




To analyze the relationship among sports practice, physical education class, habitual physical activity and cardiovascular risk in adolescents.
MethodsCross-sectional study with 120 schoolchildren (mean: 11.7±0.7 years old), with no regular use of medicines. Sports practice and physical education classes were assessed through face-to-face interview, while habitual physical activity was assessed by pedometers. Bodyweight, height and height-cephalic trunk were used to estimate maturation. The following variables were measured: body fatness, blood pressure, resting heart rate, blood flow velocity, intima-media thickness (carotid and femoral) and heart rate variability (mean between consecutive heartbeats and statistical index in the time domain that show the autonomic parasympathetic nervous system activity root-mean by the square of differences between adjacent normal R-R intervals in a time interval). Statistical treatment used Spearman correlation adjusted by sex, ethnicity, age, body fatness and maturation.
ResultsIndependently of potential confounders, sports practice was positively related to autonomic parasympathetic nervous system activity (β=0.039 [0.01; 0.76]). On the other hand, the relationship between sport practice and mean between consecutive heartbeats (β=0,031 [–0.01; 0.07]) was significantly mediated by biological maturation.
ConclusionsSport practice was related to higher heart rate variability at rest.
Analisar a relação entre prática esportiva, educação física escolar, atividade física habitual e indicadores cardiovasculares de risco em adolescentes.
MétodosEstudo transversal que selecionou 120 escolares (idade média 11,7±0,7 anos), sem consumo de medicamentos. Prática esportiva fora do ambiente escolar e educação física escolar foram avaliadas por entrevista face a face, enquanto a atividade física habitual foi avaliada por pedometria. Peso corporal, estatura e altura troncocefálica foram usados para estimar a maturação biológica. Foram avaliados: gordura corporal, pressão arterial, frequência cardíaca durante o repouso, velocidade do fluxo sanguíneo, espessura mediointimal das artérias (carótida e femoral), variabilidade da frequência cardíaca (média entre batimentos cardíacos consecutivos e o índice estatístico no domínio do tempo que representa atividade do sistema nervoso autônomo parassimpático por meio da raiz quadrada da média das diferenças sucessivas ao quadrado entre intervalos R-R consecutivos). Correlação de Spearman verificou relação entre as variáveis. Relacionamentos significativos foram ajustados por: sexo, etnia, idade, gordura corporal e maturação biológica.
ResultadosPrática esportiva, independentemente dos ajustes, apresentou correlação positiva com atividade do sistema nervoso autônomo parassimpático (β=0,039 [0,01; 0,76]). Por outro lado, a relação entre tal engajamento e a média entre os intervalos R-R (β=0,031 [–0,01; 0,07]) foi mediada pela maturação biológica.
ConclusõesA prática esportiva foi relacionada a uma maior variabilidade da frequência cardíaca durante o repouso.
It is known that cardiovascular diseases are associated with high morbidity and mortality in adults.1 This fact has been the focus of several studies, mainly due to the subclinical manifestation of their potential indicators of cardiovascular risk factors, such as high blood pressure, intima-media thickness and changes in autonomic modulation,2,3 which tend to manifest since the first decades of life.4 During adolescence, the combination of some of these outcomes can be associated with endothelial dysfunction and early atherogenic process.3 However, it is worth mentioning the difficulty of monitoring the onset of these cardiovascular disorders in young individuals, as their clinical manifestation is observed predominantly in adulthood.3
In this context, the analysis of heart rate variability, which consists in the oscillation of the intervals between consecutive heart beats,5 can be an effective tool to study the association between cardiovascular risk factors3 and autonomic response.5 It is known that parasympathetic activity may be suppressed and closely related to oxidative stress due to cardiometabolic complications.6,7 On the other hand, the same activity can be stimulated by the increase in the cardiorespiratory capacity3 and physical training, both in adults and in children.8
Sports practice in the school environment, combined with Physical Education classes, can be beneficial to the autonomic modulation9; however, the possible effects stimulated by regular physical activity or sports practice outside of the school environment in adolescence are not yet clear. Thus, the aim of this study was to analyze the association between regular physical activity, Physical Education classes and sports practice outside of the school environment on some cardiovascular indicators of health risk among adolescents.
MethodThis was a descriptive-analytical, cross-sectional study, developed with initial information from a cohort that was followed between the years 2013 and 2014 in the city of Presidente Prudente, São Paulo, Brazil. For sample calculation, due to the lack of previous studies indicating scores of correlation between pedometry and blood flow in young Brazilian individuals, we estimated a r=0:26.10 The sample calculation indicated the need to enroll at least 115 adolescents to obtain 80% power and α=5%, considering the estimated correlation. During enrollment, seven elementary schools (4 public and 3 private [the municipality has 82 schools, of which 27 are private]) were initially invited to participate in the study. The schools are close to the University and receive students from different areas of the city, due to the presence of important urban transport lines of the municipality. However, after the school principals were invited to participate, only three private schools agreed to participate (the public schools claimed excess of administrative work). In the school units that authorized the study, all young individuals aged 11-14 years were invited to participate resulting in 495 adolescents from 3 school units invited to the study ([the municipality has 6,108 elementary school students enrolled in private schools]). After the announcement of the study, the documents related to the ethical aspect of the survey were collected, when 127 adolescents returned the correctly filled out documents (there were no exclusions due to filling errors). However, after the completion of all assessments involved in the study, seven adolescents were excluded (did not complete all the tests required by the study), and thus the final sample consisted of 120 adolescents of both genders.
All adolescents who agreed to participate, provided Informed Consent form signed by parents or legal guardians and met the following inclusion criteria: age between 11 and 14 years; regularly enrolled at an elementary school unit; no previously known clinical or metabolic disorders that could interfere with any physical or sports activity, and no eventual or regular consumption of any medication. This study is in accordance with the standards established by the National Health Council (Resolution number 1996/196) and was approved by the Institutional Review Board of Universidade Estadual Paulista, Presidente Prudente campus (number 322,650/2013).
During a face-to-face interview ethnicity was recorded (white, black, Asian, and others), as well as age (difference from date of birth to the assessment date, expressed in centesimal values) and gender of adolescents. The following data were collected: participation in school Physical Education (PE) classes in number of days per week (range 0-3 days), and any sports activities practiced outside of the school environment (including any competitive sports practice supervised by a Physical Education professional or previously qualified instructor). Thus, sports activities outside of the school environment were assessed using the following questions: Do you participate in sports activities outside of the school environment? (dichotomized into yes [1] and no [0]). If yes, on which days of the week do you practice a sports activity? For statistical analysis, the variable “sports practice outside of the school environment” was treated as the number of days in the week in which the adolescents reported this practice (in our sample, this variable ranged from 1-5 days). The habitual physical activity (HPA) was evaluated by a pedometer (Yamax Digiwalker brand, model SW200) attached to the clothes at the hip, over a period of 7 consecutive days. The device computes oscillations in the vertical axis, which reproduce the human gait, and thus the habitual physical activity was expressed by the mean daily number of steps (steps/day).11
Systolic blood pressure (SBP), diastolic blood pressure (DBP) and resting heart rate (rHR) were measured by the oscillometric method, using an automatic device (Omron Healthcare, Inc., IntelliSense, model HEM 742 INT, Bannockburn, Illinois, USA) validated by Christofaro et al.12 For these measures, after a period of 10 minutes of rest in the sitting position, the midpoint of the humerus of the right arm of the assessed subject was involved by a cuff on a suitable size for arm circumference, namely: age up to 13 years [child size] (6 cm × 12 cm) and age older than 13 years [midsize] (9cm×18cm). Obese adolescents used specific cuffs, considering the greater arm circumference. Three measurements were performed with a one-minute interval between them, and the mean of the last two measurements was considered the adolescent's blood pressure (BP).13
The intima-media thickness (IMT) and the arterial blood flow were measured by a single physician, specialized in imaging diagnosis, using Doppler ultrasound assessment (Philips HD 11 XE, Brazil) equipped with a high-resolution multi-frequency linear transducer, adjusted to 12 MHz. The recommendations of the Brazilian Society of Cardiology were used for this assessment,14 which evaluated the common carotid and femoral arteries (right side), followed by the estimation of the following variables: IMT, which corresponds to the distance between the two echogenic lines representing the lumen/intima and media/adventitia interfaces of the arterial wall15 of the common carotid (CCA-IMT) e femoral artery (FA-IMT), and the index of resistance to blood flow, calculated by the sum of the maximum and minimum blood flow velocity divided by the maximum flow velocity of the common carotid (CCA-IR) and femoral artery (FA-IR). During the evaluation of the common carotid artery, the neck was slightly hyperextended and inclined to an angle of approximately 45º. For measurements in the femoral artery, the adolescent's leg remained stretched out on a stretcher, and the measurements were performed close to the inguinal region.
For the assessment of heart rate variability (HRV), the resting heart rate was recorded beat by beat using a heart rate monitor (Polar®, model RS800, Kempele, Finland), validated for the purposes of this study.16 The adolescents remained in the supine position and on spontaneous breathing for 30 minutes for this measurement, with electrodes positioned at the xiphoid process of the sternum. The watch used for data recording was placed on the wrist of the subjects, who kept their arms extended at the side of the body. All adolescents were instructed to refrain from caffeine intake and physical activity for 24 hours before the test,3 and assessments were carried out in the morning to avoid possible influences of the circadian rhythm, in an acclimatized room at 25 ºC (±1 ºC), following previous recommendations.17
Data recorded on the beat-to-beat mode in milliseconds were downloaded by infrared transmission on a laptop computer using Polar Pro Trainer software, release 5.41.002. The data filtering method was carried out in two stages: digital filtering through the software used to download the data, and manual filtering in order to visually check the variations in the intervals between heartbeats and therefore remove abnormal intervals.5,18 A total of 1,000 R-R intervals were used for data analysis, and the mean value between the R-R intervals (M-RRi) and the variability index of heart rate using the linear method in the time domain (rMSSD) were calculated using Kubios HRV software, release 2.0. The rMSSD index corresponds to the root mean square of successive differences squared between consecutive R-R intervals, in which it represents the predominance of the parasympathetic autonomic nervous system activity.5
All measurements were carried out with the subjects wearing light clothing and no shoes. Body weight was measured in a digital scale (Filizola, Personal Line 200 model, Brazil) with a precision of 0.1 kg, while height was measured using a stadiometer fixed on the wall (Sanny, Professional model, Brazil) to the nearest 0.1 cm. Sitting height was obtained using a wood bench with a height of 50 cm attached to the stadiometer. The length of the legs was obtained by subtracting sitting height from the height.19 Based on these measures, biological maturation was estimated by peak growth velocity (PGV), using mathematical models based on anthropometric measurements.20 The results obtained from this model indicate the remaining time (years) until the adolescent reaches somatic maturation.
Adipose tissue was measured by bone densitometry (General Electric, model Lunar - DPX-NT). The equipment was calibrated before the start of the measurements, in order to verify the guarantee of quality of the assessments, according to the manufacturer's recommendations. After this initial procedure, the whole body scan of the sample was performed. The radiation dose was not detrimental to the health of the adolescents, being less than 0.05 millirem. During the examination, all participants used lightweight clothing, remained barefoot, with no metal objects on their bodies, being positioned on the equipment in the supine position throughout the examination and remaining motionless for approximately 15 minutes. Body fat (BF) was expressed in percentages using the software GE Medical Systems Lunar, release 4.7.
Initially, at the statistical analysis, the distribution of the data set was tested according to the Gaussian model and, based on this assumption, we chose the non-parametric statistics for the correlation analyses. For the multivariate model, the rMSSD index was submitted to logarithmic transformation (base-10 logarithm).21
To describe the sample, the median and the difference between quartiles were used, with the difference between groups (dichotomized into yes [1] or no [0]) engaged in sports practice expressed by the Mann-Whitney test. Due to the use of certain non-parametric variables, Spearman's correlation (rho) was used to verify the association between sports practice and the cardiovascular health risk indicators. The significant associations in Spearman's correlation were entered into the multivariate model (linear regression) using two models: Model 1 - adjusted by gender, ethnicity, age and BF, and Model 2 - PGV in addition to Model 1 variables.
Similarly, significant comparisons were analyzed from the perspective of the analysis of covariance (ANCOVA [adjusted for gender, ethnicity, age and BF]), which generated means estimated after adjustment of variance explained by confounding variables. The Bonferroni post hoc test was used when necessary, and the Levene test demonstrated the homogeneity of variances for the models. Finally, effect size measures were provided by the eta-squared (ES-r) (Small 0.010 to 0.059, Moderate 0.060 to 0.139, and High ≥0.140).22 Statistical significance (p-value) was considered relevant when values were <5%, and it was analyzed by the BioEstat software (release 5.0, Tefé, Amazonas).
ResultsOf the total study sample, 50% (95% CI: 41.1%-58.9%; n=60) of the adolescents reported being involved in some sports practice outside of the school environment (56.5% boys and 43.1% girls; p=0.201). PE classes were not associated with any other physical activity indicator (sports and HPA); however, and as expected, sports activities outside of the school environment and the HPA were associated.
The dependent variables (M-RRi, rMSSD, CCA-RI, FA-RI, CCA-IMT, and FA-IMT) did not differ when the sample was stratified according to the HPA and the number of PE classes. On the other hand, when the sample was dichotomized by sports practice outside of the school environment, there was a significant difference for age (p=0.042), body weight (p=0.048), height (p=0.043), PGV (p=0.003), M-RRi (p=0.012) and rMSSD (p=0.019) (Table 1).
Comparative analysis of the dependent variables according to sports practice outside of the adolescents' school environment, Presidente Prudente, São Paulo. Brazil, 2013. Values expressed in medians (difference between quartile).
| Sports practice outside of the school environment | p-value | ||
|---|---|---|---|
| Yes (n=60) | No (n=60) | ||
| Age (years) | 12 (1) | 11 (1) | 0.042 |
| Weight (kg) | 51.2 (19) | 49.2 (19.2) | 0.048 |
| Height (cm) | 1.57 (0.10) | 153 (0.10) | 0.043 |
| BF (%) | 31.5 (13.6) | 28.9 (19.4) | 0.361 |
| PGV | −2.13 (0.93) | −2.54 (1.10) | 0.003 |
| mSBP (mmHg) | 113.3 (15.7) | 108.8 (16.1) | 0.118 |
| mDBP (mmHg) | 68.3 (10.7) | 65.0 (15.7) | 0.719 |
| rHR (bpm) | 76.6 (15.1) | 75.6 (15.5) | 0.659 |
| M-RRi (ms) | 781.6 (142.1) | 740.1 (138.1) | 0.012 |
| rMSSD (ms) | 49.5 (26) | 43.0 (29) | 0.019 |
| CCA-IMT (mm) | 0.45 (0.05) | 0.46 (0.05) | 0.228 |
| FA-IMT (mm) | 0.39 (0.08) | 0.38 (0.11) | 0.991 |
| CCA-RI | 0.75 (0.1) | 0.73 (0.1) | 0.194 |
| FA-RI | 0.94 (0.1) | 0.98 (0.1) | 0.506 |
| Steps/day | 9804.5 (6545) | 8139.2 (3085) | 0.086 |
BF, body fat; PGV, peak growth velocity; mSBP, mean systolic blood pressure; mDBP, mean diastolic blood pressure; rHR, resting heart rate; MRRi, mean RR interval; rMSSD, root mean square of successive differences between adjacent normal RR intervals; CCA-IMT, common carotid artery intima-media thickness; FA-IMT, femoral artery intima-media thickness; CCA-RI, common carotid artery resistance index; FA-RI femoral artery resistance index.
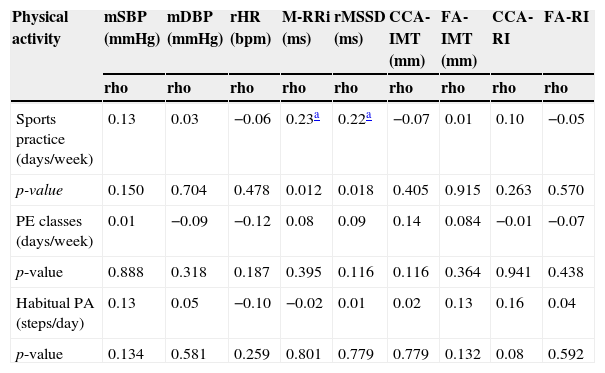
ANCOVA identified that even after controlling variance explained by the confounding factors, young individuals who practiced sports still showed higher values for HRV, and the effect magnitude of the sports practice on the dependent variables was moderate (Table 2). Sports activities outside of the school environment had a significant and positive association with M-RRi (rho=0.23) and rMSSD (rho=0.25). On the other hand, the HPA and PE classes were not associated with any of the outcomes involved in this study (Table 3).
Means (95% confidence interval) adjusted for gender, age, body fat, ethnicity and sexual maturation for the values of heart rate variability according to sports practice in adolescents, Presidente Prudente, São Paulo. Brazil, 2013.
| Heart rate variability | No sports practice (n=60) | With sports practice (n=60) | ANCOVA | Size of effect | ||
|---|---|---|---|---|---|---|
| F | p–value | ES-r | (Qualitative) | |||
| M-RRi (ms) | 726.5 (693.1–759.9) | 797.7 (765.1–830.5) | 8.674 | 0.004 | 0.078 | Moderate |
| rMSSD (ms) | 41.8 (35.7–47.8) | 53.1 (47.1–59.1) | 6.680 | 0.011 | 0.061 | Moderate |
HR, heart rate; M-RRi, mean RR interval; rMSSD, root mean square of successive differences between adjacent normal RR intervals; 95%CI, 95% confidence interval; ANCOVA, analysis of covariance; ES-r, eta squared, which denotes an effect size measure; p-value <0.05, statistical significance.
Mean and 95% CI estimated by ANCOVA.
Spearman's correlation (rho) between physical activity indicators and cardiovascular parameters in adolescents. Presidente Prudente, São Paulo. Brazil, 2013.
| Physical activity | mSBP (mmHg) | mDBP (mmHg) | rHR (bpm) | M-RRi (ms) | rMSSD (ms) | CCA-IMT (mm) | FA-IMT (mm) | CCA-RI | FA-RI |
|---|---|---|---|---|---|---|---|---|---|
| rho | rho | rho | rho | rho | rho | rho | rho | rho | |
| Sports practice (days/week) | 0.13 | 0.03 | −0.06 | 0.23a | 0.22a | −0.07 | 0.01 | 0.10 | −0.05 |
| p-value | 0.150 | 0.704 | 0.478 | 0.012 | 0.018 | 0.405 | 0.915 | 0.263 | 0.570 |
| PE classes (days/week) | 0.01 | −0.09 | −0.12 | 0.08 | 0.09 | 0.14 | 0.084 | −0.01 | −0.07 |
| p-value | 0.888 | 0.318 | 0.187 | 0.395 | 0.116 | 0.116 | 0.364 | 0.941 | 0.438 |
| Habitual PA (steps/day) | 0.13 | 0.05 | −0.10 | −0.02 | 0.01 | 0.02 | 0.13 | 0.16 | 0.04 |
| p-value | 0.134 | 0.581 | 0.259 | 0.801 | 0.779 | 0.779 | 0.132 | 0.08 | 0.592 |
mSBP, mean systolic blood pressure; mDBP, mean diastolic blood pressure; rHR, resting heart rate; M-RRi, mean RR interval; rMSSD, root mean square of successive differences between adjacent normal RR intervals; CCA-IMT, intima-media thickness of the common carotid artery; FA-IMT, intima-media thickness of the femoral artery; CCA-RI, common carotid artery resistance index; FA-RI, femoral artery resistance index; rho, Spearman's correlation coefficient; 95% CI, 95% confidence interval; PE, physical education; PA, physical activity.
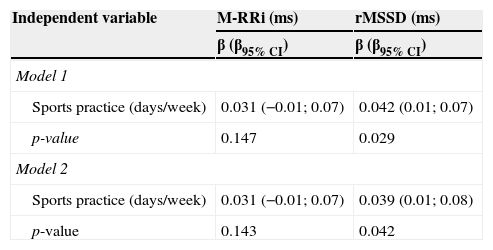
In the multivariate model, only the rMSSD index remained associated with sports practice, after adjustment for confounders (model 1 [gender, ethnicity, age and BF]). Finally, the rMSSD index remained associated with sports practice outside of the school environment, even after statistical control (model 2) for organic maturation (×=0.039 [0.01;0.08]) (Table 4).
Multivariate models (linear regression) including sports practice outside of the school environment and cardiovascular risk indicators for the adolescents' health, Presidente Prudente, São Paulo. Brazil, 2013.
| Independent variable | M-RRi (ms) | rMSSD (ms) |
|---|---|---|
| β (β95% CI) | β (β95% CI) | |
| Model 1 | ||
| Sports practice (days/week) | 0.031 (−0.01; 0.07) | 0.042 (0.01; 0.07) |
| p-value | 0.147 | 0.029 |
| Model 2 | ||
| Sports practice (days/week) | 0.031 (−0.01; 0.07) | 0.039 (0.01; 0.08) |
| p-value | 0.143 | 0.042 |
M-RRi, mean RR interval; rMSSD, root mean square of successive differences between adjacent normal RR intervals; 95% CI, 95% confidence interval; Model 1, adjusted for gender, ethnicity, age and body fat; Model 2, adjusted for gender, ethnicity, age, body fat and peak growth velocity.
The results of this study indicate that adolescents engaged in sports activities outside of the school environment had higher HRV, even when the analysis was controlled for factors such as biological maturation. On the other hand, this association was not observed for PE classes and HPA.
In this study, adolescents engaged in sports activities outside of school were older and had higher body weight, height and biological maturation. It is known that, with advancing age, there is a tendency to decreased vagal response and decline in HRV23; however, this behavior does not seem to be accentuated among adolescents.17 It should be noted that physical exercise has a modulating role in cardiorespiratory fitness and, therefore, may slow the reduction in parasympathetic activity.23,24
In parallel, the literature has identified that the cardiorespiratory fitness of obese adolescents engaged in physical exercises is closely associated with the increase in vagal response during rest,3 as well as detraining is closely associated to the decrease in the rMSSD index.25 Recently, Fernandes et al.24 observed that the reducing effect of sports on the behavior of rHR was mediated by its action on cardiorespiratory fitness (regardless of BF). In this sense, our results demonstrate that sports activities outside of the school environment are characterized as an important variable associated with autonomic modulation, as the rMSSD has been shown in the literature as an important indicator index of parasympathetic activity.5,25
On the other hand, CCA-IMT and FA-IMT, as well as CCA-IR and FA-IR showed no significant association with any of the physical activity indicators. The literature has shown that increase in the shear stress caused by exercise can stimulate the release of “cardioprotective” substances at the expense of the resistance that blood flow exerts on endothelial cells.26 These biomolecular messengers have the capacity to inhibit oxidative stress, platelet aggregation and smooth muscle cell proliferation,26 with all these cardiometabolic responses being involved with IMT in the long-term,2 not being necessarily observed in young populations. Supporting this hypothesis, a similar result was observed by Loprinzi et al.27 with adolescents of both genders (age ranging from 6-18 years), in which the practice of HPA was associated with lower C-reactive protein values (important inflammatory agent closely related to the atherogenic process) in adults, but not in young individuals.
An important consideration on the lack of associations between HPA, physical activity outside of the school environment and the analyzed outcomes needs to be made. In fact, total physical activity is a construct that involves activities of all intensities (not necessarily of moderate to high intensity), and therefore the non-significant coefficients were not a big surprise. However, the non-significant results for PE classes reflect a deficiency in our educational system (previous information report low energy demand involved in this type of activity, and a substantial part of the Physical Education class is spent with activity management),28 as actions in the school environment have been effective in improving the HRV.9 Therefore, the practice of sports has been clearly demonstrated and consistently widespread among children and adolescents, not only due to its importance in the formation of the young individuals' personality,29 but also due to its importance in increasing the time spent in moderate and vigorous intensity physical activities and its impact on the abovementioned health indicators.30
Some limitations must be mentioned. The cross-sectional design does not allow establishing a causal association between the observed outcomes. However, these results are derived from the preliminary data of an ongoing cohort and thus, in the future, these findings might be reanalyzed from a longitudinal perspective. Additionally, the absence of more accurate information about PE classes and sports activities outside of the school environment (intensity of exercise, session length, sports modality, time spent with that sports modality, etc.) deserves to be highlighted as a limitation. On the other hand, recent data in the literature showed that achieving at least 11,500 steps/day is similar to achieving the minimum guideline for physical activity in young individuals: 60 minutes/day of physical activity of moderate or vigorous intensity.11 In this sample, there was an association between achieving the cutoff of steps a day and being involved in sports activities (OR=3.05; 95% CI: 1.25 to 7.39), and the number of days involved with sports activities was associated with the total number of steps accumulated during the week (r=0.21; 95% CI: 0.02-0.37). Thus, these data demonstrate that, although relatively simple, the questions used to characterize the organized practice of sports were effective in differentiating more physically active young individuals.
Therefore, it can be concluded that the practice of sports outside of the school environment was related to HRV indicators at rest.
FundingFundação de Amparo a Pesquisa do Estado de São Paulo (FAPESP; Process n. 2013/06052-2) and CNPq (Universal Announcement 14/2013; Process n. 476295/2013-0).
Conflicts of interestThe authors declare no conflicts of interest.
