgren/Lawrence scale and the Timed UP & Go test were significantly associated with the WOMAC in its 3 dimensions, as well as with the scores of the SF-12v2 (Table 5). In this case, age and the time of evolution of knee pain also showed a significant association.
Association between the characteristics of the participants in the study and scores on the WOMAC questionnaire (n=1835).a
| WOMAC score | βb | 95% CI | Value of P |
| Pain (R2=0.23; F=116.77. P<.001) | |||
| Kellgren/Lawrence scale | 1.233 | 1.009–1.456 | <.001 |
| Level of studies | −0.673 | −0.867 to −0.479 | <.001 |
| Timed Up & Go test | 0.044 | 0.032–0.057 | <.001 |
| Rigidity (R2=0.21; F=69.27. P<.001) | |||
| Kellgren/Lawrence scale | 0.614 | 0.486–0.742 | <.001 |
| Timed Up & Go test | 0.016 | 0.010–0.023 | <.001 |
| Time of evolution of knee pain | 0.049 | 0.023–0.075 | <.001 |
| Functional capacity (R2=0.26; 214.24. p<0.001) | |||
| Kellgren/Lawrence scale | 5.573 | 4.843–6.303 | <.001 |
| Timed Up & Go test | 0.211 | 0.169–0.254 | <.001 |
95% CI: 95% confidence interval; WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index, version LK 3.0.
Association between the characteristics of participants in the study and the score on the SF-12v2 questionnaire according to the responses of patients and researchers (n=1773).c
| Score on the SF-12v2 | βd | F | Sig |
| SCPapatient (R2=0.24) | |||
| Kellgren/Lawrence scale | −3.183 | ||
| Physical activity | 3.005 | ||
| Age | −0.103 | 33.323 | <0.001 |
| SCParesearcher (R2=0.40) | |||
| Kellgren/Lawrence scale | −4.061 | ||
| Timed Up & Go test | −0.097 | ||
| Age | −0.128 | ||
| Time of evolution of knee pain | −0.210 | 132.417 | <0.001 |
| SCMbpatient (R2=0.45) | |||
| Time of evolution of knee pain | −1.177 | ||
| Timed Up & Go test | −0.293 | 10.357 | 0.001 |
| SCMbresearcher (R2=0.34) | |||
| Time of evolution of knee pain | −1.229 | 12.872 | 0.002 |
This study assessed the perception of quality of life among patients with knee and hip osteoarthritis from the perspectives of both patients and physicians. This is the most extensive study on quality of life in patients with knee and hip osteoarthritis conducted in Spain, both in terms of number of patients and in scope, as it included researchers and patients from 16 Spanish Autonomous Regions, so we estimate that its results could be considered as reference values for the Spanish population aged 50 years and older, with knee and/or hip osteoarthritis. The selection of patients limited by age, was based on the prevalence of knee13 and hip osteoarthritis among the Spanish population and on the clinical criteria of the ACR which are the most extensively used and validated.14
Collection of sociodemographic and clinical data was carried out through a specially designed instrument, whereas the quality of life of patients with osteoarthritis was assessed with the WOMAC questionnaire,8,9 which is a specifically adapted and validated instrument for the Spanish population, and widely used in clinical practice. The SF-12v2 questionnaire,10–12 in its Spanish version, was applied as a generic instrument to assess HRQoL, as it reproduces the reliability and validity of the SF-36 and because it is the questionnaire recommended to assess samples of over 500 individuals.15 Since we did not have reference values for the SF-12v2 for the general Spanish population, we proceeded like other authors,16 that is, the scores were standardized and recoded according to the values of the American population, as recommended to compare the data from populations of different countries.12
As for the validation of the Spanish version of the WOMAC,9 where the results are correlated to the dimensions of the generic SF-36 questionnaire, in this study we observed a significant correlation of the WOMAC with the dimensions of the SF-12v2 which assess physical health.9,17
Both patients and researchers gave higher scores to HRQoL in its mental dimension than to quality of life related to physical health of patients with osteoarthritis, with similar SCM values in both groups (48.34 vs 48.25, respectively). This result agrees with the assessment obtained using the SF-12v2 questionnaire, among the Spanish diabetic population.16
One of the objectives of this study was to contrast the values of the SF-12v2 as completed independently by patients and researchers in order to compare their perceptions of the health of patients. The results indicate that physical health perceived by physicians was better than that indicated by patients, since the score in three of the dimensions assessing the physical component was significantly higher than that assigned by the patients (SCP=36.74±8.61 vs 35.21±8.53; P<.001).
HRQoL as assessed by the SF-12v2 and WOMAC questionnaires became worse as the age of the patients increased, becoming more evident in the scores which measured physical function in patients aged ≥70 years, which could be explained by the fact that osteoarthritis is a progressive disease and, in addition, in this group of patients, the time of evolution of pain may have been longer. This result corroborates the objective tests conducted on all patients. Older patients presented the highest percentage of radiological evidence of severe osteoarthritis determined by the Kellgren/Lawrence scale, and also required more time to conduct the Timed Up & Go test,18 a simple test which is recommended for use in medical consultation with elderly patients19 to assess functional capacity, and which easily detects physical limitations in these patients with hip and knee osteoarthritis. The test has proven, adequate sensitivity and specificity to identify patients at risk of falls in certain studies.20
The WOMAC score in the dimension of pain was similar among patients with osteoarthritis in the hip and knee, but worsened when both joints were affected. Rigidity was greater and a worse functional capacity was observed among patients who suffered osteoarthritis in the hip or in both locations than among patients who suffered knee osteoarthritis. The perception of quality of life by patients with knee or hip osteoarthritis was similar, but significantly worse among patients with osteoarthritis in both locations. The researchers agreed with patients in their assessments of HRQoL and the scores indicate that patients with hip osteoarthritis suffer more body pain, have worse general health and social function than patients with knee osteoarthritis. In a study which assessed the perception of HRQoL following total knee and hip arthroplasties, patients in the knee group perceived a worse quality of life than patients in the hip group in the preoperative period. However, 1 year after the arthroplasty, this perception became inverted.21
Our results suggest that the scale of radiological osteoarthritis degrees by Kellgren/Lawrence and the Timed Up & Go test which objectively determine joint damage and functional capacity, respectively, are the most influential factors in the score of the 3 dimensions of the WOMAC questionnaire: pain, rigidity and functional capacity and to a similar extent among patients with osteoarthritis in the knee, hip and both locations. The level of education was a factor with an inverse and significant influence on the perception of pain by patients with knee osteoarthritis and a direct relationship was observed between the body mass index and rigidity among patients with knee and hip osteoarthritis, probably due to the fact that joint function is worse among overweight patients.
The values of the Kellgren/Lawrence scale and the Timed Up & Go test, in addition to age, had the greatest influence on the scores of the items of the SF-12v2 which assessed physical health, according to the information obtained from patients and their physicians. The need to assess the level of osteoarthritis through objective tests was determining for the selection of researchers, since specialists are most frequently responsible for requesting radiological tests.
Regarding mental health, both patients and researchers included as a determining factor the time of evolution of pain. It is known that patients with chronic pain suffer a progressive reduction of social life and happiness, as the time suffering physical pain and perceiving a reduction of their autonomy increases.
The studied sample represented the Spanish population and the distribution according to Autonomous Regions was proportional to each of their populations, but this was not adhered to strictly in all cases, thus representing a limitation of this study.
We assessed the comorbidity of osteoporosis, polymyalgia, arthritis and fibromyalgia. Only the presence of osteoporosis appeared as a factor affecting the functional capacity of patients with hip osteoarthritis.
The decrease in quality of life reported by patients with knee and hip osteoarthritis was perceived in a similar manner by the rheumatologists and traumatologists. These results could be considered as reference values for the Spanish population aged 50 years or above and suffering knee and/or hip osteoarthritis.
Level of evidenceLevel of evidence III.
Ethical responsibilitiesProtection of people and animalsThe authors declare that this investigation did not require experiments on humans or animals.
Confidentiality of dataThe authors declare that they have followed the protocols of their workplace on the publication of patient data.
Right to privacy and informed consentThe authors declare having obtained written informed consent from patients and/or subjects referred to in the work. This document is held by the corresponding author.
Conflict of interestsThe pharmaceutical company “Laboratorios Farmacéuticos ROVI” financed the printing, distribution and collection of questionnaires, but did not participate in data analysis and the drafting of the manuscript.
The authors wish to thank all traumatologists and rheumatologists who assessed participating patients.
Please cite this article as: Bernad-Pineda M, de las Heras-Sotos J, Garcés-Puentes MV. Calidad de vida en pacientes con artrosis de rodilla y/o cadera. Rev Esp Cir Ortop Traumatol. 2014;58:283–289.
