


This paper aims to study the role of nine variables in the susceptibility to External apical root resorption (EARR), in order to obtain an integrative model to predict the occurrence of this orthodontic-induced complication.
Materials and methods212 patients treated with multi-bracket appliances were studied. Root resorption was measured in the four maxillary incisors and maxillary canines using before and after treatment radiographs (2544 measured teeth). A design-to-purpose software was developed to optimize image processing and data collection. For each patient, the tooth with maximum percentage of root resortion (%EARRmax) was evaluated. A multiple linear regression model was used to assess the role of nine clinical and treatment variables to the susceptibility of EARR.
ResultsThe analysis of intra-observer mean error confirmed the reliability of the method (Student's t test for paired samples and Dahlberg test). Five clinical and treatment variables explained 28% of the %EARRmax variance: gender, treatment duration, anterior open bite, premolar extractions and Hyrax appliance. Other variables, such as age, tongue thrust, overjet and skeletal pattern, had less significant effect on %EARRmax.
ConclusionAmong the clinical and treatment variables studied that are potential contributors for EARR, five variables associated with root resorption were identified.
Estudar a influência de nove variáveis na suscetibilidade à reabsorção radicular apical externa (RRAE), com o propósito de obter um modelo integrado que preveja a ocorrência desta complicação induzida pelo tratamento ortodôntico.
MétodosForam estudados 212 pacientes tratados com aparelhos ortodônticos multi-bracket. A RRAE foi avaliada através de radiografias realizadas antes e após o tratamento ortodôntico, tendo-se analisado os 4 incisivos e os 2 caninos do maxilar superior. Para tal, foi desenvolvido um protótipo de software que permite optimizar o processamento de imagem e registar de forma automática a percentagem de reabsorção radicular. Para cada paciente, foi considerado o dente com percentual máximo de reabsorção radicular (%RRAEmax). Usando um modelo de regressão linear múltipla, a contribuição das nove variáveis clínicas e relacionadas com o tratamento foi analisada.
ResultadosA análise do erro médio intra-observador confirmou a fiabilidade do método (teste t de Student para amostras emparelhadas e fórmula de Dahlberg). Verificou-se que 28% da variância da %RRAEmax era explicada por cinco variáveis: sexo, duração do tratamento, aparelho Hyrax, mordida aberta anterior e extração de pré-molares. Outras variáveis, como idade, interposição lingual, overjet e padrão esquelético, não tiveram uma contribuição significativa.
ConclusõesDas variáveis clínicas e relacionadas com o tratamento estudadas, que podem contribuir potencialmente para a RRAE, cinco foram associadas ao fenómeno de reabsorção radicular.
External apical root resorption (EARR) is a complex, multifactorial phenotype, determined by host and environmental factors, which are still not clearly identified.1–4 Biological or host-related risk factors that have been described include genetic susceptibility,2,5–7 gender,3,8–10 age,9,11–14 tongue thrust, existence of anterior open bite, type of malocclusion14 and systemic diseases.3,4 Environmental factors mainly concern mechanical or orthodontic treatment variables like treatment duration,9,14 type of orthodontic appliance,1 tooth extraction,8,9 intrusive movement, root torque and force magnitude. Polymorphisms in interleukin 1 gene and a few other loci have also been implicated, but results remain controversial.7,9,10,15 Lessons from other well-studied complex phenotypes like diabetes have shown that genotyping hardly contributes to improve clinical evaluation of disease susceptibility.16
There are no strict criteria for the diagnosis of this phenotype. Levander and Malmgren have proposed the evaluation of root resorption using ordinal scales,17 whereas others have assessed it by measuring root lengths,11,13,18 and arbitrary cut-offs, with no prognostic correlation, that have been frequently used. In clinical orthodontics, panoramic and cephalometric X-rays/radiographs are routinely ordered as the primary diagnostic tool. Although less accurate than periapical films, panoramic radiographs have advantages like less radiation exposure and visualization of the complete dentition, besides being less time-consuming for the operator and even more patient-friendly. Panoramic films may overestimate by approximately 20% the amount of root loss19 but this magnification factor is relatively constant in the vertical axis,20,21 which is clinically the most important aspect in analyzing EARR.22 This overestimation can be overcome using the percentage of root/tooth length variation instead of direct measurement of root length. In addition, mainly due to image distortion, comparison of panoramic with periapical films has revealed maximum differences in the lower incisors, but minimum in the maxillary incisors,19 precisely the most frequently affected teeth.1 Recent advances in digital image processing and artificial intelligence techniques offer more precise computer-assisted methods for dental X-ray analysis. Three-dimensional imaging systems are known to be the best way to evaluate EARR, though not easy to apply in clinical practice.
In order to individualize orthodontic treatment choices, it would be particularly important to predict each patient's risk of developing EARR.
The aim of this work was to evaluate the contribution of several clinical and treatment factors to orthodontic-induced EARR, in order to create a multifactorial integrative model that would predict the risk of developing this common orthodontic complication.
Materials and methodsFor this retrospective study, 212 patients who had been submitted to orthodontic treatment were selected from the archives of two orthodontic clinics and from the Orthodontic Department of the School of Dental Medicine (Faculty of Medicine, University of Coimbra). The sample included 79 males and 133 female patients, with an average age of 17 years (SD±6.63). Criteria used for patient selection were the following: caucasian origin with completed comprehensive orthodontic treatment (straight-wire technique) and high-quality panoramic radiographies before and after treatment; completely formed maxillary incisors and canines by the beginning of treatment; absence of fractures, abrasion or dental cavities on the incisal edges between measurements; absence of aberrant morphology of roots that could interfere with length measurement; absence of craniofacial malformation and absence of congenitally missing, supernumerary or impacted maxillary canines or incisors. Nine clinical and treatment variables were analyzed using a multiple regression model: gender, age, treatment duration, premolar extractions, skeletal pattern, Hyrax appliance, overjet, anterior open bite and tongue thrust.
This study was performed within the ethical principles governing medical research and human subjects as mentioned in the Helsinki Declaration (2002 version, www.wma.net/e/policy/b3.htm) as well as with the approval of the Research Ethics Commission of the Faculty of Medicine of Coimbra University. All patients signed a written informed consent.
In order to classify patients’ skeletal pattern, measurements were performed on pre-treatment lateral cephalometric X-rays. Both panoramic radiographies (before and after treatment) were performed with the same equipment. The standard quality criteria of a panoramic X-ray were observed. The 424 panoramic radiographs were digitalized (300 dpi, 256 gray levels) using a scanner (Expression 1680 Pro, Epson) and saved in TIFF. For each patient, the four maxillary incisors and maxillary canines were measured using before (T-1) and after (T-2) orthodontic treatment X-rays.
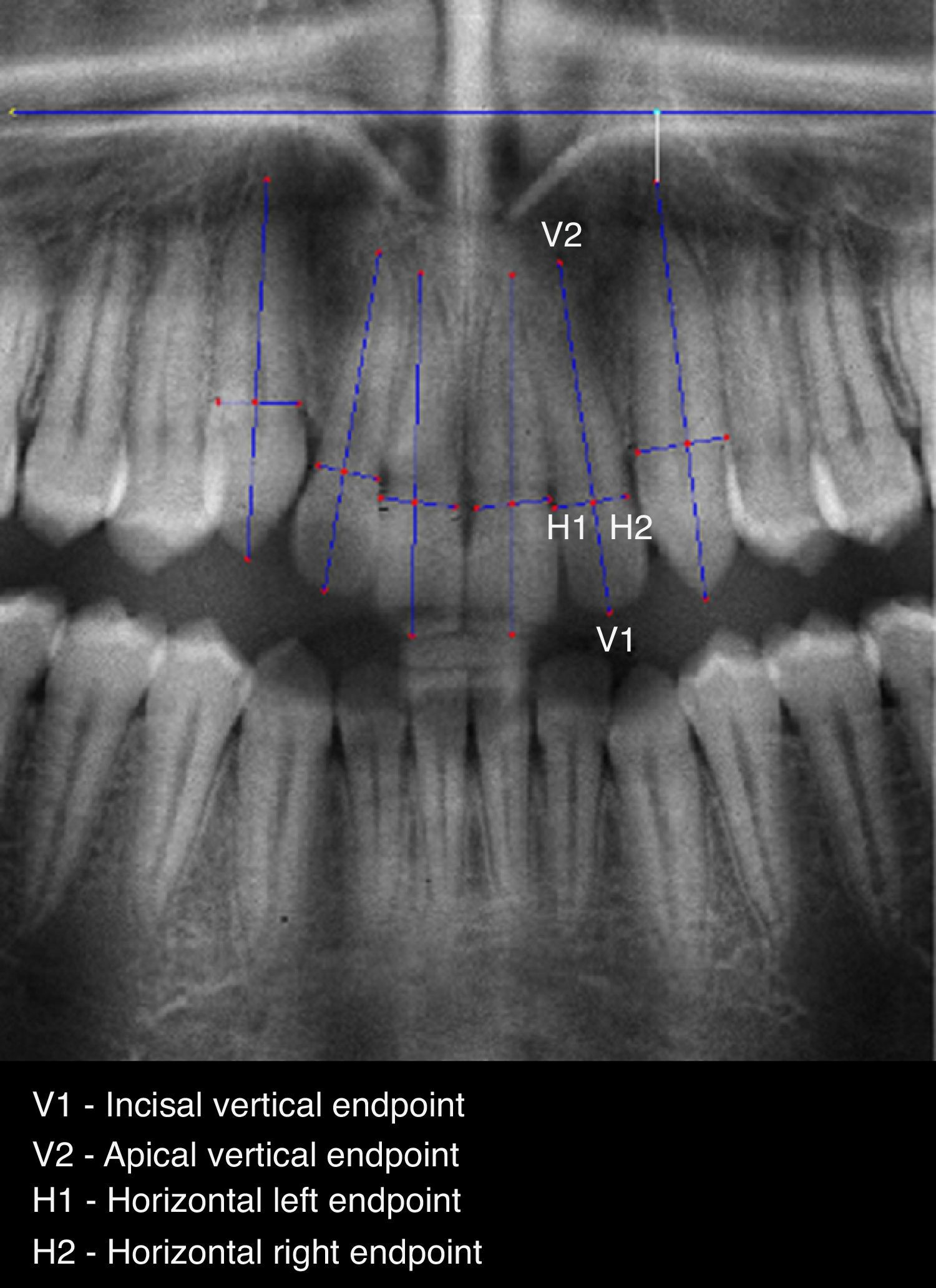
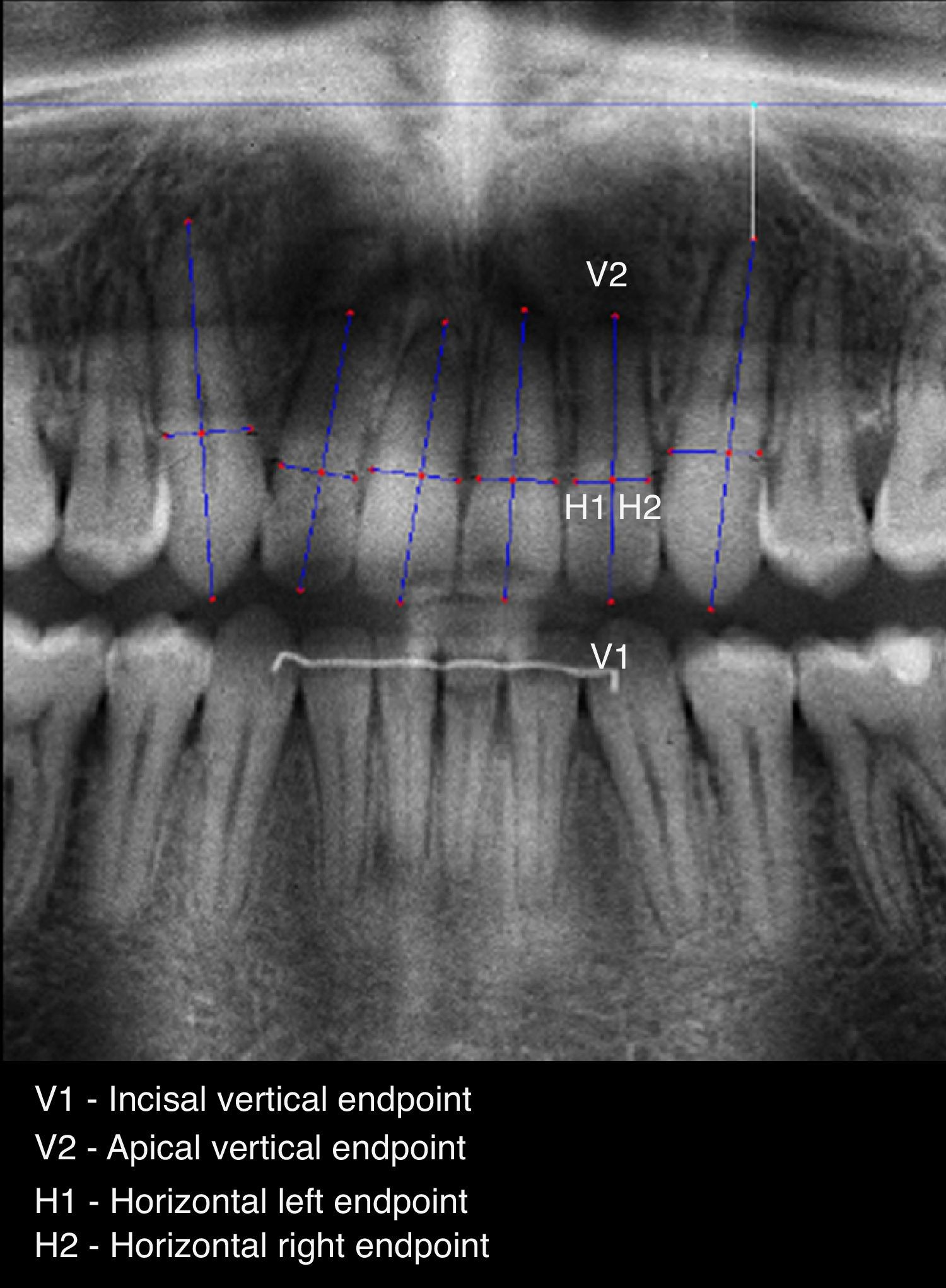
To allow a standardized and accurate method for measuring EARR, a software prototype (ARIAS – Apical Resorption Image Analysis System) in MATLAB version 7.12.0.635 (R2011a) was developed. The proposed method includes the following three steps: (1) image preprocessing, allowing the application of image enhancing filters; (2) point selection, manually marking 4 points on each selected tooth: two points, V1 and V2 (the vertical points) defining a vertical line segment outlining the intersection between root and crown, and two points H1 and H2 (the horizontal points) defining a horizontal line segment that represents the tooth width (Figs. 1 and 2) and (3) feature extraction, to automatically produce a set of linear measurements in T1 and T2 radiographic images, such as: initial root length (R1), initial crown length (C1), final root length (R2), final crown length (C2) and corrected final root length (CR2) – Table 1.


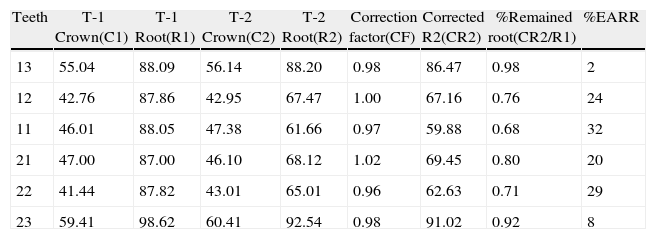
Data obtained from automatic computing of measurements,a using ARIAS.
| Teeth | T-1 Crown(C1) | T-1 Root(R1) | T-2 Crown(C2) | T-2 Root(R2) | Correction factor(CF) | Corrected R2(CR2) | %Remained root(CR2/R1) | %EARR |
| 13 | 55.04 | 88.09 | 56.14 | 88.20 | 0.98 | 86.47 | 0.98 | 2 |
| 12 | 42.76 | 87.86 | 42.95 | 67.47 | 1.00 | 67.16 | 0.76 | 24 |
| 11 | 46.01 | 88.05 | 47.38 | 61.66 | 0.97 | 59.88 | 0.68 | 32 |
| 21 | 47.00 | 87.00 | 46.10 | 68.12 | 1.02 | 69.45 | 0.80 | 20 |
| 22 | 41.44 | 87.82 | 43.01 | 65.01 | 0.96 | 62.63 | 0.71 | 29 |
| 23 | 59.41 | 98.62 | 60.41 | 92.54 | 0.98 | 91.02 | 0.92 | 8 |
It is accepted that during orthodontic treatment the crown length does not change, so, the ratio between the initial crown length and the final crown length (C1/C2) determines the enlargement factor to be used to determine the corrected final root. The six anterior maxillary teeth were measured using the Linge and Linge method,11 modified by Brezniak et al.23 The root and crown lengths in both T-1 and T-2 radiographic images were then used by the software to calculate the other parameters. Mathematical formulations computed to obtain the final %EARR are shown below:
CF=C1/C2; where CF is the correction factor
CR2=R2/CF; where CR2 is the corrected final root
Ratio CR2/R1; represents the remaining root ratio
%EARR=1−(CR2/R1)
This program speeds up measuring and decreases the introduction of human errors, as all of the predetermined parameters are automatically computed and can be saved to an individual Microsoft Excel file associated to each patient.
To avoid inter-observer error, the same operator – specialist in orthodontics (S.A.P.) – performed all the measurements. The intra-observer error analysis on measuring panoramic radiographs consisted of a statistical evaluation of the difference between 2 measurements, taken 15 days apart, on each tooth type, from 20 random patients.
The difference in measurements was assessed by Student's t-test for paired samples (systematic error) and by the Dahlberg formula (random error). A one-way repeated measurement using ANOVA with post hoc tests was conducted to compare EARR of the selected teeth. In order to globally analyze EARR in each patient and not only in each separate tooth, the maximum observed %EARR (%EARRmax) of the six selected teeth was considered. A Chi-square goodness of fit test was used to assess whether the distribution of the maximum observed EARR was homogeneous among the six teeth. As EARR is a quantitative variable, instead of dividing patients into arbitrary grades of EARR severity, a multiple regression model was used to explore the relationship between the maximum observed EARR on the six selected teeth and 9 clinical and treatment variables. The statistical package SPSS (version 19.0, IBM SPSS Statistics for Windows, IBM Corp.) was used.
ResultsFor systematic error (t-test), there were no statistically significant differences between the 2 measurements performed by the same operator (P>0.05); for random error (Dahlberg formula), values varied between 0.5% and 1%, being not clinically significant.
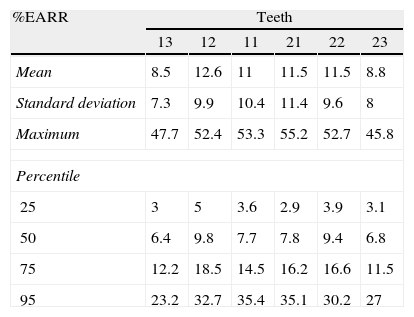
In the first step, for each tooth, EARR values were analyzed in the 212 patients (Table 2). On average, %EARR ranged from 8.5% (tooth 13) to 12.6% (tooth 12). For 95 percentile, values ranged from 23.2% (tooth 13) to 35.4% (tooth 11). Root resorption was higher in incisors than in canines (P<0.01).
Results of %EARR for each tooth (n=212).
| %EARR | Teeth | |||||
| 13 | 12 | 11 | 21 | 22 | 23 | |
| Mean | 8.5 | 12.6 | 11 | 11.5 | 11.5 | 8.8 |
| Standard deviation | 7.3 | 9.9 | 10.4 | 11.4 | 9.6 | 8 |
| Maximum | 47.7 | 52.4 | 53.3 | 55.2 | 52.7 | 45.8 |
| Percentile | ||||||
| 25 | 3 | 5 | 3.6 | 2.9 | 3.9 | 3.1 |
| 50 | 6.4 | 9.8 | 7.7 | 7.8 | 9.4 | 6.8 |
| 75 | 12.2 | 18.5 | 14.5 | 16.2 | 16.6 | 11.5 |
| 95 | 23.2 | 32.7 | 35.4 | 35.1 | 30.2 | 27 |
%EARR – % of external apical root resorption.
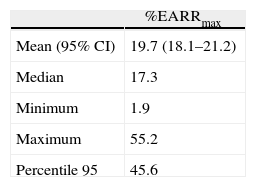
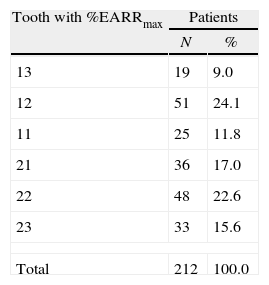
Considering the maximum %EARR value obtained in each patient, from the six teeth (%EARRmax), results ranged from 1.9% to 55.2%, with an average of 19.7%, a median of 17.3% and 45.6% for percentile 95 (Table 3). As for %EARR, the distribution of %EARRmax (Table 4) was not homogeneous, with the lateral incisors being the most frequently involved teeth (P<0.01).
The correlation between %EARRmax and the 9 variables was assessed using a multiple regression model. At an initial stage, the multiple regression was conducted with all individuals but the standardized residual values suggested that 5 subjects should be removed (1 male and 4 females).
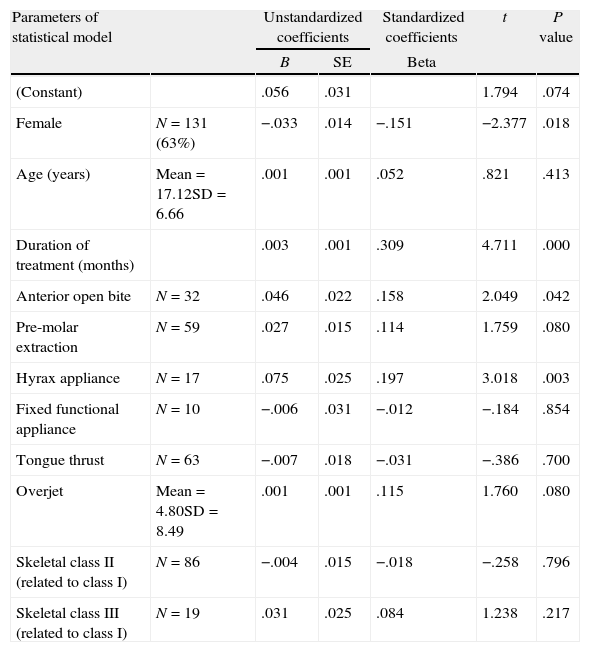
The final model (Table 5, n=207) showed that the clinical variables explained 28% of the %EARRmax variance (ANOVA: F=6.901, P=0.000; adjusted determination coefficient=0.24). Individually, the variables with more significant contribution to the model were: gender (P<0.05), treatment duration (P<0.001), anterior open bite (P<0.05), premolar extractions (P<0.1), Hyrax appliance (P<0.01) and overjet (P<0.1). Other variables, like age, tongue thrust and skeletal pattern, had only minor contributions.
Results of multiple regression model (n=207a).
| Parameters of statistical model | Unstandardized coefficients | Standardized coefficients | t | P value | ||
| B | SE | Beta | ||||
| (Constant) | .056 | .031 | 1.794 | .074 | ||
| Female | N=131 (63%) | −.033 | .014 | −.151 | −2.377 | .018 |
| Age (years) | Mean=17.12SD=6.66 | .001 | .001 | .052 | .821 | .413 |
| Duration of treatment (months) | .003 | .001 | .309 | 4.711 | .000 | |
| Anterior open bite | N=32 | .046 | .022 | .158 | 2.049 | .042 |
| Pre-molar extraction | N=59 | .027 | .015 | .114 | 1.759 | .080 |
| Hyrax appliance | N=17 | .075 | .025 | .197 | 3.018 | .003 |
| Fixed functional appliance | N=10 | −.006 | .031 | −.012 | −.184 | .854 |
| Tongue thrust | N=63 | −.007 | .018 | −.031 | −.386 | .700 |
| Overjet | Mean=4.80SD=8.49 | .001 | .001 | .115 | 1.760 | .080 |
| Skeletal class II (related to class I) | N=86 | −.004 | .015 | −.018 | −.258 | .796 |
| Skeletal class III (related to class I) | N=19 | .031 | .025 | .084 | 1.238 | .217 |
B – value of the unstandardized coefficient; SE – standard error; SD – standard deviation.
The contribution of each single significant variable to %EARRmax (unstandardized B coefficient) revealed that average female values were 3% below male values (B=−0.033); each additional month of treatment represented an average increase of 0.3% (B=0.003); anterior open bite was associated with another 5% of %EARRmax (B=0.046); use of Hyrax appliance increased the amount of %EARRmax by 8% (B=0.075); premolar extractions were associated with more than 3 of %EARRmax (B=0.027) and each additional score on overjet represented an average increase of 0.1% (B=0.001) (Table 5).
DiscussionEARR is a multifactorial phenotype, resulting from a combination of biological and mechanical risk factors, which remains highly controversial. In the present study, using a multiple regression model, the role of 9 clinical and treatment variables in the susceptibility to EARR was analyzed.
There is no ideal method for root measurement. Even periapical film accuracy has been questioned because of errors caused by variability in tooth shape.24 Nowadays, cone beam computed tomography (CBCT), a three-dimensional imaging system, is regarded as the most valid and accurate technique to evaluate EARR.25 The improvement of the accuracy of panoramic films to evaluate EARR is very important for clinicians, since this diagnostic radiograph tool is systematically ordered in orthodontics and allows the immediate evaluation of all dentition without extra radiation exposure.
In studies of orthodontic-induced EARR there are numerous references to both periapical12–14 and panoramic films,2,7,9,10,14,15 with the latter frequently including more teeth2,5,7,10,15 and larger population samples.2,5,7 Limitations of panoramic measurements are the magnification factor and distortion, but these are less critical for maxillary teeth,19 which were evaluated. A software prototype that allowed an improvement in the degree of accuracy and reproducibility of measurements for digital panoramic films, minimizing human error and avoiding workload, was implemented. To achieve further accuracy, instead of measuring the root length7 the % of EARR was calculated. The measurements in our method were reliable as far as intra-observer errors are concerned. The aim of the present study was to propose a model that could be implemented by clinicians in their clinical practice.
The maximum percentage of EARR for each patient was analyzed, as this is a clinically more meaningful criteria to evaluate the need for specific treatment proceedings.18 As widely observed in literature, the most frequently affected teeth were maxillary incisors.2,7,12,15 For data analysis, a multiple linear regression model12 was preferred, instead of a logistic one, avoiding the use of the 2mm cut-off for defining pathologic EARR, for which there are no studies setting a correlation with clinical outcome.
Gender, treatment duration, use of Hyrax appliance, anterior open bite and premolar extractions were the main factors that independently contributed to EARR, explaining 28% of its variability. Although overjet contribution was close to statistical significance (P<0.1), each additional score only represented an average increase of 0.1%, which is not clinically relevant.
Gender has also been previously described as a significant predictor of EARR,8,26 and males were found to be more susceptible.26 However, on average, female values were only 3% below male values. In line with our results, some authors have identified treatment duration as a very significant variable predicting EARR1,8,14,26 although others have not.12,18 For each additional year, an average increase of 3.6% was found. Regarding the use of a Hyrax appliance, previous studies had only focused on molar and premolar root resorption. The association we described, between EARR of anterior maxillary teeth and the use of Hyrax appliance has only been reported in animal models27 and may be explained by the tipping that occurs on the maxillary incisors during de palatal expansion, allowing incisors’ root proximity. This interesting finding deserves further research.
According to the results of the present study, in patients who underwent maxillary premolars extractions the percentage of EARR was higher, which is in accordance with the findings of two recent studies8,28 though in disagreement with other authors.26 The amount of EARR could to be related to the distance that canines and incisors are moved. Clinically, after premolar extraction, maxillary canines and incisors retract several millimeters, especially in the case of high incisor protrusion. However, if the space is used to solve teeth crowding, the incisors’ movement is much shorter.
Anterior open bite was also a significant factor for EARR. The same result was achieved in a previous study, which they explained by the association between this morphologic condition and the tongue and lip dysfunction.11 A correlation between root resorption and open bite cases, especially in the hypofunctional teeth, was also found.29 Of the 32 patients with anterior open bite found in our sample, 12 (37.5%) were submitted to maxillary premolars extractions. Yet, patients only with open bite had 26.1% of EARR and those with open bite and premolar extractions had 26.0%, reinforcing that both factors independently contributed to EARR.
The lower predictive power achieved with this model suggests the interference of other factors. Genetic predisposition to EARR has long been suggested2 but as for other complex diseases, it is not clear if a patient's genetic profile will significantly improve risk evaluation. In future research, one even more elusive variable, epigenetics, should be included in this complex interplay.
ConclusionUsing a multiple regression model analysis, five clinical and treatment variables, explaining 28% of External Apical Root Resorption variability, were identified: treatment duration, gender, use of Hyrax appliance, anterior open bite and premolar extractions. The limited impact of these clinical and treatment variables in root resorption suggest the existence of other, probably multiple, low penetrance factors that need to be looked into.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the responsible Clinical Research Ethics Committee and in accordance with those of the World Medical Association and the Helsinki Declaration.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data and that all the patients included in the study have received sufficient information and have given their informed consent in writing to participate in that study.
Right to privacy and informed consentThe authors must have obtained the informed consent of the patients and/or subjects mentioned in the article. The author for correspondence must be in possession of this document.
Conflicts of interestThe authors have no conflicts of interest to declare.