



The COVID-19 pandemic has led to the confinement of approximately one third of the world population, causing a drastic change in the activities of daily life with many repercussions at the health, economic and social levels.
ObjectivesThe objective of the present work is to present the epidemiological variations in the production of fractures in the period of mandatory confinement in our reference population.
MethodsAnalytical retrospective comparative study of two groups of patients: Group A: patients admitted before the state of alarm that forced confinement in the period from January 13 to March 13 compared to Group B: patients admitted in the two months of confinement, until the de-escalation period began, March 13-May 13. Epidemiological variables including age, personal history, type of fracture, mechanism of injury, outpatient rate, and hospital stay were recorded.
ResultsA total of 190 patients were included. 112 in the pre-confinement period and 78 in the confinement (30% decrease). The mean age (p = 0.007) and falls at home (p < 0.001) were higher in the confinement group. The postoperative (p = 0.006) and overall (p < 0.001) hospital stay were significantly less in the confinement group. No differences were found in the anatomical location of the lesion, sex, comorbidities, mechanism of injury, outpatient rate, or death.
ConclusionsBased on the results of our study, the period of forced confinement due to the COVID-19 pandemic has produced a drastic decrease in the total number of fractures admitted to the traumatology service of a third level hospital. On the other hand, osteoporotic hip fractures have not varied in their incidence and a decrease in the average postoperative and overall stay has been observed.
La pandemia por COVID-19 ha supuesto el confinamiento de aproximadamente un tercio de la población mundial, provocando un cambio drástico en las actividades de la vida diaria con enorme impacto sanitario, económico y social.
ObjetivosEl objetivo de este trabajo es presentar las variaciones epidemiológicas en la producción de fracturas en el período de confinamiento obligatorio en nuestra población de referencia.
Material y métodosEstudio analítico retrospectivo comparativo de dos grupos de pacientes: Grupo A: personas ingresadas antes del estado de alarma que obligó al confinamiento en el período del 13 enero al 13 de marzo vs. Grupo B: individuos atendidos durante los dos meses de confinamiento, hasta que comenzó la desescalada, período del 13 marzo al 13 mayo. Se registraron variables epidemiológicas, incluyendo edad, antecedentes personales, tipo de fractura, mecanismo de lesión, porcentaje de ambulatorización y estancia hospitalaria.
ResultadosSe incluyeron un total de 190 pacientes. En el período de pre-confinamiento 112 y en el confinamiento 78 (disminución del 30%). La edad media (p = 0,007) y las caídas en domicilio (p < 0,001) fueron mayores en este último grupo. La estancia hospitalaria postoperatoria (p = 0,006) y global (p < 0,001) resultaron significativamente menores en el mismo grupo. No se encontraron diferencias en la localización anatómica de la lesión, el sexo, las comorbilidades, el mecanismo de lesión, la tasa de ambulatorización ni el éxitus.
ConclusionesCon base en los resultados de nuestro estudio, el período de confinamiento forzoso por la pandemia de COVID-19 ha producido una drástica disminución del número total de fracturas ingresadas en el servicio de traumatología de un hospital de tercer nivel. Por otro lado, las fracturas osteoporóticas de cadera que requirieron tratamiento quirúrgico no variaron en número y se ha constatado un decremento de la estancia media postoperatoria y global.
The recent declaration of the COVID-19 pandemic by the World Health Organisation on 10 March this year led to the confinement of approximately one third of the world’s population, causing a drastic change in the activities of daily living of most of the inhabitants of the affected countries, with major economic, occupational and social changes.1–3 In Europe, Italy, Spain and France, in decreasing order of prevalence and incidence,4 have been the most affected, and in Spain, at the time of writing, the number of deaths is close to 28,000, with a total of 229,398 infected cases.5 But confinement has not only led to a decrease in outdoor activities, whether in sports venues or in the workplace, it has also resulted in more activities at home that we were not used to doing in our own homes. These facts, taken together, have probably led to a decrease in the total number of fractures diagnosed, not only because their incidence has directly decreased, but also because very often patients have decided not to go to hospital to confirm or discount these injuries due to the risk of infection by COVID-19.3,6
In the history of humanity, the so-called “Spanish flu” in 1918–1919 remains the epidemic that caused the most deaths worldwide, ranging from 50 to 100 million.7 The dreadful consequences of that epidemic, aggravated by the socio-sanitary conditions of the time and the high rate of bacterial over-infection due to the ineffectiveness of the existing antibiotics, are clearly behind us. However, although living conditions and development in our country have improved radically, the virulence of COVID-19 and the social alarm at the growing number of infections and deaths secondary to this virus have triggered the greatest social and health crisis in Spain and Europe of the last 100 years.
The objective of this study is to present the variation in hospital admissions for fractures with surgical indication during the period of compulsory confinement in our reference population. The hypothesis is that confinement drastically decreases the number of fractures and the average length of hospital stay of admitted patients.
Material and methodsAfter approval by the healthcare ethics committee, a retrospective historical cohort study was conducted, comparing fractures admitted to a tertiary level hospital during the COVID-19 pandemic with those treated during the pre-pandemic stage in the same institution. The pre-pandemic cohort included the period from 13 January to 13 March 2020 (start of confinement) and the pandemic cohort the period from 14 March to 13 May 2020 (start of de-escalation).
The inclusion criteria for the study were patients with a diagnosis of fracture with criteria for admission for surgery.
The exclusion criteria were patients who refused hospital admission and those in whom the mechanism for the fracture could not be determined.
The epidemiological variables, age, sex, personal history, risk factors and those related to the fracture were recorded, with special interest in the type and mechanism of injury, and location where it occurred (Tables 1 and 2). Mean pre-surgical, post-surgical and overall mean hospital stay were recorded (Table 3), as well as the percentage of outpatients, i.e., patients not admitted and undergoing surgery on an outpatient basis.
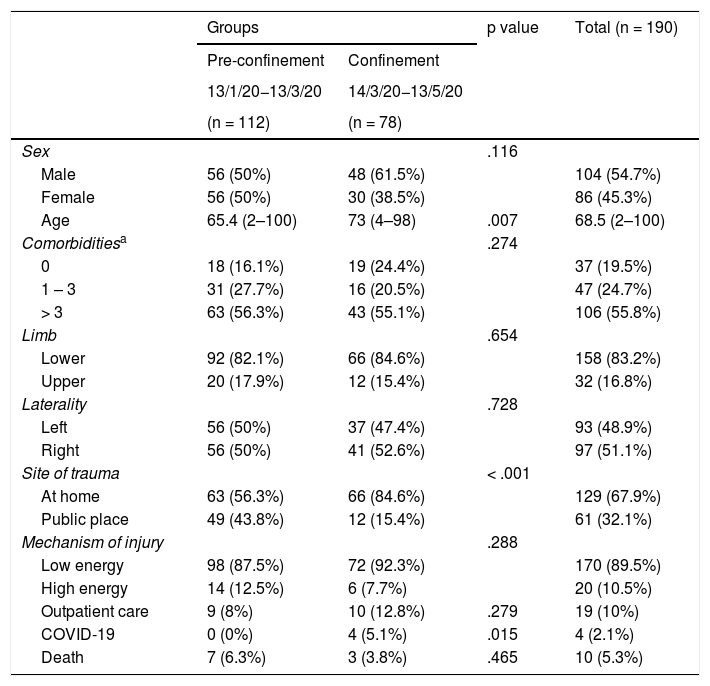
Epidemiological analysis.
| Groups | p value | Total (n = 190) | ||
|---|---|---|---|---|
| Pre-confinement | Confinement | |||
| 13/1/20−13/3/20 | 14/3/20−13/5/20 | |||
| (n = 112) | (n = 78) | |||
| Sex | .116 | |||
| Male | 56 (50%) | 48 (61.5%) | 104 (54.7%) | |
| Female | 56 (50%) | 30 (38.5%) | 86 (45.3%) | |
| Age | 65.4 (2–100) | 73 (4–98) | .007 | 68.5 (2–100) |
| Comorbiditiesa | .274 | |||
| 0 | 18 (16.1%) | 19 (24.4%) | 37 (19.5%) | |
| 1 – 3 | 31 (27.7%) | 16 (20.5%) | 47 (24.7%) | |
| > 3 | 63 (56.3%) | 43 (55.1%) | 106 (55.8%) | |
| Limb | .654 | |||
| Lower | 92 (82.1%) | 66 (84.6%) | 158 (83.2%) | |
| Upper | 20 (17.9%) | 12 (15.4%) | 32 (16.8%) | |
| Laterality | .728 | |||
| Left | 56 (50%) | 37 (47.4%) | 93 (48.9%) | |
| Right | 56 (50%) | 41 (52.6%) | 97 (51.1%) | |
| Site of trauma | < .001 | |||
| At home | 63 (56.3%) | 66 (84.6%) | 129 (67.9%) | |
| Public place | 49 (43.8%) | 12 (15.4%) | 61 (32.1%) | |
| Mechanism of injury | .288 | |||
| Low energy | 98 (87.5%) | 72 (92.3%) | 170 (89.5%) | |
| High energy | 14 (12.5%) | 6 (7.7%) | 20 (10.5%) | |
| Outpatient care | 9 (8%) | 10 (12.8%) | .279 | 19 (10%) |
| COVID-19 | 0 (0%) | 4 (5.1%) | .015 | 4 (2.1%) |
| Death | 7 (6.3%) | 3 (3.8%) | .465 | 10 (5.3%) |
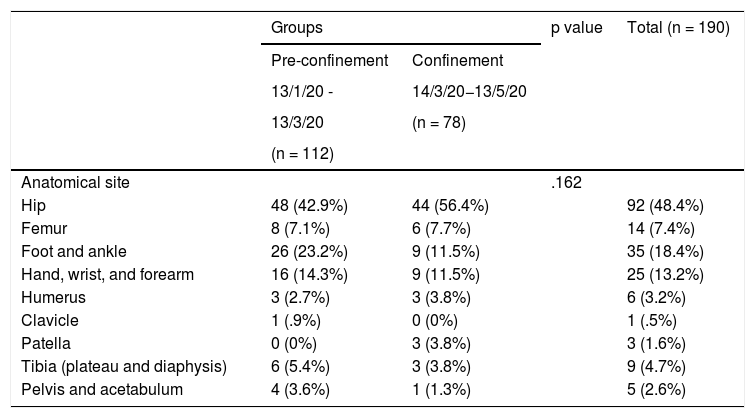
Anatomical site of the fractures.
| Groups | p value | Total (n = 190) | ||
|---|---|---|---|---|
| Pre-confinement | Confinement | |||
| 13/1/20 - | 14/3/20−13/5/20 | |||
| 13/3/20 | (n = 78) | |||
| (n = 112) | ||||
| Anatomical site | .162 | |||
| Hip | 48 (42.9%) | 44 (56.4%) | 92 (48.4%) | |
| Femur | 8 (7.1%) | 6 (7.7%) | 14 (7.4%) | |
| Foot and ankle | 26 (23.2%) | 9 (11.5%) | 35 (18.4%) | |
| Hand, wrist, and forearm | 16 (14.3%) | 9 (11.5%) | 25 (13.2%) | |
| Humerus | 3 (2.7%) | 3 (3.8%) | 6 (3.2%) | |
| Clavicle | 1 (.9%) | 0 (0%) | 1 (.5%) | |
| Patella | 0 (0%) | 3 (3.8%) | 3 (1.6%) | |
| Tibia (plateau and diaphysis) | 6 (5.4%) | 3 (3.8%) | 9 (4.7%) | |
| Pelvis and acetabulum | 4 (3.6%) | 1 (1.3%) | 5 (2.6%) | |
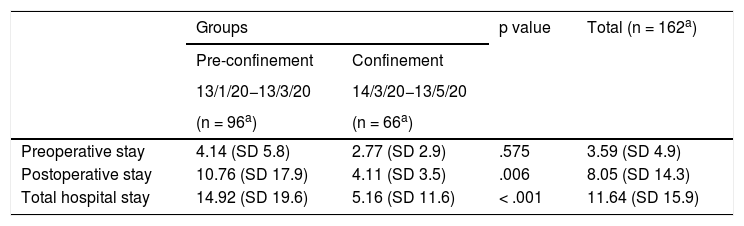
General hospital stay.
| Groups | p value | Total (n = 162a) | ||
|---|---|---|---|---|
| Pre-confinement | Confinement | |||
| 13/1/20−13/3/20 | 14/3/20−13/5/20 | |||
| (n = 96a) | (n = 66a) | |||
| Preoperative stay | 4.14 (SD 5.8) | 2.77 (SD 2.9) | .575 | 3.59 (SD 4.9) |
| Postoperative stay | 10.76 (SD 17.9) | 4.11 (SD 3.5) | .006 | 8.05 (SD 14.3) |
| Total hospital stay | 14.92 (SD 19.6) | 5.16 (SD 11.6) | < .001 | 11.64 (SD 15.9) |
SD: standard deviation.
The patients’ characteristics were summarised showing the frequencies and their respective percentages. The different epidemiological characteristics analysed with respect to belonging to the pre-confinement or confinement group were compared using the X2 test and in the case of 2 × 2 tables, the Yates correction. A student’s t-test was used to compare the age variable treated as a continuous variable. Group comparisons of quantitative and ordinal variables were performed with the Student’s t-test, Mann–Whitney test, or analysis of variance (ANOVA), as appropriate. Probability values of less than .05 were considered significant. The SPSS statistical package (IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY) was used for the data analyses.
ResultsIn the pre-pandemic period 112 patients were admitted and in the pandemic stage this number decreased to 78, representing a decrease of 30.4% (Table 1). The age of the cases who underwent surgery during confinement was higher (73 [4–98]) than those operated in the pre-pandemic control group (65.4 [2–100]) (Table 1). In the case of forced confinement, there was a statistically significant increase in the occurrence of fractures at home in patients under 55 years of age. No significant differences were found in terms of sex, comorbidities, preferential involvement of the upper or lower limb, laterality, mechanism of injury, percentage of outpatient care or deaths.
No statistically significant differences were found in terms of the anatomical location of the injury (Table 2).
Only four COVID-19 positive cases were diagnosed in our series (three with hip fractures and one with an ankle fracture), none required admission to the intensive care unit.
Regarding mean hospital stay, statistically significant differences were observed in reduction of postoperative stay (10.76 before vs. 4.11 after) and in total hospital stay (14.92 vs. 5.16) (Table 3).
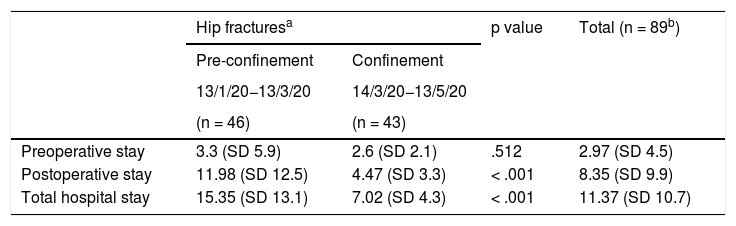
Regarding hip fractures, although the total number of fractures was maintained (48 before vs. 44 in the pandemic period), the reduction in overall length of stay was statistically significant (15.35 days vs. 7.02) (Table 4).
Hospital stay of hip fractures.
| Hip fracturesa | p value | Total (n = 89b) | ||
|---|---|---|---|---|
| Pre-confinement | Confinement | |||
| 13/1/20−13/3/20 | 14/3/20−13/5/20 | |||
| (n = 46) | (n = 43) | |||
| Preoperative stay | 3.3 (SD 5.9) | 2.6 (SD 2.1) | .512 | 2.97 (SD 4.5) |
| Postoperative stay | 11.98 (SD 12.5) | 4.47 (SD 3.3) | < .001 | 8.35 (SD 9.9) |
| Total hospital stay | 15.35 (SD 13.1) | 7.02 (SD 4.3) | < .001 | 11.37 (SD 10.7) |
SD: Standard Deviation.
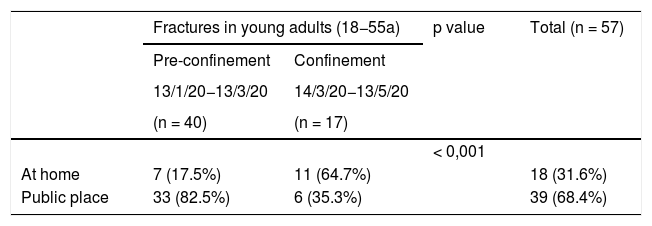
Finally, there was a statistically significant difference in the occurrence of fractures at home, in patients under 55 years of age, from 17.5% in the control stage to 64.7% during confinement (Table 5).
DiscussionThe results of our study show a dramatic decrease in the total number of admissions for fracture to a trauma department due to forced confinement, with a reduction of 30.4% during the pandemic period compared to the pre-pandemic stage (112 vs. 78). This percentage of 30% is similar to that published by French authors in the same study period.8 The decrease in the overall number of fractures admitted is directly related to the decrease in the total number of patients seen in the emergency department. Recent publications state that the decrease (between 50%–60%9) in diseases seen in the emergency department not related to respiratory infections or possible cases of COVID-19 infection is striking. Non-essential work being halted has resulted in a clear decrease in the number of occupational and traffic accidents and, on the other hand, confinement of the population has resulted in an absence of injuries related to accidental falls in public places and outdoor or team sports. However, the important psychological factor that has accompanied this pandemic must not be forgotten, with almost 30,000 recorded deaths and its omnipresence in the press and social networks. Another key reason for the fall in the number of fractures admitted is likely to have been that patients have felt afraid to go to hospital.3,6 Perhaps, from this point on, there will be a phase of traumatic sequelae due to delayed treatment, which will be interesting to examine in future studies.
A detailed analysis of the reduced number of fractures shows that it has not been homogeneous for all types. Thus, osteoporotic hip fractures, typical in older patients, have not varied substantially (46 vs. 43), which has recently been published by other authors in our country.10 However, Italian researchers have recently published a reduction in the total number of hip fractures admitted in two hospitals in the north of Italy, also comparing the pre-pandemic period with the pandemic period.11 It seems logical that these proportions should be maintained in our study if we consider that most fractures in these cases occur in the home. Likewise, the maintenance of the proportion of older patients with hip fracture admitted and the relative decrease in other younger population groups, has meant that the mean age of our pandemic series is higher than the pre-pandemic (73 vs. 65.4) series. Overall, hip fractures accounted for 56.4% of the total fractures admitted, figures very similar to those published by Zhu et al.12 in China (58.3%), where the pandemic originated.
At the other end of the population pyramid, we only saw two fractures in the paediatric age group, the same number as the total number of admissions in the pre-pandemic period, both figures (before and during the pandemic) being unusually low in our centre. In this sense, a recent publication reports a striking decrease in the number of paediatric fractures worldwide,13 also understandable because it has been impossible for children to play or practise sport, which is the main cause of these injuries in this population.
Regarding the mechanisms of injury and places where fractures occurred, it is clear that most fractures were sustained in the home (84% vs. 56% in the pre-pandemic period). This may seem simple to explain, as people were not allowed to leave home, injuries could only occur at home. However, we are struck by the high percentage of fractures occurring at home in the population apparently without associated risk factors. Understanding that most of the injuries were due to low-energy mechanisms within the home, we performed a specific analysis of the 18–55 age group (considered a group of healthy patients) (Table 5), and found a statistically significant increase in fractures at home in this age group. This can only be explained by the fact that sports and recreational activities were likely to have been undertaken in unsuitable premises, with unsuitable footwear and perhaps by people unaccustomed to these activities. On the other hand, the confinement meant that homeowners were performing DIY tasks, minor repairs or even doing up their homes, since non-essential work was prohibited. This was found in up to four cases in our series, and although we cannot infer a direct relationship, undertaking “unusual” activities in the home may be one of the predisposing causes of fractures.
We followed the recommendations of the Spanish Society of Orthopaedic Surgery and Traumatology (SECOT) with regard to COVID-19 infection in hospitalised patients,14 and the guidelines of the Ministry of Health.15 We redistributed tasks within the service by work team, with rest days and taking the recommended contact and hygiene precautions.15–17 In relation to elective surgery, also following the recommendations of SECOT and the Ministry, all elective surgery was suspended, except for septic and tumour surgery, as recommended by other authors.18–21
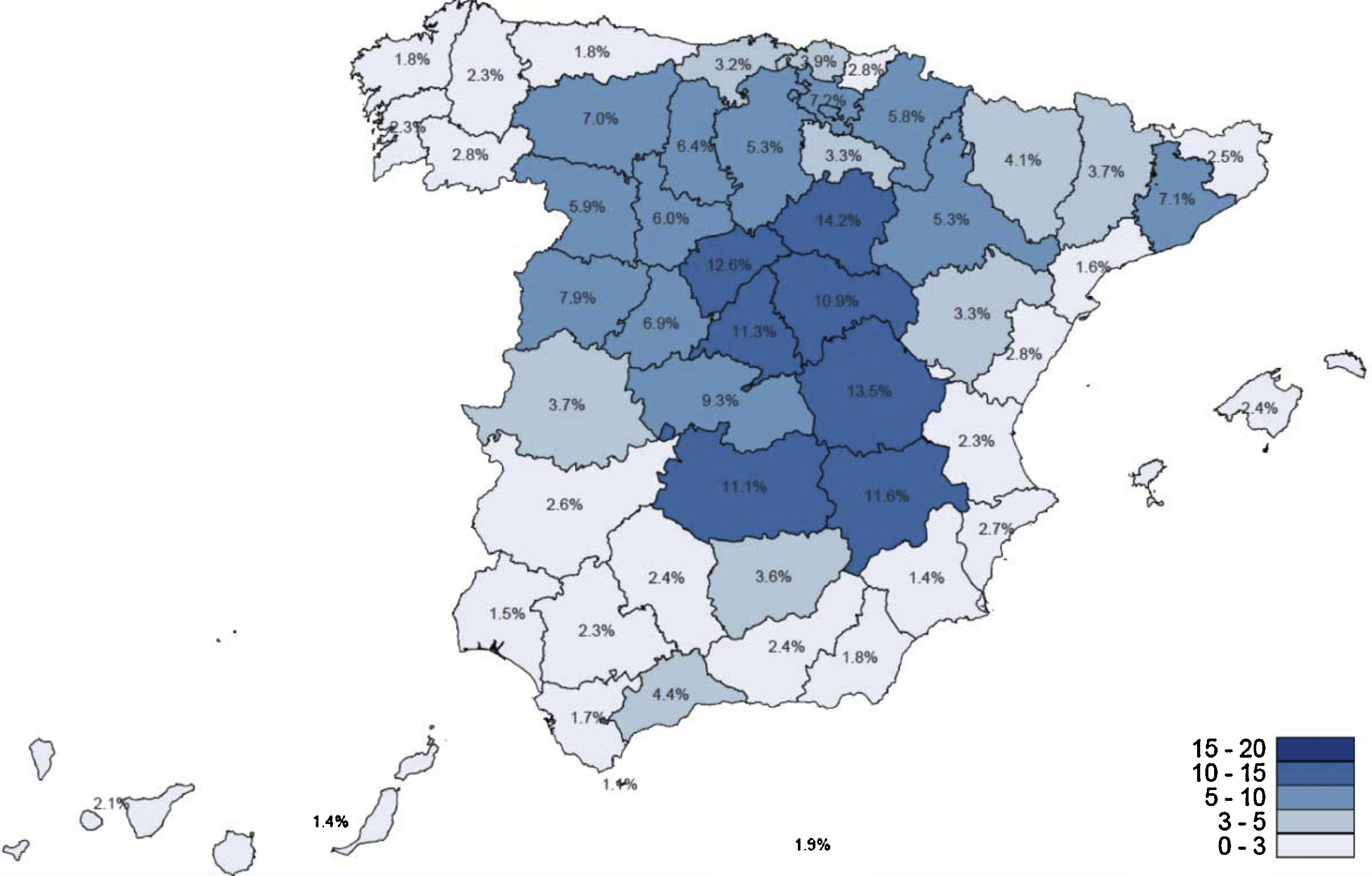
The specific nature of our geographical area, its insularity, has perhaps contributed to it being one of the areas of Spain with the lowest number of COVID-19 cases. The incidence of the disease in our autonomous region is among the lowest in Spain, with 2,365 cases at the time of writing,22 with a cumulative incidence of 109.83 cases per 100,000 inhabitants, and the preliminary seroprevalence study23 (presence of IgG antibodies to COVID-19) conducted in Spain detected 1.8% in the entire community (Fig. 1). Regarding infection by COVID-19, in our series only four patients were diagnosed (of whom three were hip fractures), all nosocomial origin, as they began with clinical symptoms five to 10 days after admission.24
.")
No significant differences were observed in relation to mean preoperative stay, although there was a reduction that contributed to a decrease in overall mean stay, which may be because elective surgery, in this period, except for tumour and/or septic surgery, was suspended by order of the Regional Ministry of Health, operating theatres being available for fractures.
In terms of overall mean hospital stay, the difference between the control and confinement groups is striking (14.92 days vs. 5.16 days) (Table 3). This discrepancy is particularly noteworthy in patients with hip fractures, who usually have convalescence periods that prolong the overall mean stay, although during the confinement and pandemic period the average stay in these cases reduced by 54% (15.35 days vs. 7.02) (Table 4), which is explained not only by the social pressure of fear of contagion during their admission and social responsibility due to the significant increase in patients, both locally and globally, but also by the implementation of measures by our centre. In this regard, early discharge was encouraged during the quarantine period, approved centres were set up and communication with primary care increased to free up hospital beds should there be an increase in COVID-19 cases.
Furthermore, in this period we observed greater general involvement of the relatives of hip fracture patients in their early discharge and subsequent care at home, two people (4%) being discharged in under 24 h following surgery, 15 (35%) in the first 48 h and 22 (51%) within 72 h. We have found no other study in the literature analysing postoperative stay in this group of patients during the pandemic stage versus a control period.
The main limitations of this study are its retrospective, single-centre nature and that it analyses the impact of COVID-19 in one of the least affected regions of Spain. However, a strength of the study is that it offers an unprecedented description of the effect of confinement, state of alarm and social unrest in the context of a global pandemic.
ConclusionsBased on the results of our study, the period of forced confinement due to the COVID-19 pandemic has resulted in a marked decrease in the total number of fractures admitted to the trauma department of a tertiary hospital. However, the total number of osteoporotic hip fractures seen for surgical treatment did not vary (as they almost always occurred at home) and an abnormally high number of these injuries were recorded at home in patients under 55 years of age. The average postoperative and overall length of stay have decreased significantly for many reasons, perhaps the most relevant being the greater availability of operating theatres and the greater involvement of relatives and patients in recovery at home, although further scientific analysis would be needed to confirm the influence of these factors in reducing length of hospital stay.
Level of evidenceLevel of evidence III (historical cohort).
FundingThis paper has received no funding of any type.
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: González-Martín D, Álvarez-De la Cruz J, Martín-Vélez P, Boluda-Mengod J, Pais-Brito JL, Herrera-Pérez M. Análisis cuantitativo y cualitativo de la influencia del confinamiento por COVID-19 en los pacientes con fractura ingresados en un servicio de traumatología en un hospital de tercer nivel. Rev Esp Cir Ortop Traumatol. 2021;65:374–381.
