











The head and neck are commonly affected in gunshot injuries and this can cause functional and esthetic defects in the maxillofacial region. Mandibular discontinuity is an important esthetic and functional problem and its reconstruction represents a huge challenge. The opening, closing, lateral and protrusive movements of the mouth are diminished and malocclusion can occur. The purpose is to report a clinical case of a 44 years man who had an immediate loaded implant-supported prosthesis after six months of mandibular reconstruction with free iliac bone grafting of a greatmandibular defect caused by gun shot. Autogenous bone grafting is the most predictable treatment from the available reconstruction options for mandibular bone defects. Reconstructed patients can achieve good results with dental implants and implant-supported prostheses with immediate loading. This treatment can promote better masticatory function, improving the nutrition capacity, facial symmetry, muscular equilibrium, better diction and quality of life.
A cabeça e o pescoço são comumente afetados em lesões por arma de fogo, podendo causar defeitos estéticos e funcionais. Descontinuidade mandibular é um problema estético e funcional importante e a sua reconstrução representa um desafio. A abertura, encerramento, movimentos de lateralidade e protrusão da boca estão diminuídos e uma má oclusão pode ocorrer. O objetivo deste trabalho é relatar o caso de um homem de 44 anos submetido a reconstrução de um defeito mandibular causado por arma de fogo, com enxerto ósseo livre do ilíaco e instalação de prótese implanto-suportada em carga imediata. Enxerto ósseo autógeno é o tratamento mais previsível entre as opções disponíveis para a reconstrução de defeitos mandibulares. Este tipo de reconstrução em pacientes pode obter bons resultados com implantes dentários e próteses com carga imediata. Este tratamento pode promover uma melhor função mastigatória, melhorando a capacidade de nutrição, simetria facial, equilíbrio muscular, melhor dicção e qualidade de vida.
Functional and esthetic defects in the maxillofacial region can be caused by different reasons as trauma, pathologies, congenital or iatrogenic. The head and neck are commonly affected in gunshot injuries. More than 50% of attempted suicides, 14% of assaults, and 12% of accidental injuries occur in this area.1 Mandibular discontinuity is a very important esthetic and functional problem and the reconstruction of these patients represents a very huge challenge. The opening, closing, lateral and protrusive movements of the mouth are diminished and impaired, malocclusion and problems with proprioception can occur.2,3
Autogenous bone is believed to be the “gold standard” for graft procedures. It has a very high osteogenic potential, however, it has a limited availability and the surgical procedures might cause additional morbidity.4–6 Bone grafts taken from the iliac crest have demonstrated to be a very reliable means for the reconstruction of maxillofacial defects after ablation of tumors.7 Non-vascularized bone grafts from the anterior iliac crest offer numerous advantages, such as reliable shape, adequate volume, low donor morbidity, and a distant location from the mandible to facilitate a multiteam approach.8 This kind of bone reconstructions allow not only the adequate facial contour and bone continuity, but also creates an adequate support for the implant placement and implant-supported prosthetic rehabilitations.7–9
The grafting procedure using bone from the anterior iliac crest is less invasive than a free-flap technique, has a good success rate and provides good quality bone for successful osseointegration of dental implants.10,11 The purpose of this article is to report a clinical case of an immediate loaded implant-supported prosthesis after six months of mandibular reconstruction with free iliac bone grafting of a great mandibular defect caused by fire gun shot.
Case reportA 44 years old man attended the Oral and maxillofacial surgery department for treatment of a mandibular bone defect after injury by firearms. He reported an attempt of suicide about 1 year before. On the clinical evaluation, the facial contour was preserved by a reconstruction plate and the panoramic radiograph showed a bone defect without continuity of the left mandibular body. The stabilization of bone segments was maintained by a reconstruction plate of load bearing type (Figs. 1 and 2). The proposed treatment plan was the reconstruction of the mandibular defect using free iliac crest bone and after that, an implant-supported rehabilitation.


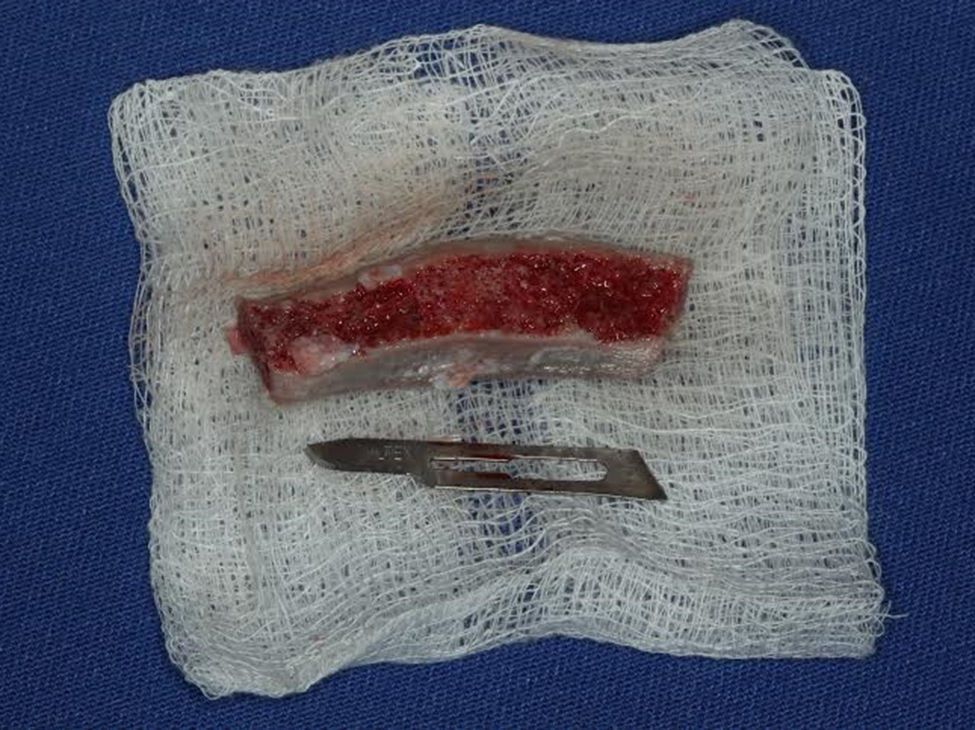
Under general anesthesia, surgery for mandibular reconstruction was performed by submandibular access, location of defect and preparation of the recipient area with small perforations. Then the free block of iliac crest bone was adapted and fixed on the reconstruction plate of 2.4mm (Neo-ortho, Curitiba, PR, Brazil) in the defect area (Figs. 3 and 4). Antibiotics, anti-inflammatories and analgesics were administered during the hospitalization period and mouthwash with chlorhexidine was used as an adjunct to oral hygiene. The patient was discharged 3 days after the surgical procedure and he remained using antibiotics and analgesics for seven days. After six months, the panoramic radiography showed good adaptation of the bone graft. During the period after reconstruction, the patient did not show any signal of infection or pain. The planning for the oral rehabilitation was initiated by the confection of a provisional partial denture. This prosthesis was replicated to fabricate a surgical guide for implant placement (Fig. 5). Morse tapered implants (Drive-Neodent Curitiba-Brazil) were placed following the manufacturer's instructions. All implants achieved primary stability above 45Ncm and the abutments were immediately installed for the provisional hybrid prosthesis transformation (Fig. 6). For it, the titanium cylinders were incorporated in the acrylic partial removable prosthesis using acrylic resin immediately after performing the implant surgery (Figs. 7 and 8). After 12 months of the implant placement, no pain, inflammation or infection in the operated sites was observed and panoramic radiographs showed no radiolucency around the implants (Figs. 9 and 10).
Discussion and conclusions







Anatomical, functional and esthetic aspects have to be carefully analyzed while performing reconstructive surgery. The facial trauma and treatment of jaw tumors can result in bone loss affecting the facial contour, speech and chewing. The reconstruction and rehabilitation of patients who have suffered major defects of facial bones is difficult and challenging. A large free bone reconstruction using bone graft is possible, however, can have greater difficulty of incorporation when compared to vascularized bone grafts.12 It has also been shown that the extension of the defect does not represent a limit to the use of non-vascularized bone grafts.6 Some of the advantages of the non-vascularized iliac bone grafts are large volume, minimal donor site morbidity, shorter surgery and recovery time and no necessity for microvascular surgical expertise.9 The resorption of non-vascularized iliac bone grafts is an important consideration that must be carefully analyzed in the treatment planning of bone reconstruction and dental implant placement.9 Successful bone grafting requires intimate contact between the reminiscent bone and the graft, stability and exclusion of pressure from a removable prosthesis.13 In the present situation, the shape of the iliac graft was sculpted to fit into the mandibular defect and then was fixated using the preexistent 2.4mm reconstruction plate and bicortical screws. After the surgery, the patient was instructed to avoid using his removable prosthesis.
Subsequent to the osseous anatomic reconstruction, the oral and maxillofacial rehabilitation can be completed by the placement of dental implants and implant-supported prosthesis, returning the masticatory function, esthetics and phonetics to the patient. It is an excellent alternative of treatment, promoting better nutrition and also a better diction.7–9 However, the quality of bone tissue is a factor that determines the success of the rehabilitation with dental implants, recent publications have stated good results with the use of dental implants in patients who have undergone bone reconstruction.7–9 Before the implant placement surgery, a healing period of 4–6 months after performing the reconstruction surgery is necessary. This period should not be overextended to prevent graft resorption.6 Another important issue is that the functional loading with implants stimulates the graft and inhibits bone resorption.7,9 This healing period would allow us to verify the incorporation and re-vascularization of the reconstructed area. In the case reported, during the drilling procedure for implant placement it was observed a change in bone density when compared to the bone of origin.
After graft incorporation, the osseous density was improved, increasing an initial stability of the implants during placement. This condition of primary stability provided the immediate loading of the dental implants and anticipation of the masticatory function of the patient, improving the nutrition capacity, facial symmetry, muscular equilibrium and quality of life. The hybrid prosthesis has shown a passive fit in the mouth and the single screw test14 was performed to confirm it. The passive fit, the tripod configuration, the unilateral extension and the lack distal cantilever of the prosthesis probably helped to prevent biomechanical problems such as screw fractures or screw loosening. Clinical evaluation of the patient after 12 months showed normal aspects. The appearance of the mucosa was satisfactory and the implants were tested individually after retrieving the prosthesis and all were stable after surgery, they were clinically evaluated and demonstrated no mobility, bone loss, or clinical signs of infection. Radiologic examinations confirmed the normal condition of the bone segments and all the implants.
Autogenous bone grafting produce is the most predictable treatment modality from the available reconstruction options for mandibular bone defects and missing segments. In reconstructed patients, good results can be achieved with the use of dental implants and implant-supported prostheses with immediate loading. This alternative of treatment can promote better masticatory function of the patient, improving the nutrition capacity, facial symmetry, muscular equilibrium, better diction and also quality of life.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interestThe authors have no conflicts of interest to declare.