


Erectile dysfunction incidence is about 19–26 cases for every 1000 men/year, requiring about 20,000 penile implants/year. There is high demand for information on the part of patients, however, there is a lack of evidence about the sources of information prior to penile implant and the figure of the Expert Patient (EP) has never been described in this area.
AimsTo evaluate the sources of information used by candidates for penile implant as well as to describe the role of the EP as an information source.
MethodsPilot study of candidates for penile prosthesis. Patients already implanted attending for exchange or reallocation surgery were excluded. Each patient had an interview with an EP, and commercial documentation was given. Each source of information was evaluated in a face-to-face interview. SPSS™ version 20.0 was used.
Main outcome measuresThe EP was evaluated by the International Index of Erectile Function, the Generalized Anxiety Disorder 7 questionnaire, and the Erectile Dysfunction Inventory of Treatment Satisfaction. Each source of information was evaluated by a non-validated 6-section questionnaire.
ResultsTen patients were included. Mean age was 60±10.3 years. Medical interview with the urologist resulted in a global value and truthfulness score of 9.2±.9 and 9.8±.4, respectively. Commercial information had a global score of 8.5±.9 and a truthfulness score of 8.6±.6, while the internet had 6.8±.8 points for global value and 7.2±1 for truthfulness. The global score of the EP was 8.7±1.2 points and their veracity scored 9.6±.5 points.
ConclusionsThe urologist remains the main source of information for patients with erectile dysfunction candidates for penile prosthesis implant. However, the EP is an alternative and could be a key pillar in presurgical counselling.
El paciente experto (PE) es una nueva fuente que brinda información a otros pacientes, basada en su experiencia personal en un proceso de salud determinado. La figura del PE está más desarrollada dentro de enfermedades crónicas, aunque, sin embargo, no está descrito su papel en pacientes con disfunción eréctil (DE) candidatos a prótesis de pene (PP).
ObjetivosNuestro objetivo principal es analizar la valoración del PE como fuente de información por parte de pacientes candidatos a PP. Secundariamente, analizaremos otras fuentes de información consultadas.
Material y métodosEstudio prospectivo de pacientes candidatos a PP. Cada paciente se entrevistó con el PE (paciente de 58 años, portador de prótesis de pene hidráulica de 3 componentes desde hace 24 meses por DE post-prostatectomía radical). A cada paciente se le entregó, además, información aportada por las casas comerciales. El urólogo que realizó el implante, el PE, la información comercial y la información obtenida en Internet sobre las prótesis de pene fueron evaluados como fuentes de información mediante un cuestionario no validado, estructurado en 6 apartados, aplicado en una entrevista cara a cara por un único médico diferente a su médico tratante.
ResultadosSe incluyeron 10 pacientes con edad media de 60±10,3 años. La entrevista médica con el urólogo obtuvo una puntuación global de 9,2±0,9. La información comercial obtuvo una puntuación global de 8,5±0,9 y una puntuación de veracidad de 8,6±0,6, mientras que Internet obtuvo 6,8±0,8 puntos de puntuación global y una veracidad de 7,2±1. El paciente experto fue valorado globalmente con 8,7±1,2 puntos y una veracidad de 9,6±0,5 puntos.
ConclusionesEl urólogo es considerado como la mejor fuente de información por parte de pacientes con DE previo a una prótesis de pene. Sin embargo, el PE representa una alternativa y puede constituir un soporte adicional previo a la cirugía.
Erectile dysfunction (ED) has a big impact on quality of life both for patients and their partners, and its treatment has radically evolved from the deep dorsal vein ligation used at the end of the XIX century or testicular implants performed at the beginning of the XX century. Nowadays, ED surgical treatment is strongly based in penile prosthesis implantation, representing the third line treatment for this condition.1
In Europe ED prevalence is about 19% of the population aged 30–80, with an incidence between 19 and 26 cases for every 1000 men per year. Besides, one out of four patients consulting for ED is under 40 years old, and among those, half of them suffer from severe ED.2 It is estimated that in the United States 6500 out of 100,000 patients consulting do it because of their ED, reaching the amount of 20,000 penile implants per year.3
That important incidence determines a huge demand of information about ED and the several options available to treat it, not only through the general practitioner or the urologist, but through medical websites, forums or platforms like Youtube or Twitter. In fact, up to 94% of patients suffering from ED has taken advice from more than one source of information, being the doctors the ones who are more frequently consulted (54%), but almost evenly matched with the internet (52%).4 However, there is few data available nowadays about the main sources of information consulted previously to penile implant.
The term expert patient (EP) first introduced in 2001 by the chief medical officer for England has been applied and deeply studied in the field of chronic diseases. Thus, the EP is the one with experience and knowledge about his own condition that makes him able to detect risk situations and skilled enough to self-management. Such concept has evolved and nowadays EP is believed to have a key role in the communication and transfer of information to other patients suffering from the same disease.5 This scenario has never been described in the field of the penile prosthesis surgery.
Our aim is to evaluate the different sources of information used by the candidates to a penile implant as well as to describe the role of EP as a reliable source of information.
MethodsWe conducted a pilot study where candidates to penile prosthesis followed up at Urology Outpatient Clinic in our Centre were included. Patients who were already implanted attending for an exchange or reallocation surgery were excluded.
In the office, the urologist explained to candidates the process of penile implant surgery, the different types of penile prostheses, expected benefits, potential surgical complications, postoperative care and recovery, as well as long-term complications. Besides, the urologist delivered written and audiovisual material to every patient provided by both companies Boston Scientific™ and Coloplast™ with information about the prosthesis and procedure. Likewise, every patient was offered the opportunity to meet face to face with the EP at the Hospital in the presence of a physician different from their usual urologist. Objectives of the study and confidentiality of the data was clearly stated to all participants and every of them gave his consent to participate.
EP initial evaluation was performed using three validated questionnaires: International Index of Erectile Function (IIEF), Generalized Anxiety Disorder 7 (GAD-7) and Erectile Dysfunction Inventory of Treatment Satisfaction (EDITS).6–8
The meeting took place at our Hospital and patients had the chance to freely ask any question to the EP and comment whatever they wanted regarding the procedure of the prosthetic surgery, or subsequent controls.
Following this, an interview face to face with an interviewer was performed and, as no validated questionnaire for medical information sources evaluation was found, we designed a structured 6-section questionnaire ad hoc. First section recorded demographic data, educational level, comorbidity, internet availability at home and time spent browsing per day. Section two to five conform the intra-source data, containing the information linked to each source separately (Urologist, companies’ information, internet and EP, consecutively). Items recorded for each source were: time used globally seeking for information, usefulness of the source (yes/no), ability to solve doubts (yes/no) and the fact of making reference to both benefits and complications of the procedure (yes/no). Finally, global value and truthfulness of each source were evaluated using two separate scales ranging from 0 to 10, where 0 represents poor and 10 represents excellent.
Inter-source evaluation constitutes section six, where four questions are proposed: (1) which source did you find the most useful to get informed about the procedure? (2) Which source helped you the most to decide to get involved in the procedure? (3) Which source made you feel more comfortable with? And (4) globally, which source do you value the most?
The study was conducted following the ethical principles outlined in the Helsinki Declaration of 1975 revised in 1983.
Descriptive statistics using SPSS™ version 20.0 was implemented to describe the study group and calculate proportions, means and standard deviations (SDs).
Main outcomes measuresEP prior evaluation was performed using the International Index of Erectile Function (IIEF) which is a 15-item questionnaire that assesses domains of male sexual function that include erectile function, orgasmic function, sexual desire, intercourse satisfaction and overall satisfaction; the Generalized Anxiety Disorder 7 (GAD-7) questionnaire which has 7 items each of which scores between 0 and 3 according to the frequency of symptoms (Generalized Anxiety Disorder is diagnosed if score is over 8 points); and the Erectile Dysfunction Inventory of Treatment Satisfaction (EDITS) which is a 11-item questionnaire, which answers range from 0 (very dissatisfied) to 4 (very satisfied). The EDITS index is calculated by multiplying the mean score of all 11 items by 25, which yields a total score ranging from 0 (lowest satisfaction) to 100 (highest satisfaction).
Each source of information was evaluated by a non-validated 6-section questionnaire. Intra-source evaluation was made by four questions with dichotomous answers (yes/no), global value and truthfulness of each source were evaluated using two separate scales ranging from 0 to 10, where 0 represents poor and 10 represents excellent. Finally inter-source evaluation was made by four questions as previously mentioned.
ResultsA total of ten patients were included, which represents the 100% of the total group invited to participate. Mean age of the cohort was 60±10.3 years. Four patients had primary educational level and six had secondary educational level. EP was 58 years old and an IIEF score of 30 points (no ED), GAD-7 of two points (no anxiety) and EDITS score of 100 (highly satisfied).
A total of 80% of patients had Internet available at home (except patients 4 and 7) and the mean time spent browsing daily was 88.1±50.9min.
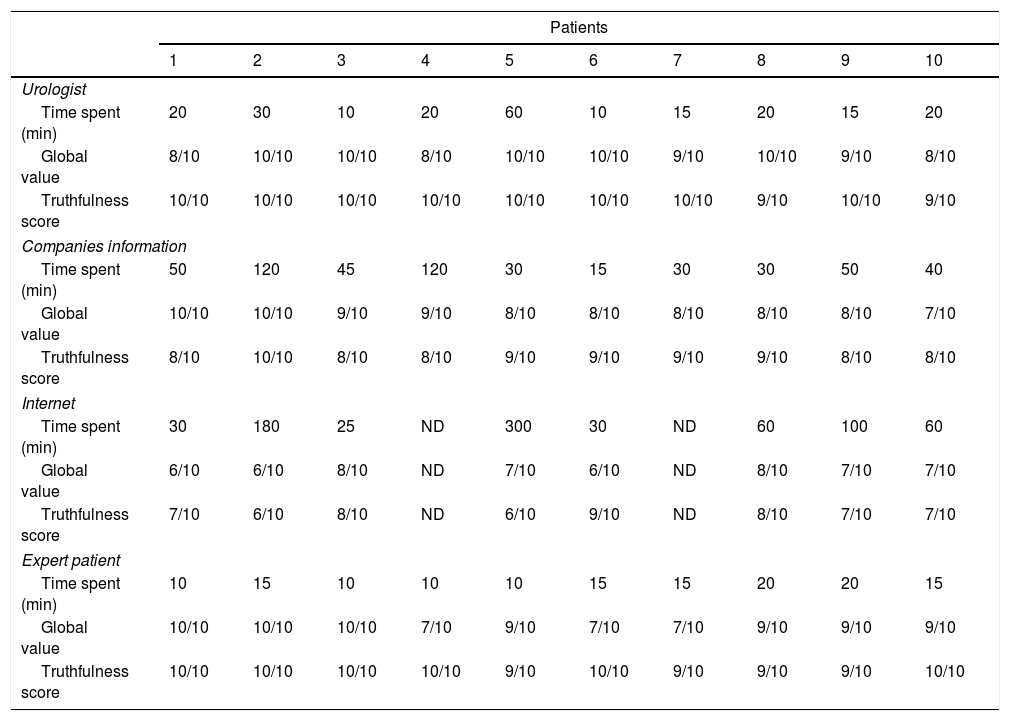
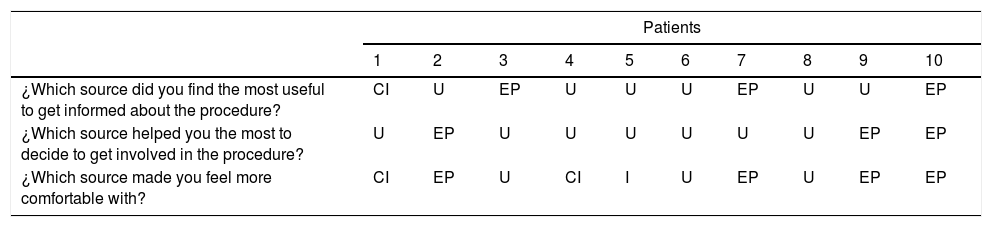
Intra and inter-source evaluation (answers to sections two to six) are shown in Tables 1 and 2 respectively.
Time spent, global value and truthfulness scores for each source of information.
| Patients | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
| Urologist | ||||||||||
| Time spent (min) | 20 | 30 | 10 | 20 | 60 | 10 | 15 | 20 | 15 | 20 |
| Global value | 8/10 | 10/10 | 10/10 | 8/10 | 10/10 | 10/10 | 9/10 | 10/10 | 9/10 | 8/10 |
| Truthfulness score | 10/10 | 10/10 | 10/10 | 10/10 | 10/10 | 10/10 | 10/10 | 9/10 | 10/10 | 9/10 |
| Companies information | ||||||||||
| Time spent (min) | 50 | 120 | 45 | 120 | 30 | 15 | 30 | 30 | 50 | 40 |
| Global value | 10/10 | 10/10 | 9/10 | 9/10 | 8/10 | 8/10 | 8/10 | 8/10 | 8/10 | 7/10 |
| Truthfulness score | 8/10 | 10/10 | 8/10 | 8/10 | 9/10 | 9/10 | 9/10 | 9/10 | 8/10 | 8/10 |
| Internet | ||||||||||
| Time spent (min) | 30 | 180 | 25 | ND | 300 | 30 | ND | 60 | 100 | 60 |
| Global value | 6/10 | 6/10 | 8/10 | ND | 7/10 | 6/10 | ND | 8/10 | 7/10 | 7/10 |
| Truthfulness score | 7/10 | 6/10 | 8/10 | ND | 6/10 | 9/10 | ND | 8/10 | 7/10 | 7/10 |
| Expert patient | ||||||||||
| Time spent (min) | 10 | 15 | 10 | 10 | 10 | 15 | 15 | 20 | 20 | 15 |
| Global value | 10/10 | 10/10 | 10/10 | 7/10 | 9/10 | 7/10 | 7/10 | 9/10 | 9/10 | 9/10 |
| Truthfulness score | 10/10 | 10/10 | 10/10 | 10/10 | 9/10 | 10/10 | 9/10 | 9/10 | 9/10 | 10/10 |
Inter-source evaluation.
| Patients | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
| ¿Which source did you find the most useful to get informed about the procedure? | CI | U | EP | U | U | U | EP | U | U | EP |
| ¿Which source helped you the most to decide to get involved in the procedure? | U | EP | U | U | U | U | U | U | EP | EP |
| ¿Which source made you feel more comfortable with? | CI | EP | U | CI | I | U | EP | U | EP | EP |
ND: no data; U: urologist; EP: Expert patient; CI: Companies information; I: Internet.
Medical interview with the urologist lasted for 22±14.5min and reached a global value and truthfulness score of 9.2±0.9 and 9.8±0.4 respectively. About commercial information provided by the companies, patients invested on average 53±36.9min, giving a global value of 8.5±0.9 and a truthfulness score of 8.6±0.6. To seek information through the net 98.1±96.3.1min were spent by the patients given a global value of 6.8±0.8 and a truthfulness score of 7.2±1. Regarding to EP, interview lasted for 14±3.9minutes, and was globally valued with 8.7±1.2 points and its degree of reliability scored with 9.60±0.5 points.
DiscussionED is not only a physical limitation as it affects the psychosocial aspect and quality of life of both patients and sexual partners. European Guidelines from European Association of Urology include penile implant as third line of treatment for the ED.3
It has been described that penile prosthesis reaches the best results concerning erection grade and patient satisfaction,9 and the psychosexual support seems to have a crucial role for the reestablishment of both organic and erotic functions after the penile implant. This underscores the importance of given information, control of expectations and psychological aspect in terms to improve sexual life.10
In this sense, it is fair to recognize the increasing offer of medical information through several sources, specially, the internet. This fact facilitates our patients to come to the clinic with a huge amount of information about their conditions, diagnosis options and possible treatments. Fox et al. concluded that 72% of internet users have browsed medical information at least once, and 77% among them started browsing with tools like Google™, Bing™ o Yahoo™, maybe linking to websites managed by non-medical providers and containing inaccurate and potentially damaging information.11
When we focus in urology, several publications place the figure of urologist as the main source of information: on the one hand, 59% out of 200 patients evaluated by Davidson et al. after radical prostatectomy or brachytherapy because of localized prostate cancer; and on the other, 54% of ED patients studied by Zhang et al.4,12 Those findings correlate with ours, where the urologist was the most valuable source of information for the 80% of patients.
Regarding the internet, the use given by our patients (80%) is clearly higher than the 51% provided by Davidson et al.4 This difference could be explained by the fact of Davidson et al. publishing in year 2004 and we doing it now, with the wide diffusion the Internet has experienced.
Several series exist where written information was selected as the most valuable tool in more than half of the study groups, confronting our findings, where none of our patients selected the commercial information in the inter-source question. Surprisingly, this source obtained a high global score, close to the EP (8.7 points) and the urologist (9.2 points) in the intra-source evaluation. A strength point of the commercial information is the fact that was selected by two of our patients as the easiest way to consult, being one of both patients the one without Internet access at home. This might be explained by the fact of being a source with easy and wide access almost everywhere and every time, and presented in a more traditional fashion (triptychs, brochures and patient guidelines).
Other publications confront our results as the one by Buvat et al. with the 35% of their population consulting a doctor and only the 13.6% using the Internet, magazines or television as sources of information. It has to be explained that the study population was conformed of men and women with miscellaneous sexual pathologies (loss of libido, premature ejaculation, ED and absent sexual pleasure) and they asked about the very first source of information consulted. It seems logical that medical information, the Internet webs and the written information have been displaced by the sexual partner, which appears as the first source for the 52% of the consulted population.13
After our review, we have been unable to find any publication neither about the sources of information prior to penile implantation, nor about the figure of the EP as part of the options offered to those patients in clinics.
In our pilot study, every source of information was globally scored as satisfactory. Notwithstanding, when asked about truthfulness assigned to each source, urologists obtained the best score with only a difference of 0.2 points over the EP. The internet, meanwhile, in spite of being consulted by almost every patient in the study (except patients 4 and 7 because of no availability), was the worst scored with a global value and truthfulness of 6.8 and 7.2 points respectively.
Inter-source information concludes that the urologist is a cornerstone. Besides, EP was considered the most comfortable source by four patients and as the most valuable, useful and helpful source by three patients. These results agree with the impression perceived by the physician during the meeting between the EP and the patients. For example, despite of being two strangers, they interacted with trust and familiarity, they discussed doubts not only about the procedure and potential complications, but personal questions about their sexual partners and psychological aspects related to surgery, recovery period and lifestyle after the implantation. Some of them reached a close and empathetic environment which higher than the one established between physician and patient. We found that candidates felt really comfortable and got over that imaginary limit that unfortunately sometimes exists between us and the patients, despite the effort we made to avoid it. As a consequence of that, more personal questions previously considered taboo or inappropriate to pose to the urologist are now proposed, giving the EP a key role in the prosthetic pre-surgical assessment.
Those findings are reinforced in social media like Twitter, where profiles like @HealthUnlocked, @patientsco (Patients Know Best) or @patientslikeme promote the communication patient-to-patient with over 5000, 1000 and 29,000 followers, respectively.
To the best of our knowledge, this is the first report about the sources of information consulted by the candidates to penile implant. Besides, we described and evaluate the role of the EP in a new scenario where it has never been described before: penile prosthetic surgery.
Nevertheless, several limitations should be taken into account. First, as in all single-centre studies, the management of a given pathology may be influenced by the protocols, work habits, and resources of one particular hospital. Perhaps, other significant limitations are the small number of patients involved and the use of a non-validate questionnaire.
In the future, new lines of research should be developed to obtain more data on the sources of information consulted, the global value given to the sources after the implant and a new evaluation of the sources depending of patient groups like re-implantation, Peyronie's disease or sex change surgery, for example.
ConclusionsAccording to our results, the urologist constitutes the most valuable source of information for candidates to penile implant. Nevertheless, we have described, proposed and studied the figure of EP for our patients as an additional source with a good reception. We believe it might represent a key component in the prosthetic pre-surgical information plan.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of dataThe authors declare that no patient data appears in this article.
Right to privacy and informed consentThe authors declare that no patient data appears in this article.
Conflicts of interestsThere's no conflicts of interests in this study.