



The overestimation by physicians of the risk of a lawsuit has, among other consequences, the stepped-up of defensive medicine. To analyse the characteristics of medical liability rulings in Spain in public health care in the specialties of cardiology and cardiovascular surgery.
Materials and methodsCross-sectional observational study analysing the rulings handed down in the contentious-administrative jurisdiction by the High Courts of Justice in the period 2008–2020, in the specialties of cardiology and cardiovascular surgery. The variables were administrative, clinical, judicial, and compensatory.
ResultsA total of 1015 rulings were analysed; 47 (4.63%) involved to the specialties of cardiology and cardiovascular surgery. Both obtained similar frequency percentages, cardiology 22 (2.2%) and cardiovascular surgery 25 (2.5%). A total of 74.1% of the rulings were dismissed in the first instance and 75% in the second instance. The 2 grounds for finding against the defendent were loss of chance 6 (42.85%) and diagnostic and/or therapeutic malpractice 5 (35.71%). Damages were usually claimed: death 21 (44.68%) and sequelae 26 (55.32%). The median award was 30 000 euros.
ConclusionsThe low frequency of claims in cardiology and cardiovascular surgery indicates that these are "low risk" specialties for litigation. The vast majority of the rulings are, moreover, dismissive of the patients' claims. The data help to structure the role of lawsuits and to increase professionals' knowledge of the medical–legal dimension of health care.
La sobrestimación por los facultativos del riesgo a una demanda judicial tiene, entre otras consecuencias, la intensificación de la medicina defensiva. El objetivo del trabajo fue analizar las características de las sentencias sobre responsabilidad médica en España en la asistencia sanitaria pública en las especialidades de cardiología y cirugía cardiovascular.
Material y métodosEstudio observacional transversal cuyo objetivo fue analizar las sentencias dictadas en la jurisdicción contencioso-administrativa por los Tribunales Superiores de Justicia en el período 2008-2020, en las especialidades de cardiología y cirugía cardiovascular. Las variables fueron administrativas, clínicas, judiciales e indemnizatorias.
ResultadosSe analizaron 1015 sentencias, de las cuales 47 (4,63%) se refirieron a las especialidades de cardiología y cirugía cardiovascular. Ambas obtuvieron porcentajes de frecuencia similares, cardiología 22 (2,16%) y cirugía cardiovascular 25 (2,46%). El 74,1% de las sentencias fueron desestimatorias en primera instancia y el 75% en segunda instancia. Los dos motivos de sentencia estimatoria más frecuentes fueron la pérdida de oportunidad 6 (42,85%) y la mala praxis diagnóstica y/o terapéutica 5 (35,71%). Los daños reclamados fueron: fallecimiento 21 (44,68%) y secuelas 26 (55,32%). La mediana de las indemnizaciones fue 30.000 euros.
ConclusionesLa baja frecuencia de las demandas en cardiología y cirugía cardiovascular indica que se trata de especialidades de “bajo riesgo” de litigiosidad. La inmensa mayoría de las sentencias son, además, desestimatorias de la pretensión de los pacientes. Los datos contribuyen a estructurar el papel de las demandas judiciales y a aumentar el conocimiento de los profesionales en la dimensión médico-legal de la asistencia sanitaria.
Medical liability has traditionally been a major concern for doctors. Within the international context, there is now debate about future claims for damages deriving from the COVID-19 pandemic.1 This concern about liability is also felt within governments and health services. Thus, one of the aspects usually taken into account is the expense associated with litigation, as this has increased in recent years.2,3 Given the increase in the number of lawsuits over recent years and the possibility of future claims due to the COVID-19 pandemic, it is necessary to underline that the Spanish context differs from the international one in several ways, including differences in the medical and legal systems here. This is why these circumstances are not thought likely to arise in Spain.
Given the above considerations, the medical speciality in question is one factor that influences the probability of being involved in a lawsuit.4 According to international studies, 8.6% of specialist cardiologists and 18.9% of cardio-thoracic surgery specialists are subjected to a lawsuit for liability every year. These figures are higher than the average corresponding to doctors in general, which stands at 7.4%.5 One result of the possibility that a doctor will have to face a lawsuit is the fear of being subjected to judicial processes, which leads to the phenomenon known as defensive medicine. This practice refers to requesting unnecessary diagnostic tests and treatments to protect oneself against a lawsuit (positive defensive medicine). Negative defensive medicine also exists, although it is harder to study, and it is based on either avoiding or refusing to treat high-risk patients, with the same aim.6
Within the context of the specialities which treat patients with cardiovascular diseases (cardiology and cardiovascular surgery) in the public health system, medical negligence in Spain has rarely been studied.
Cardiovascular diseases have been described as a worldwide pandemic.7 It is estimated that in 2015, the prevalence of cardiovascular diseases accounted for 422 million deaths in the whole world. Furthermore, the loss of years of life, the fall in quality of life, and the direct and indirect costs which arise due to these diseases are, according to the experts, unacceptable.8 We therefore consider it to be highly important to study the negligence within the specialities that are most specifically dedicated to treating patients with cardiovascular diseases. This work therefore aims to discover the characteristics of sentences due to liability in the specialities of cardiology and cardiovascular surgery in Spain. We believe that better knowledge and understanding of “cardio-judicial” epidemiology may help to contextualise the perceived risk of lawsuits among the professionals working in these specialities. At the same time, professionals will have a tool to try to reduce their fear that their cardiological practice will be subjected to judicial criteria.
MethodsThis is a cross-sectional observational study of the sentences for medical liability in the Higher Courts of Justice (Courts for Cases against the State) in Spain, pronounced from January 2008 to August 2020. Supreme Court sentences are excluded, as access to appeal there is extraordinarily restricted, so that including them would give rise to clear distortions in the final results. Criminal jurisdiction is also excluded, as this covers actions or omissions which constitute a crime. We also exclude civil jurisdiction, as this basically covers private medical care.
In terms of methodology, first and second instance sentences are included. In this point, it is necessary to take into account the fact that depending on the case, the Higher Courts of Justice may pass sentence in a first and unique instance, or in a second instance when the case has been settled beforehand by a lower court (a Court for Cases against the State). The variability of one or the other case depends on the amount claimed and the administrative medical body which is competent to resolve the previous claim. It also has to be pointed out that, in lawsuits for liability in the context of the public healthcare system, only the corresponding medical administration can be sued, as the professional involved in the case cannot be sued directly.
Sentences were analysed using the CENDOJ (Judicial Documentation Centre) public database. The key term that was searched for was medical liability, and a first group of 11 767 sentences was obtained.
The variables studied and collected in annual data files are classified under 4 headings: (a) administrative: instance, appellant; (b) clinical: patient age, field of medical intervention, speciality involved; (c) judicial: damage claimed, reason for the sentence and ruling; (d) amount of compensation.
The sample size was obtained using version 7.12 of the Granmo programme. Given that there are no previous data on the prevalence of sentences, an estimated proportion was selected of P = .50, with a 95% confidence level and a precision of 5%, with the result of at least 350 sentences. To increase the reliability of the data, it was decided to broaden the sample up to 1015 sentences, applying systematic sampling with analysis of 1 of every 8 sentences. There were 3 inclusion criteria: clinical motivation of the judicial ruling, consequences for the patient, and the amount of compensation. The following were excluded: (i) sentences that solely deny a claim due to formal considerations (such as expiry of the period for claiming); (ii) sentences in which more than one speciality is involved; (iii) sentences that include claims that only apply to the insurance company; (iv) sentences that are unconnected with the aim of this study.
Descriptive statistics were applied as a whole and separately depending on the specialities under study. Categorical variables are shown as absolute values, percentages, and confidence intervals of 95%, while quantitative variables are shown by the median and interquartile range (IQR). For quantitative variables, the type of distribution was checked beforehand using the Kolmogorov–Smirnov z-test, and the chi-squared test, a contingency table or the Student’s t-test were used to compare qualitative data, depending on which was applicable. The Mann–Whitney U-test or the Kruskal–Wallis test were used to compare quantitative variables with qualitative ones, as necessary. P values < .05 are considered significant. Data were analysed using version 24 of the IBM SPSS Statistics programme (Python License 2.7.6. and 3.4.3.)
ResultsOf the 1015, the cardiology and cardiovascular surgery specialities were found to have been involved in 47 cases (4.63%; CI 3.42–6.11). 31 cases were obtained in the first instance (65.95%; CI 50.68–79.13) and 16 were obtained in the second instance (34.04%; CI 20.86–49.31). In the case of the second instance, 12 cases were found where the appellant was the patient and/or the family (75%; CI 47.62–92.73) while in 4 cases the appellant was the health service and/or the insurer (25%; CI 7.26–52.37).
Regarding the clinical variables, the majority of the patients were adults, with 46 cases (97.87%; CI 88.70–99.94) and only 1 case of a minor (2.21%; CI 0.05–11.29). All of the sentences referred to incidents within a hospital context, at 47 cases (100%). The speciality of cardiology was implicated in 22 cases (2.2%; CI 1.36–3.26) and the speciality of cardiovascular surgery was implicated in 25 cases (2.5%; CI 1.60–3.61). Table 1 shows the administrative and clinical variables, differentiating between both of the specialities studied.
Descriptive analysis of administrative and clinical variables according to the speciality studied.
| Administrative variables | Cardiology | CV.S. | Cardiology | CV.S. |
|---|---|---|---|---|
| N (%) | N (%) | CI 95% | CI 95% | |
| Instance | ||||
| -First | 13 (59.10) | 18 (72) | [36.35–79.29] | [50.61–87.92] |
| -Second | 9 (40.90) | 7 (28) | [20.70–63.64] | [12.07–49.38] |
| Appellant | ||||
| -Patient and/or family | 6 (66.67) | 6 (85.71) | [29.93–92.51] | [42.12–99.63] |
| -H.S. and/or insurer | 3 (33.33) | 1 (14.29) | [7.48–70.07] | [0.36–57.87] |
| Clinical variables | Cardiology | CV.S. | Cardiology | CV.S. |
| N (%) | N (%) | CI 95% | CI 95% | |
| -Adult | 21 (95.46) | 25 (100) | [77.15–99.88] | |
| -Minor | 1 (4.54) | 0 (0) | [0.11–22.84] | |
| Context | ||||
| -Hospital | 22 (100) | 25 (100) | ||
| -Outside hospital | 0 (0) | 0 (0) | ||
CV.S.: cardiovascular surgery; H.S.: health service.
Of the judicial variables, the damages claimed for the most often were sequelae, in 26 cases (55.32%; CI 40.11–69.82) and death in 21 cases (44.68%; CI 30.17–59.88).
Of the 47 sentences, infraction of good clinical practice (lex artis) was found in 14 cases (29.78%; CI 17.34–44.90) due to the following causes: lost opportunity in 6 cases (42.85%; CI 17.66–71.13), poor praxis in diagnosis and/or treatment, with 5 cases (35.71%; CI 12.76–64.86), a lack of information in 1 case (7.14%; CI 0.18–33.86), disproportionate harm in 1 case (7.14%; CI 0.18–33.86) and pain and suffering in 1 case (7.14%; CI 0.18–33.86).
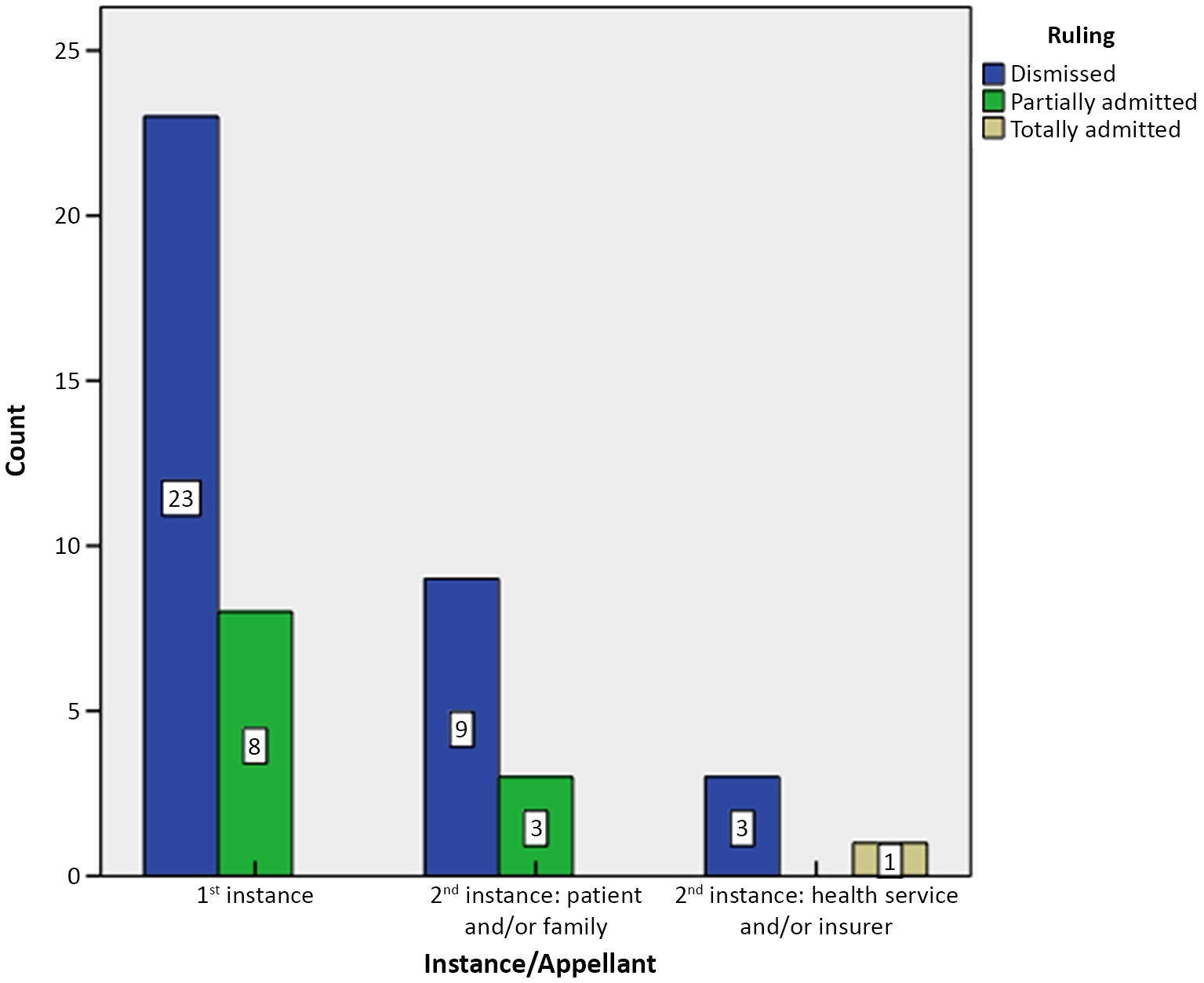
In the variable for rulings in the first instance (31), 23 cases were dismissed (74.19%; CI 55.38–88.14) and 8 cases were partially admitted (25.81%; CI 11.85–44.61). No complete acceptance was found in any case. In the second instance (16), when the appellant was the patient and/or the family (12), 9 cases were dismissed (75%; CI 42.81–94.51) and 3 cases were partially admitted (25%; CI 5.48–57.19). When the appellant was the health service and/or the insurer (4), 3 cases were dismissed (75%; CI 19.41–99.36) and 1 case was totally admitted (25%; CI 0.63–80.58) (Fig. 1). Table 2 shows the judicial variables, differentiating between the specialities that were studied.

Descriptive analysis of the judicial variables according to the speciality studied.
| Variables | Cardiology | CV.S. | Cardiology | CV.S. |
|---|---|---|---|---|
| N (%) | N (%) | CI 95% | CI 95% | |
| Damages claimed | ||||
| Death | 12 (54.55) | 9 (36) | [32.21–75.61] | [17.97–57.47] |
| Sequelae | 10 (45.45) | 16 (64) | [24.38–67.79] | [42.52–82.02] |
| Reasons for the sentences | ||||
| Missed opportunity | 4 (28.57) | 2 (14.29) | [8.38–58.10] | [1.77–42.81] |
| Poor praxis in diagnosis and/or treatment | 2 (14.29) | 3 (21.42) | [1.77–42.81] | [4.65–50.80] |
| Lack of information | 1 (7.14) | 1 (7.14) | [0.18–33.86] | [0.18–33.86] |
| Disproportionate harm | 1 (7.14) | [0.18–33.86] | ||
| Ruling | ||||
| 1st Instance | ||||
| -Dismissed | 9 (69.23) | 14 (77.78) | [38.57–90.90] | [52.36–93.59] |
| -Partially admitted | 4 (30.76) | 4 (22.22) | [9.09–61.42] | [6.40–47.63] |
| -Totally admitted | 0 | 0 | ||
| 2nd Instance (according to appellant) | ||||
| Patient and/or family | ||||
| -Dismissed | 5 (41.68) | 4 (33.33) | [15.16–72.33] | [9.92–65.1] |
| -Partially admitted | 1 (8.33) | 2 (16.66) | [0.21–38.48] | [2.09–48.41] |
| -Totally admitted | 0 | 0 | ||
| Health service and /or insurer | ||||
| -Dismissed | 2 (50) | 1 (25) | [6.75–93.24] | [0.63–80.59] |
| -Partially admitted | 0 | 0 | ||
| -Totally admitted | 1 (25) | 0 | [0.63–80.59] | |
CV.S.: cardiovascular surgery.
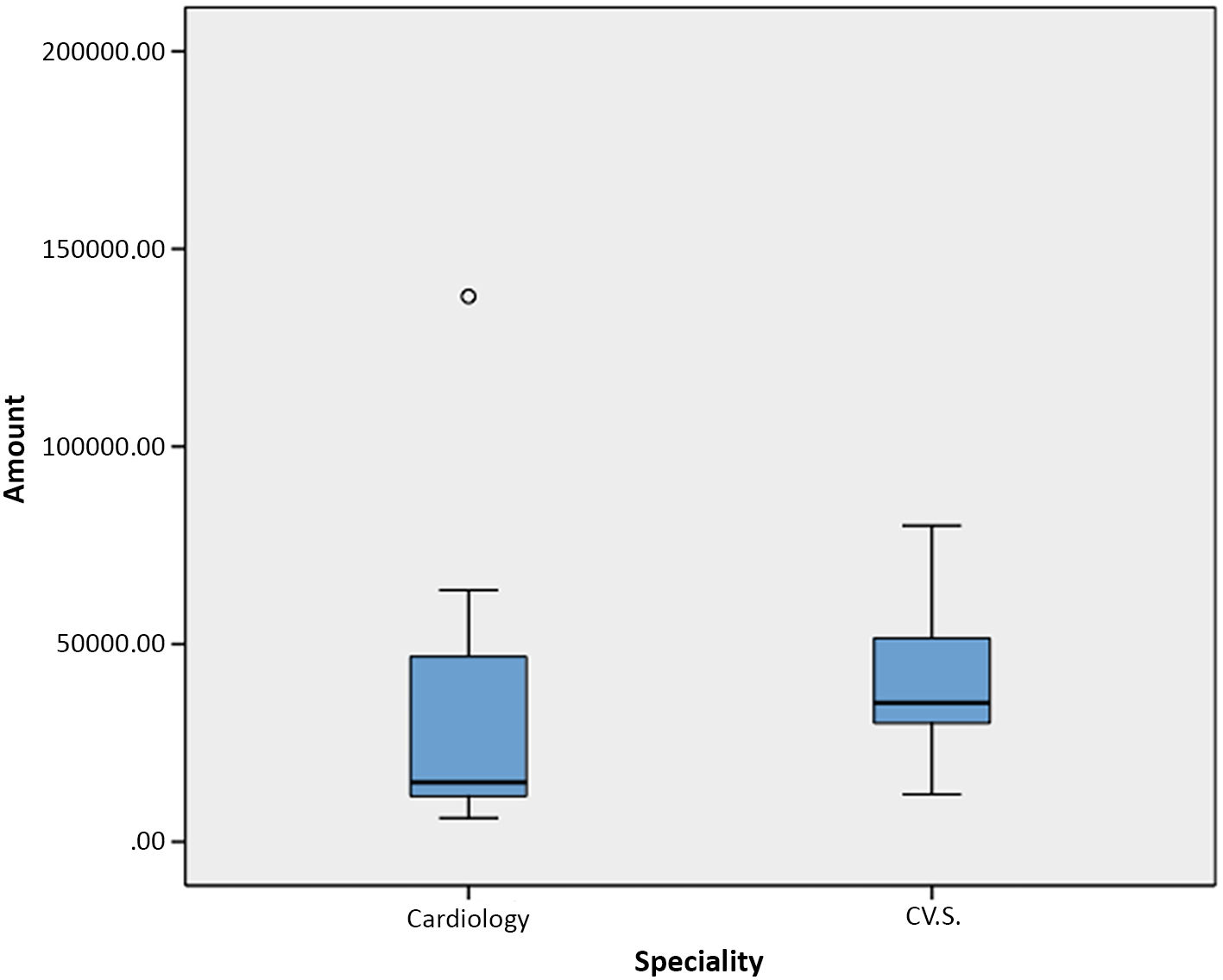
The median sum paid in compensation was 30 000 euros (IQR 132 000), with a minimum of 6000 euros and a maximum of 138 000 euros. The median sum for the speciality of cardiology was 15 000 euros (IQR 55 667.90), with a minimum of 6000 euros and a maximum of 138 000 euros. The median sum for the speciality of cardiovascular surgery was 35 140.64 euros (IQR 24 000), with a minimum of 11 983.48 euros and a maximum of 80 000 euros (Fig. 2). The median sum corresponding to lost opportunity was 36 271.83 euros (IQR 60 250.93) and for poor praxis in diagnosis and/or treatment it was 30 000 euros (IQR 75 008.26). No statistically significant differences were found between the median sums in the 2 most common reasons for sentencing (P = .946).

Regarding the damages claimed, a median sum of 42 070.32 euros (IQR 67 2450.93) was paid in cases of death, with a minimum of 15 000 euros and a maximum of 138,000 euros. A median sum of 30 000 euros (IQR 39 004.13) was paid in cases of sequelae, with a minimum of 6000 euros and a maximum of 80 000 euros. No statistically significant differences were found (P = 282).
DiscussionThe claims for liability in the specialities of cardiology and cardiovascular surgery have 3 main characteristics: (a) they arise in cases of adult patients; (b) they occur in a hospital context; and (c) the immense majority are dismissed; i.e., rulings are unfavourable for patients and/or their families.
The frequency of claims for the speciality of cardiology (2.2%) indicates that it is a speciality with a low level of judicial risk. Although this result agrees with those in the international literature, it should be underlined that the methodology, sources, health services, and legal systems all differ widely. In the case of Canada, after analysing 60 598 cases, it was found that a cardiologist was only implicated in 0.6% of cases.9 A study in the U.S.A. that analysed 230 624 claims found that cardiologists were implicated in 1.8% of them.10 A Spanish study of second instance sentences found that cardiologists were implicated in 1.63% of the sentences analised.11 Another study in Catalonia obtained similar findings: claims from 2000 to 2018 were analysed, of which 2.02% corresponded to cardiology and 0.97% corresponded to cardiovascular surgery.12
The frequency for cardiovascular surgery is similar to that for cardiology, with 2.5% of cases. This finding does not agree with those of international studies, as it is widely accepted that this is a high-risk speciality.13 Nevertheless, it does agree with the findings of other studies in Spain. One such study which analysed 2817 sentences found that cardiovascular vascular was not among the specialities most subjected to claims.14 Another study of 6952 cases found that 1.3% corresponded to vascular surgery.15 It therefore seems that both specialities in Spain are not among those which are most subject to claims, so that here they can be classified are specialities with a low level of litigation.
The fundamental finding of this study is that 74.1% of first instance sentences are dismissals. In the second instance, 75% of cases are dismissed if the appellant is the patient and/or their family. It is striking that no sentence completely admits the claim by a patient and/or their family. Our findings here agree with those of other studies, which find that 13.6% of the claims against cardiologists are admitted.16 They are also similar to those of another study in Spain which used a different methodology, which found that sentences consisted of dismissal in 69% of cases.11 In the case of cardiovascular surgeons, another study of negligence in 140 cases found that 27.9% of cases were found in favour of the plaintiff.17
The fact that the majority of sentences are favourable for the health administration supports our idea that defensive medicine is a responses that is not only reprehensible, as it is also exaggerated. It is important to underline that merely committing an error is not a sufficient cause for liability, as this is based on the duty to pay compensation due to an error caused by negligence. However, even if a claim is made implicating the specialities that were studied, the majority of rulings favour the public administration.
Although defensive medicine is widely used around the world, it is hard to discover the degree to which it is prevalent. The studies undertaken of this are fundamentally based on surveys of the professionals themselves, who recorded levels of defensive medicine of up to 93% in 1 study in the United States.18 Another study based on a survey in Italy found that defensive practices affected 58.8% of medical interventions.19 A study recently published in Spain on Hospital Emergency Departments found that 89.8% of professionals stated that they carried out diagnostic tests that may be unnecessary, and 63% prolonged patient stays in the Emergency Department.20 In spite of these data, we consider the fact that undergoing a judicial proceeding has a major psychological impact on professionals,21 and that this may be sufficiently negative to lead them to even abandon their profession.22
The most common reasons for sentencing are lost opportunity (42.85%) and poor praxis in diagnosis or treatment (35.71%). Evaluation in cases of lost opportunity is based on what would have happened if professionals had acted diligently.23 The criterion of lost opportunity implies a reduction the amount of compensation in situations where precisely the probability that the harmful event was a condicio sine qua non does not surpass the threshold of certainty. In Anglo-Saxon law, the doctrine of lost opportunity applies when the probabilities of causality are less than 50% (a “less-than-even-chance”). Nevertheless, in European legal culture it applies when the said probabilities are less than the threshold of 80%.24 The possible real benefit that the patient did not obtain due to delay, diagnostic error, a lack of diagnosis or treatment, lack of monitoring or information is therefore evaluated.25
Although our findings are similar to those in the current tendency, we found few sentences based on infraction of the lex artis (14 cases). It would therefore be necessary to confirm these findings by broader studies.
Our data show that the numbers of claims for death and sequelae are practically the same. Few studies cover this question for both of the specialities in question. We believe that the fact that in curative medicine obligations apply to measures and not to results should be underlined. That is, no professional can be subjected to demand which go beyond what is considered to be the state-of-the-art and the available resources, which is known as lex artis ad hoc.26 Even when the result is death, if actions have been according to lex artis, there can be no causes for liability.
The sums paid in compensation in the cases that were admitted amount to a median of 30 000 euros, and no statistically significant difference was found in this respect between both specialities. The median was 15 000 euros in the case of cardiology, while in cardiovascular surgery it was 35 140.64 euros. Our data can be compared to those of very few other studies, given that our analysis is restricted to the public health system and that there are major differences with the judicial context in the United States, where the majority of studies were conducted. Nevertheless, it is possible to observe that the above sums are very much lower than the average compensation paid in the U.S.A. from 2009 to 2014 in cardiology, 368 350 dollars.27 An analysis of the claims for negligence against cardiovascular surgeons in the U.S.A. found that the average compensation amounted to 1 830 000 dollars.28 In Spain, an analysis of the second-instance sentences in cardiology by the Provincial, Higher and Supreme Courts (the civil and criminal jurisdictions together with cases against the state) found sums that were almost always higher than 60 000 euros.11 A study in Catalonia analysed 5246 claims, 72 of which corresponded to cardiology and 65 to cardiovascular surgery. The median amounts paid in compensation were 153 249 euros in cardiology and 18 000 euros in cardiovascular surgery.29
The main limitation of this study is its low number of sentences due to infraction of the lex artis. This is why it should be corroborated by a study with a higher number of positive sentences. Another limitation is that the study centres on judicial processes, as it analyses sentences within the context of the Higher Courts of Justice in the Court of Cases against the Government, so that it excludes claims for liability and, when applicable, cases which were resolved out-of-court. Lastly, this study does not include civil and criminal cases: i.e., the results obtained are restricted to public administration medical liability.
ConclusionsThe results of this study point to 2 fundamental conclusions. The first conclusion is that the vast majority of claims for medical liability in the field of cardiology and cardiovascular surgery are dismissed. The importance of this finding lies on the one hand in the fact that the public administration was unaware of this datum to date, and this was also the case for both of the specialities which cover cardiovascular diseases.
The second conclusion leads us to state that, in spite of the high level of technology use in cardiology and cardiovascular surgery, and the treatment of increasingly complex cases, both specialities could be described as being of low judicial risk in Spain.
We believe that these findings may help to increase professionals’ awareness of certain medical and legal aspects that are intrinsic to their speciality. Furthermore, the findings contribute to opening up new lines of research, as is already the case in other countries, which would make it possible to implement measures that reduce the exaggerated perception of the risk of judicial lawsuits. This could thereby reduce the tendency to practice defensive medicine and, in turn, the negative consequences of this in professionals.
Key pointsWhat is known?Medical liability in Spain has hardly been studied. Over-estimation of professionals’ legal risk leads to an increase in the number of tests and treatments, or to avoiding high-risk patients and the consequent possibility of lawsuits, which is known as defensive medicine. The latter has highly negative consequences, and using it is no protection against claims. Internationally, the specialities of cardiology and cardiovascular surgery are considered to be medium- or high risk in terms of lawsuits.
What it contributes?For the first time in Spain, this research shows the characteristics of the claims made for medical liability in the specialities which centre on treating patients with cardiovascular diseases. The majority of sentences are in favour of the public administration. The infrequent number of cases detected in cardiology and cardiovascular surgery means that they can be considered to be specialities with a low risk of claims.
This study offers fundamental medical–legal tools for professionals. Increased knowledge of these questions may help to mitigate the fear of lawsuits and thereby reduce the use of defensive medicine, as it leads to highly negative consequences.
FinancingThis study received no specific grants from public, commercial or not-for-profit agencies.
Please cite this article as: Hernández-Herrero M, Cayón-De Las Cuevas J. Judicialización en cardiología y cirugía cardiovascular: estudio observacional transversal en materia de responsabilidad patrimonial en la sanidad pública española. Revista Española de Medicina Legal. 2022. https://doi.org/10.1016/j.remle.2022.10.001