










Poor anteroposterior mandibular relations comprise the largest number of cases. In this group class II malocclusion is the most frequent. Orthodontists began using extraoral forces with modified Hawley retainers many years ago. Margolis realized that removable appliances combined with extraoral forces could not only serve as good containers, but be used as effective correction mechanisms. He called his appliance ACCO (AC acrylic, CO cervico occipital anchorage).
ObjectiveThe objectives of the case hereby presented were maxillary growth control and try to protrude the mandible.
Case presentationA 10 year-3 month-old female patient attended the Orthodontics Clinic at the Division of Postgraduate Studies and Research at the National Autonomous University of Mexico. She presented a skeletal class II due to mandibular retrusion and maxillary protrusion, a vertical growth pattern, excessive growth of the nasomaxillary complex and protrusive incisors.
TreatmentOrthopedic: ACCO with high traction and impact to retrude the maxilla and decrease vertical growth; with expansion screw (one turn a week). Headgear: nocturnal use and three to four hours in the afternoon. Active plate 24hours and the patient was told to remove it for eating. Orthodontic treatment: .022 Roth fixed appliances retention: bimaxillary appliance for nocturnal use.
ResultsAfter five months of ACCO use, cephalometric tracings were performed again and the following values were obtained: maxillomandibular relationship: ANB 5° (initial 11°), Wits 2mm (initial 3mm), Bimler overjet 9mm (initial 10mm) convexity 6mm (initial 11mm). Maxillary position: SNA 82° (initial 87°) mandibular position: SNB: 78° (initial 76°). Facial pattern: facial cone of 67° (61° initial dolichofacial). Vertical dimension: SN-mandibular 36.5° (initial 42°), FMA (Tweed) 35° (initial 43°), Goniac (Jarabak) 130° (initial 128°). Incisor Inclination: UpI/SN 114° (initial 117°), LowI/Mand remained the same (95°).
ConclusionsOrthopedics in conjunction with orthodontics harmonizes the maxilla and mandible and at the same time provides natural facial aesthetics, while maintaining proper functions: chewing, swallowing, phonation and breathing. It is vitally important to perform a timely diagnosis in order to intervene orthopedically, correct this kind of malocclusions and limit or prevent its severity.
Las malas relaciones mandibulares anteroposteriores comprenden el mayor número de casos. En este grupo, la maloclusión de clase II es la más frecuente. Los ortodoncistas comenzaron utilizando extraorales con contenedores de Hawley modificados hace muchos años. Margolis se dio cuenta que los aparatos removibles combinados con la fuerza extraoral podían no sólo servir como buenos contenedores, sino ser utilizados como efectivos mecanismos de corrección. Llamó a su aparato ACCO (AC acrílico, CO anclaje cervicooccipital).
ObjetivoLos objetivos óseos del caso fueron controlar el crecimiento maxilar y tratar de protruir la mandíbula.
Presentación del casoSe presenta en la Clínica de Ortodoncia de la División de Estudios de Postgrado e Investigación de la Universidad Nacional Autónoma de México paciente femenino de 10 años con 3 meses, clase II esquelética por retrusión mandibular y protrusión maxilar, patrón de crecimiento vertical, crecimiento excesivo del complejo nasomaxilar, protrusión de incisivos.
TratamientoOrtopédico: ACCO con tracción alta para retruir e impactar el maxilar y disminuir el crecimiento vertical; con tornillo de expansión (una vuelta a la semana). Arco extraoral uso nocturno y de tres a cuatro horas por las tardes. Placa activa 24 horas y se indica quitar para comer. Tratamiento ortodóntico: aparatología fija Roth .022. Retención: aparato bimaxilar de uso nocturno.
ResultadosDespués de cinco meses de uso del ACCO se volvieron a hacer trazados cefalométricos y se obtuvieron los siguientes valores: relación maxilomandibular: ANB 5° (inicial de 11°), Wits 2mm (inicial 3mm), resalte Bimler 9mm (inicial 10mm), convexidad 6mm (inicial 11mm). Posición maxilar: SNA 82° (inicial 87°). Posición mandibular: SNB: 78° (inicial 76°). Patrón facial: cono facial de 67° (inicial 61° dolicofacial). Dimensión vertical: SN-mandibular 36.5° (inicial 42°), FMA Tweed 35° (inicial 43°), Goniaco Jarabak 130° (inicial 128°). Inclinación de los incisivos: I Sup SN 114° (inicial 117°), I infMand se mantuvo igual (95°).
ConclusionesLa ortopedia en conjunto con la ortodoncia armonizan los maxilares y al mismo tiempo proporcionan estética facial natural, mientras mantienen el adecuado funcionamiento de la masticación, la deglución, la fonación y la respiración. Es de vital importancia realizar un diagnóstico oportuno para poder interceder ortopédicamente y llegar a corregir este tipo de maloclusiones y limitar o evitar su severidad.
In orthodontic practice, poor anteroposterior mandibular relationships comprise the largest number of cases. In this group, class II malocclusion is the most frequent.1
Teeth are positioned where they are because of an inadequate relationship of the bones, aided and supported by a deforming and adaptive muscular activity.2 The correction of the anteroposterior dysplasia should be the first goal of treatment.
Extraoral forces are directed against the maxilla in order to harmonize the direction and the increments of movement in that area with the mandibular pattern.3
Orthodontists began using headgears with modified Hawley retainers many years ago, when there was a dominant class II pattern.
Margolis realized that removable appliances combined with a headgear could not only serve as good containers, but be used as effective correction mechanisms. He called his appliance ACCO (AC acrylic, CO cervicooccipital anchorage).4
The acrylic adaptation over the labial arc of the Hawley-type retainer provides better stability and retention to the appliance and reduces the tilting action that may occur due to the reception of the extraoral force arms in the anterior region. It incorporates an inclined plane to release the mandible thus allowing as much anterior growth as possible and eliminating functional retrusion. Keeping the anterior upper and lower antagonist teeth separated stimulates the eruption of the lower teeth, reducing the overbite and the excessive curve of Spee (Figure 1).
.")
Graber performed a modification of the original Margolis appliance by adding a screw to achieve the necessary expansion.
Margolis instructed his patients to use the ACCO 24hours a day, plus the headgear for at least 12hours a day.5
Generally fixed appliances are used to correct rotations, intrude teeth or close spaces and produce the required root torque in that area. Then again the ACCO for any residual necessary distalization plus the retention.6
CASE REPORTA Mexican female patient of 10 years and 3 months of age with a habit of oral breathing attended the Orthodontics Clinic of the Division of Postgraduate Studies and Research at the National Autonomous University of Mexico. The reason for consultation referred by the patient was «my front teeth show too much».
Clinical examDolichofacial patient, her facial thirds are not proportionate (increased middle third), mild facial asymmetry: asymmetric superciliar, bipupilary subnasal and commissural planes, asymmetric ear implantation, wide nose, slightly asymmetric with good extension round nostrils, thick lips, convex profile, her facial midline does not match the dental midline, gingival smile (she shows the complete crown of the upper incisors and 2 to 3mm of gingival margin). The upper lip was 6mm and the lower lip 9mm with respect to the aesthetic line of Ricketts. She is an oral breather (Figure 2).
Intraoral features Front, B) Smile, C and D) Right and left profile.")
The upper midline does not match the lower midline, molar and canine class I on the left side and on the right side, the canine class is non-assessable and the molar is class I.
3mm overjet, 7mm overbite, 10 permanent teeth on the upper arch, the right first premolar and canine are partially erupted. On the lower arch there are 12 permanent teeth. Upper and lower incisor proclination (Figure 3).
Cefalometric analysis Front, B) Right side, C) Left side.")
Maxillary-mandibular relationship: ANB: 11°, Wits: 3mm, Bimler: 10mm, convexity: 11mm. Maxillary position: SNA: 87°. Mandibular position: SNB: 76°. Facial pattern: facial taper of 61°, dolichofacial. Vertical dimension: SN-mandibular: 42°, FMA (Tweed): 43°, Goniac (Jarabak): 128°. Incisor proclination: UpI/SN 117°, Lo I/Mand 95°.
The patient was diagnosed as a skeletal class II due to mandibular retrusion and maxillary protrusion with a vertical growth pattern, excessive growth of the nasomaxillary complex, a short and flat cranial base, vertically short mandibular ramus and protrusive incisors (Figure 4).
DIAGNOSIS AND TREATMENT PLAN Panoramic. B) Lateral headfilm.")
The facial and functional objectives of the treatment plan were: to decrease vertical growth, improve lip competence, the profile and the smile. Also, it was aimed to maintain the opening pattern and eliminate the mouth breathing habit.
Dental goals: maintain canine and molar class (class I), correct the overjet and rotations, achieve an ovoid shape in both arches and retrocline the upper incisors.
Skeletal objectives: control maxillary growth and try to protrude the mandible.
Orthopedic treatment: ACCO with high-pull headgear (to retrude and impact the protrusive maxilla and decrease vertical growth) and an expansion screw (one turn per week). The headgear must be worn at night and three to four hours in the afternoon. The active plate should be worn 24hours daily and be removed for eating.
Orthodontic treatment: .022 Roth fixed appliances.
Retention: Night time use of a bimaxillary appliance.
TREATMENTDecember 14 2011: ACCO placement with headgear (12 oz). Expansion screw 1 turn per week (Figure 5).

March 12 2012: plate activation was suspended and the screw was blocked with acrylic. Headgear use was continued with a 14 oz force.
June 18 2012: 0.022”-slot Roth appliance placement. Upper and lower 0.014-inch NiTi archwires were placed (Figure 6).

In November 2012 a gingivoplasty and a frenilectomy were performed in the Periodontics Department of the Division of Postgraduate Studies and Research at the National Autonomous University of Mexico (Figure 7).

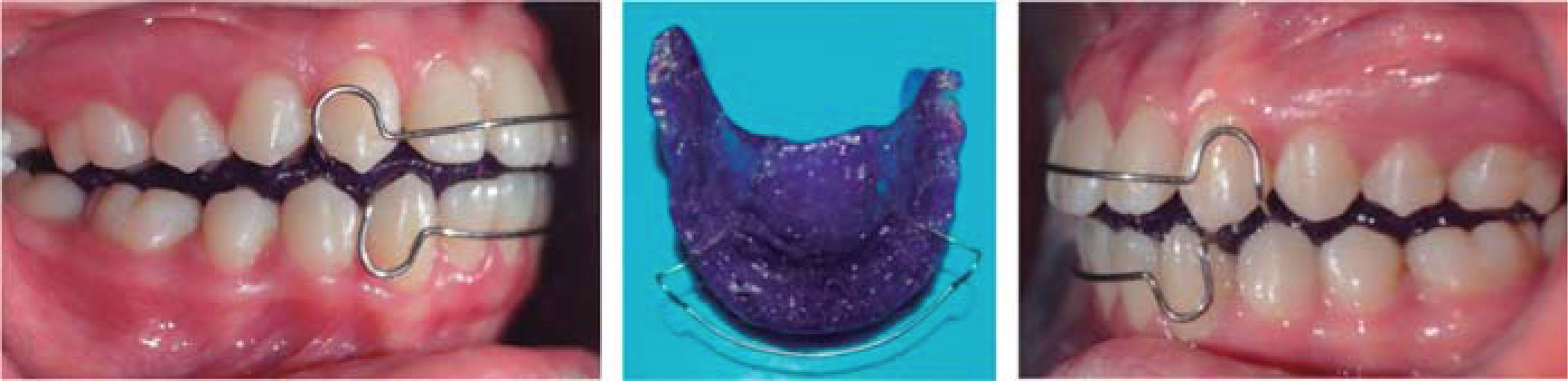
In February of 2013 a single-keyhole loop archwire (SKL) was placed for space closure. Nine months later, 3 ½ oz class II elastics were placed and used for a month. Brackets were maintained for a month as containment and in March 2014 they were removed. A bimaxillary retainer for night use was placed (Figure 8).
RESULTS
After five months of ACCO use, cephalometric tracings were performed again and the following values were obtained: maxillomandibular relationship: ANB: 5° (initial 11°), Wits: 2mm (initial 3mm), Bimler: 9mm (initial 10mm), convexity: 6mm (initial 11mm). Maxillary position: SNA: 82° (initial 87°). Mandibular position: SNB: 78° (initial 76°). Facial pattern: facial taper: 67° (61° initial, dolichofacial). Vertical dimension: SN-mandibular: 36.5° (initial 42°), FMA (Tweed): 35° (initial 43°), Goniac (Jarabak): 130° (initial 128°). Incisor proclination: UpI/SN: 114° (initial 117°), LowI/Mand remained the same (95°) (Figure 9).
DISCUSSION
The use of extraoral forces in orthodontics for solving sagittal problems is not new: Kingsley described the extraoral appliances used today in 1880.7 The introduction of the intermaxillary anchorage in 1893 almost completely eliminated the use of extraoral appliances. However, the Viennese Oppenheim in 1930 reintroduced the headgear in the United States.8
CONCLUSIONSOrthopaedics in conjunction with orthodontics harmonize the maxilla and the mandible while providing natural facial aesthetics and maintaining the proper function of chewing, swallowing, phonation and breathing. It is vitally important to make a timely diagnosis to be able to intervene orthopedically in order to correct this type of malocclusions and limit or prevent its severity.
Graduate from the Specialty of Orthodontics.
This article can be read in its full version in the following page: http://www.medigraphic.com/ortodoncia