




There is an increasing amount of evidence showing that physical activity and sun exposure are effective coadjuvant treatments for patients with mild to moderate depression. However, there is a lack of information regarding patient's adherence to these recommendations in daily clinical practice.
MethodsWe conducted a study including 15 depressive patients who had been under antidepressant treatment for at least one month. They wore a wrist-watch-like actimetry sensor to measure physical activity and sun exposure 24h a day. After one week of baseline assessment, patients were randomized into one of the two arms of the study. Patients in the experimental group received a brief note in which they were explicitly asked to increase both their physical activity level and time of sun exposure, while control group patients did not receive these explicit recommendations.
ResultsOne week after recommendations were delivered, only patients in the experimental group had increased time of sun exposure and physical activity (25.8% and 14.3%, respectively).
ConclusionsDepressive patients are able to follow prescribed lifestyle recommendations in the short-term.
La práctica de ejercicio físico y la exposición a la luz solar cada vez tiene mayor respaldo experimental sobre su eficacia antidepresiva coadyuvante en pacientes con depresión leve o moderada. Sin embargo, no hay información objetiva disponible sobre el grado de adherencia que los pacientes depresivos son capaces de desarrollar frente a estas recomendaciones en condiciones de práctica habitual, lo que limita la tendencia del clínico a prescribirlas.
MétodosSe estudia una muestra de 15 pacientes con un episodio depresivo de más de un mes de evolución con tratamiento antidepresivo a los que se les colocó un actígrafo en forma de reloj de pulsera capaz de medir la actividad física y la exposición a la luz durante las 24 horas del día. Una semana después de la evaluación basal estos pacientes fueron aleatorizados en 2 grupos. En el primero de ellos se les pedía en una breve nota por escrito de forma explícita y concreta que aumentaran la actividad física y la exposición a la luz solar, mientras que en el segundo grupo no.
ResultadosEn la semana posterior a la entrega de las recomendaciones, solo el primer grupo aumentó su actividad física y su exposición a la luz (14,3 y 25,8% respectivamente).
ConclusiónLos pacientes con depresión muestran un buen nivel de adherencia a recomendaciones sobre su estilo de vida a corto plazo.
Depression is a very prevalent, incapacitating illness, with high chronification rates. The treatments of choice available (psychotherapy and drug therapy) do not always manage to achieve complete remission of the symptoms or prevent its relapses or recurrences. For that reason, it is still necessary to investigate new adjuvant therapeutic antidepressant alternatives, especially if they can add efficacy to the treatment without reducing tolerance and safety.1
In the last few years, data have been growing about the usefulness of having patients who are depressed make specific changes in their lifestyles.2,3 For example, moderate physical exercise is capable of contributing to improvements in depressed patients, to the point that it is now being included in some clinical guidelines.4,5 In addition, while it has been known for years that light therapy is the treatment of choice for seasonal affective disorder, it is now being shown that including sunlight exposure can be of use in non-seasonal depression as well.6,7
Adherence to treatment is a fundamental problem in treating depression, as much in its psychopharmacological aspects as in its psychotherapeutic ones. The degree of adherence to this other type of recommendations based on lifestyle changes is, to a great extent, unknown. It has been suggested that it could be very low, given that the presence of depressive symptoms constitutes one of the main barriers when lifestyle changes are recommended to patients with medical illnesses.8 However, there are no studies that focus specifically on samples of patients with depression. That may be why many centers are sceptical about how pertinent it is to make these recommendations to patients in the acute phase of depression. This study represents an objective assessment in a pilot experiment of whether patients with a depressive episode are capable of increasing, at least in the short term, their levels of physical activity and sun exposure when these are prescribed as a therapeutic recommendation adjuvant to their normal antidepressant treatment.
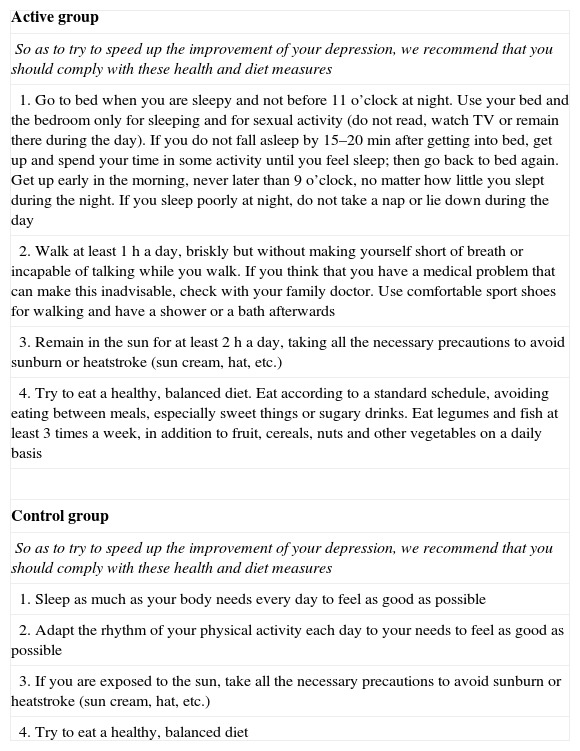
Materials and methodsWe recruited 15 patients older than 18 years with a depressive episode (major depression, dysthymia or bipolar disorder in the depressive phase, according to the DSM-IV). The diagnoses were confirmed with the MINI scale and the level of seriousness was assessed with the Hamilton Depression Rating Scale and the Beck Depression Inventory. The patients had been in antidepressant treatment for at least 1 month and they committed to continuing it during the study. Patients at significant risk of suicide or with other psychiatric or medical problems that would make their participation difficult were excluded. The patients recruited formed part of a multi-center clinical trial whose objective was to assess the efficacy of health and diet recommendations for depressed patients and whose protocol had been registered (ISRCTN59506583) and published.1 The recommendations that the patients received are presented in Table 1. This study was approved by the local ethics committee in writing after being informed of its characteristics. We had 4 actigraph devices that were allotted as they became available immediately after being used by the previous patients. The devices were worn on the wrist of the non-dominant arm for the 2 weeks that the study lasted. We asked the patients not to take the device off except for having a bath or shower and to prevent it from being covered by their clothes. The model used was the Actiwatch Light AWL (dimensions 37mm×29mm×10mm; 17g; Cambridge Neurotechnology Ltd.), configured for a sample interval of 1min. The actigraph detected and measured the movements that exceeded 0.01g (the force of gravity per minute). In addition, the photoconductive cell registered the levels of exposure to light in lux (1lx: full moon night; 32,000lx: sunlight on an average day). The averages for daily physical activity and sun exposure were registered; days on which the patients put on and took off the Actiwatch were ignored (as incomplete), as well as the day on which patients received the written recommendation. In most of the cases, it was possible to obtain complete data for 7 days before and 7 days after receiving recommendations.
Recommendations given to the patients.
| Active group |
| So as to try to speed up the improvement of your depression, we recommend that you should comply with these health and diet measures |
| 1. Go to bed when you are sleepy and not before 11 o’clock at night. Use your bed and the bedroom only for sleeping and for sexual activity (do not read, watch TV or remain there during the day). If you do not fall asleep by 15–20min after getting into bed, get up and spend your time in some activity until you feel sleep; then go back to bed again. Get up early in the morning, never later than 9 o’clock, no matter how little you slept during the night. If you sleep poorly at night, do not take a nap or lie down during the day |
| 2. Walk at least 1h a day, briskly but without making yourself short of breath or incapable of talking while you walk. If you think that you have a medical problem that can make this inadvisable, check with your family doctor. Use comfortable sport shoes for walking and have a shower or a bath afterwards |
| 3. Remain in the sun for at least 2h a day, taking all the necessary precautions to avoid sunburn or heatstroke (sun cream, hat, etc.) |
| 4. Try to eat a healthy, balanced diet. Eat according to a standard schedule, avoiding eating between meals, especially sweet things or sugary drinks. Eat legumes and fish at least 3 times a week, in addition to fruit, cereals, nuts and other vegetables on a daily basis |
| Control group |
| So as to try to speed up the improvement of your depression, we recommend that you should comply with these health and diet measures |
| 1. Sleep as much as your body needs every day to feel as good as possible |
| 2. Adapt the rhythm of your physical activity each day to your needs to feel as good as possible |
| 3. If you are exposed to the sun, take all the necessary precautions to avoid sunburn or heatstroke (sun cream, hat, etc.) |
| 4. Try to eat a healthy, balanced diet |
The statistical study was performed using the program SPSS Version 19, carrying out a descriptive analysis and a comparison of means. Given the small sample size, we used non-parametric tests (Mann–Whitney and Wilcoxon).
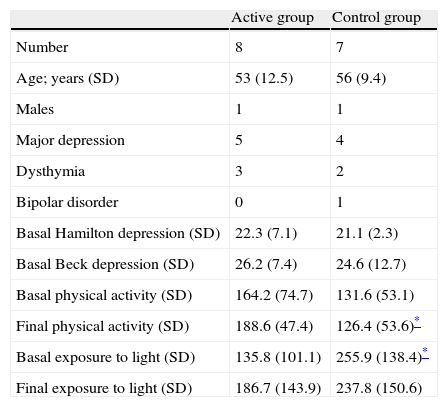
ResultsThe main sociodemographic and clinical data for the patients are presented in Table 2. The means for physical activity and sun exposure are also included for each treatment group, for both the 7 days prior to and 7 days after receiving the recommendations. Given the small sample size and the wide inter-individual variability of these measurements, which also depended on the seasons with their different hours of light, we could see an imbalance between groups in the basal measurements for physical activity and sun exposure. For that reason, we used percentages of decrease with respect to the basal measurement to compare the changes between groups. Consequently, it was possible to establish that there was a clear difference between groups at the end of the study with respect to the basal situation, which was in line with our study hypothesis. Indeed, the physical activity and sun exposure increased 14.3% and 25.8%, respectively in the active group, while the same parameters were −15.8% and −26.9% for the control group. However, the statistical contrast was not significant. What was demonstrated was that, for the active treatment group, the sun exposure level rose from the basal level (135.85 vs 186.75; P=.046). The increase in physical activity (164.22 vs 188.69; P=.194) indicated only a tendency that was not statistically significant (see Table 1). There was no correlation between the degree of adhesion and the seriousness of the depression measured on the scales.
Clinical and sociodemographic data.
| Active group | Control group | |
| Number | 8 | 7 |
| Age; years (SD) | 53 (12.5) | 56 (9.4) |
| Males | 1 | 1 |
| Major depression | 5 | 4 |
| Dysthymia | 3 | 2 |
| Bipolar disorder | 0 | 1 |
| Basal Hamilton depression (SD) | 22.3 (7.1) | 21.1 (2.3) |
| Basal Beck depression (SD) | 26.2 (7.4) | 24.6 (12.7) |
| Basal physical activity (SD) | 164.2 (74.7) | 131.6 (53.1) |
| Final physical activity (SD) | 188.6 (47.4) | 126.4 (53.6)* |
| Basal exposure to light (SD) | 135.8 (101.1) | 255.9 (138.4)* |
| Final exposure to light (SD) | 186.7 (143.9) | 237.8 (150.6) |
No relevant problems were found with respect to tolerance and there were no incidents related with safety.
DiscussionThe Mediterranean lifestyle has been linked to the positive health indicators enjoyed by the countries in southern Europe.9 Within the “ingredients” of the Mediterranean lifestyle are diet, physical exercise, control of stress and high social support level, as well as spending more time outside in the fresh air and exposure to sunlight, all of these factors being favored by the normally pleasant climate.10 Unfortunately, we are witnessing a slow but inexorable loss of these lifestyle patterns. The doubt arises as to whether this is an inevitable and irreversible phenomenon, due to what is known as “globalization”. At least in medicine, it seems not, to the extent that it has been shown that patients affected by different, prevalent and serious neurological, metabolic and cardiovascular illnesses can improve their life expectancy significantly when they modify aspects of their lifestyle.10–13 Depression might very well be added to this group of illnesses, given that we know that there is a bidirectional relationship between depression and poor eating habits, a sedentary lifestyle, disordered circadian rhythms and exposure to sunlight.14 Nevertheless, health and diet treatment have still not been accepted as a necessary component of the therapeutic plan for depressed patients in a general way, although many clinics have certainly been giving recommendations for many years based on their intuition and experience. One of the reasons for the lack of use of lifestyle recommendations in depression might be the justified doubts as to adherence to these measures.15 It is true that psychomotor delay is a key obstacle, as well as anhedonia, anergy, abulia, withdrawal, despair and somatic and psychic anguish. Obstacles can also be found in other depressive symptoms, such as memory and concentration problems, multiple corporal discomforts and lack of interest in appearance and health. All of these increase the difficulties involved in having patients change specific behavior related to their lifestyle in the manner in which they are asked. On the other side of the scales, we have the good recognition of illness and proper collaboration of patients with depression, especially if it is not excessively serious and the patients are capable of convincing themselves that it is worth the effort. The results of our study point to the fact that patients with mild or moderate depression do increase physical activity and exposure to light after receiving recommendations to do so, at least in the following week. However, it is noteworthy that the control group's decrease in the measurements of physical activity and light exposure was of a magnitude similar to the active group's increase. It is possible that the control group did not interpret the recommendations given to them as neutrally as intended (see Appendix 1). That is, when control group patients were asked to increase the rhythm of their physical activity and their hours of sleep to their needs, in order to feel as good as possible, and that they should protect themselves from the sun if they were exposed to it, this might have led them to do less physical activity, go out of the house less or sleep more. At any rate, we have to mention that, due to the limited sample, caution must be used in reaching conclusions on events that are perhaps chance circumstances or that at least do not have statistical support. Consequently, we feel that there are aspects of this project that deserve to be investigated better with a wider sample. For example, further research should be carried out on whether it is preferable or not for the control group to receive recommendations, and on the strategies for increasing motivation and adherence. It would also be important to ascertain the extent to which the patients are capable of maintaining their adherence in the 3–6 months afterwards.
In summary, in spite of its limitations, this pilot study suggests that providing a simple sheet of paper with recommendations on lifestyle to patients with depression is enough for them to make an effort to follow the recommendations, at least in the short term.
Ethical disclosuresProtection of human and animal subjects. The authors declare that the procedures followed conform to the ethical regulations of the committee responsible for human subject experimentation and are in agreement with the World Medical Association and the Helsinki Declaration.
Confidentiality of data. The authors declare that they have followed the protocols of their work center on the publication of patient data and that all of the patients included in the study have received sufficient information and have given their informed consent in writing to participate in this study.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Conflict of interestThe authors have no conflict of interest to declare.
We extend our thanks to all the patients and doctors at Ib-Salut that collaborated in this project, to the Instituto Carlos III for its funding (FIS no. PI07 0544) and to the Hospital Son Llàtzer, the FUE and the UIB, which permitted its implementation thanks to their collaboration agreement.
Please cite this article as: García-Toro M, et al. Adherencia a las recomendaciones sobre estilo de vida en pacientes con depresión. Rev Psiquiatr Salud Ment (Barc.). 2012;5:236–40.