




Attention deficit–hyperactivity disorder (ADHD) is a common neuropsychiatric disorder in adulthood. Its diagnosis requires a retrospective evaluation of ADHD symptoms in childhood, the continuity of these symptoms in adulthood, and a differential diagnosis. For these reasons, diagnosis of ADHD in adults is a complex process which needs effective diagnostic tools.
AimTo analyse the criterion validity of the CAADID semi-structured interview, Spanish version, and the concurrent validity compared with other ADHD severity scales.
MethodsAn observational case-control study was conducted on 691 patients with ADHD. They were out-patients treated in a programme for adults with ADHD in a hospital.
ResultsA sensitivity of 98.86%, specificity 67.68%, positive predictive value 90.77% and a negative predictive value 94.87% were observed. Diagnostic precision was 91.46%. The kappa index concordance between the clinical diagnostic interview and the CAADID was 0.88. Good concurrent validity was obtained, the CAADID correlated significantly with WURS scale (r=0.522, P<.01), ADHD Rating Scale (r=0.670, P<.0.1) and CAARS (self-rating version; r=0.656, P<.01 and observer-report r=0.514, P<.01).
ConclusionCAADID is a valid and useful tool for the diagnosis of ADHD in adults for clinical, as well as for research purposes.
El trastorno por déficit de atención/hiperactividad (TDAH) es un trastorno neuropsiquiátrico frecuente en la edad adulta. Su diagnóstico requiere realizar una evaluación retrospectiva de los síntomas durante la infancia, evaluar la continuidad de los mismos en la edad adulta y realizar un diagnóstico diferencial. Por estos motivos, el diagnóstico de TDAH en adultos supone un proceso complejo que precisa de instrumentos de evaluación efectivos.
ObjetivoAnalizar la validez de criterio de la versión española de la entrevista semiestructurada CAADID y la validez de concurrente comparándola con escalas de gravedad del TDAH.
MétodoSe realizó un estudio observacional de casos y controles en el que participaron un total de 691 sujetos, evaluados a nivel ambulatorio en el marco de un programa especializado en el TDAH de adultos
ResultadosSe observó una sensibilidad del 98,86%, una especificidad del 67,68% un valor predictivo positivo del 90,77% y un valor predictivo negativo 94,87% La precisión diagnóstica fue de 91,46%. El índice de concordancia Kappa entre el patrón oro (entrevista clínica abierta) y la CAADID fue de 0,74. La validez concurrente reflejó una correcta correlación con la escala WURS (r=0,522 p<0,01), con la ADHD Rating Scale (r=0,670 p<0,01) y con la CAARS tanto en su versión autoreportada (r=0,656 p<0,01) como en la del observador (r=0,514 p<0,01).
ConclusionesLa CAADID es una herramienta diagnóstica válida y útil para evaluar el TDAH en adultos siendo de utilidad para la práctica clínica diaria y en el ámbito de la investigación.
Attention deficit–hyperactivity disorder (ADHD) is a neuropsychiatric disorder characterised by the presence of a persistent pattern of inattention and/or hyperactivity and impulsivity. It is considered a chronic disorder, which begins in childhood and continues in adulthood in over 50% of the cases.1 Prevalence in children is estimated to be approximately 5%2,3 and in adults, some 2–4%.4,5
Both in adults and children, ADHD has been associated with a general pattern of problems in academic achievement and social, family and work adaptation, generating elevated healthcare and economic costs.6 In spite of the negative repercussions on different areas that ADHD produces in adult patients and of having effective treatment for it available,7–9 it is still an underdiagnosed disorder that is scarcely treated. Only approximately 11% of the adults with ADHD receive treatment.10 In our environment, less than 0.5% of the general adult population get drug treatment for ADHD.11
Diagnosis of ADHD in adults, just as in childhood, is based on the medical history, searching for the presence of symptoms of hyperactivity, attention deficit and impulsivity throughout life. It is necessary to perform a retrospective diagnosis of the symptoms during childhood and assess their continuity in adulthood.12 There are presently no reliable diagnosis methods, such as neuroimaging or neuropsychological tests.7,13 Despite the similarity between the disorder in childhood and adulthood, the clinical signs and symptoms can change with the patient's age. For example, the outward hyperactivity of the child with ADHD usually appears in the adult as a sensation of psychomotor restlessness or of an internal motor.12 Furthermore, a differential diagnosis with other pathologies that have similar clinical pictures should be performed. For these reasons, effective assessment tools are needed for ADHD diagnosis in adults.
Different studies have assessed the psychometric properties of the Spanish versions of scales used to assess ADHD in adults; however, these tools are self-administered (the patients themselves are the ones who evaluate the presence and intensity of the symptoms), without being able to assign a definite diagnostic value.14–16 Sensitivity and specificity have also been studied in the retrospective detection of childhood ADHD symptoms in adults that consulted due to clinical ADHD signs and symptoms, through a semi-structured interview based on DSM-III-R criteria.17 The results showed that it is possible to assess childhood ADHD symptoms with precision from the information provided by adults with ADHD. In contrast, there are no studies that examine the criterion validity for semi-structured interviews in Spanish for diagnosing ADHD in adults.
The Conners’ Adult ADHD Diagnostic Interview for DSM-IV (CAADID)18 is a semi-structured, mixed interview consisting of 2 sections. Each part is designed to provide information needed to make a clinical determination on the presence or absence of the disorder. Part i collects information on the following areas: (1) demographic history, (2) psychomotor development, (3) risk factors for ADHD and (4) psychiatric comorbidity. This part of the interview can be filled in by the patient or by a clinician, while Part ii (designed to assess the DSM-IV criteria that define ADHD) should be administered by a trained clinician.19The validity and reliability of ADHD diagnosis provided by the CAADID (English version) were studied in a 30-patient sample, evaluating the simultaneous validity between the current and the childhood ADHD symptoms.19 The results suggest that the CAADID is a tool with appropriate reliability and test–retest consistency for diagnostic judgements. This interview has been used in research widely, in both clinical trials and in genetics.20–23
Validating the Spanish version of a semi-structured interview in agreement with the DSM-IV criteria would make a precise diagnostic tool for assessing ADHD in adults available. This would be useful for daily clinical practice and in the research environment.
The main objective of our study was to analyse the criterion validity of the Spanish version of the semi-structured interview CAADID Part ii (Conners’ Adult ADHD Diagnostic Interview for DSM IV).18 The second study objective was to examine the concurrent validity of the CAADID, comparing it with ADHD severity scales. This was the first study carried out with the goal of validating the Spanish version of this interview.
Material and methodsParticipantsThis was an observational, case-control study in which 691 subjects participated, with outpatient assessment in the framework of a specialised programme for ADHD in adults at a tertiary university hospital. This is a programme for assessment, diagnosis and comprehensive treatment is carried out for adult patients with ADHD, referred from primary health centres, child psychiatry consultations, mental health centres and centres for drug abuse attention when a diagnosis of ADHD is suspected. This study was approved by the ethical committee of the hospital and all of the subjects signed the corresponding informed consent.
The criteria for inclusion in the study were having an age equal to or greater than 18 years and less than 65 years, and presenting appropriate capacity for granting and signing the corresponding informed consent. The criteria for exclusion were presenting an intellectual quotient lower than 70 or presenting symptoms of intoxication due to psychotropic substances.
ToolsTo study the criterion validity of the CAADID, its results were compared with an open interview carried out in the first phase of the study. Through the open interview, we registered the presence of symptoms according to the DSM-IV criteria (Criterion A), the age at symptom onset (Criterion B), the presence of symptoms in 2 or more areas (Criterion C), the deterioration caused by the symptoms during childhood and adulthood (Criterion D) and the fact that the symptoms could not be explained better by another disorder (Criterion E).
When administering the CAADID, the interviewer should perform a clinical determination as to the presence or absence of each symptom and to the rest of DSM-IV criteria for the disorder, based on the information provided by the patient and an observer that has known the patient from childhood. For each symptom, the CAADID gives examples of typical behaviour related with the symptom, which the interviewer can use to detect its presence or absence.
To analyse the concurrent validity of the CAADID, the diagnosis provided by administering it was compared with the following scales:
- •
Wender Utah Rating Scale (WURS)24: a self-administered 61-item scale, with good internal consistency and temporal stability. The adults need to remember the symptoms from their own childhood retrospectively. Each symptom is scored from 1 to 4. Of the 61 items, 25 present greater empirical validity to discriminate ADHD versus non-ADHD.
- •
ADHD Rating Scale25: 18-item scale that evaluates ADHD diagnostic criteria according to the DSM-IV. Each of the items is scored from 0 («Never or almost never») to 3 («Very frequently») and serves to determine the presence and intensity of each of the symptoms. This questionnaire can be administered to either the patient or a close relative.
- •
Conners Adult ADHD Rating Scale (CAARS)26: This is a scale consisting of 6 questionnaires, 3 of which are self-reported and 3 completed by an observer, in which item is scored from 0 («Never») to 3 («Very frequently»). The number of items in each scales depends on the version:
- •
Long Versions (66 items): self-reported (CAARS-S:L) and observer (CAARS-O:L) forms.
- •
Short Versions (26 items): self-reported (CAARS-S:S) and observer (CAARS-O:S) forms.
- •
Screening Version (30 items): self-reported (CAARS-S:SV) and observer (CAARS-O:SV) forms.
The initial step was the conceptual translation of the English version to Spanish, according to the regulations designed and approved by the business holding the interview copyright (Multi-Health System).
When we had the Spanish translation, the first stage consisted of administering an open interview to assess ADHD according to the DSM-IV criteria. The DSM-IV was our gold standard, as there was no other interview validated in Spanish for adults. We obtained 527 subjects from the sample total that fulfilled diagnostic criteria for ADHD. The remaining 164 subjects constituted the control group, given that they did not fulfil these ADHD diagnostic criteria.
In the second stage, all the study subjects were administered, using a second professional, the assessment protocol from the ADHD Programme.27 In the first visit of this stage, the Spanish version of the semi-structured CAADID parts I and II18 to assess the ADHD diagnosis in childhood and in adulthood was used. The interview was complemented with the information provided by the patients and by that obtained from a relative or person who had known them since childhood. If there was a discrepancy between the relative and the patient, the centre evaluated the presence or absence of symptoms based on the entire case history. The diagnostic threshold for determining presence of the disorder in adulthood was placed at 6 or more symptoms at the current moment of inattention and/or hyperactivity-impulsivity, as specified by DSM-IV Criterion A. The symptoms have to appear before the patient is 7 years old (Criterion B), be present in at least 2 domains (Criterion C) and present a functional deterioration as a consequence of the symptoms (D). In the second and third visits, the differential diagnosis with other psychiatric disorders was carried out using the Structured Clinical Interviews I and II for DSM-IV (SCID I and II)28,29 in order to evaluate DSM-IV Criterion E.
The intensity of the ADHD symptoms were assessed with various scales: the self-administered and observer long versions of the Conner's ADHD Rating Scale (CAARS-S:L, CAARS-O:L),26 the ADHD Rating Scale (ADHD-RS)25 and lastly, the Wender Utah Rating Scale (WURS)24 for the retrospective childhood symptoms. The level of deterioration was assessed with the Clinical Global Impression (CGI) scale30 and the Sheehan Disability Scale.31 Intellectual quotient (IQ) was estimated from the Vocabulary and Block Design, Wechsler Adult Intelligence Scale-3rd Edition (WAIS-III).32 All of the patients were assessed by psychiatrists and clinical psychologists with experience in ADHD diagnosis in adults and in administration of the CAADID.
We compared the results from the CAADID with the clinical diagnosis (gold standard), obtained from the open interview. To reduce possible bias, the centre that administered the open interview was always different from the one that assessed the patient with the CAADID. In addition, both professionals were blind with respect to the diagnosis obtained through the other colleague's interview. The results from the CAADID were compared with the scores on the WURS, ADHD-RS and CAARS scales.
Statistical analysisWe determined the criterion validity of the CAADID using analyses of Sensitivity (percent of affected cases identified by the test), Specificity (percent of the non-affected identified by the test), Positive Predictive Value (percent of the affected that obtain a positive assessment in the test) and Negative Predictive Value (percent of the non-affected cases that obtain a negative assessment in the test). All of these estimations were accompanied by their corresponding confidence intervals. This information was complemented with the kappa value as a general measure of concordance. We performed bivariate correlations for the concurrent validity analysis. In all of the cases, the statistical hypotheses were bivariate and the confidence level was 95%.
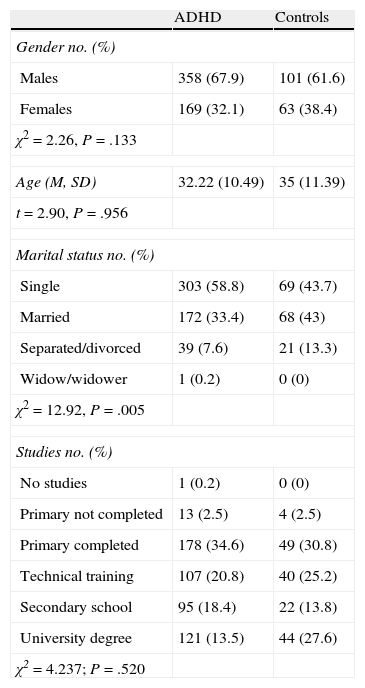
ResultsThe socio-demographic characteristics of the subjects in the study showed a greater participation of males (n=459, 66.4%), with a mean age of between 32 and 35 years. As for marital status, the majority of the subjects were single, with statistically-significant differences between the ADHD and control groups (χ2=12.92, P=.005). Those diagnosed with ADHD presented lower university training, but there were no overall differences between the 2 groups in academic background (see Table 1).
Socio-demographic characteristics of the sample.
| ADHD | Controls | |
| Gender no. (%) | ||
| Males | 358 (67.9) | 101 (61.6) |
| Females | 169 (32.1) | 63 (38.4) |
| χ2=2.26, P=.133 | ||
| Age (M, SD) | 32.22 (10.49) | 35 (11.39) |
| t=2.90, P=.956 | ||
| Marital status no. (%) | ||
| Single | 303 (58.8) | 69 (43.7) |
| Married | 172 (33.4) | 68 (43) |
| Separated/divorced | 39 (7.6) | 21 (13.3) |
| Widow/widower | 1 (0.2) | 0 (0) |
| χ2=12.92, P=.005 | ||
| Studies no. (%) | ||
| No studies | 1 (0.2) | 0 (0) |
| Primary not completed | 13 (2.5) | 4 (2.5) |
| Primary completed | 178 (34.6) | 49 (30.8) |
| Technical training | 107 (20.8) | 40 (25.2) |
| Secondary school | 95 (18.4) | 22 (13.8) |
| University degree | 121 (13.5) | 44 (27.6) |
| χ2=4.237; P=.520 | ||
In terms of criterion validity, using the presence of 6 or more symptoms at the current moment of inattention and/or hyperactivity-impulsivity as the cut-off point, we obtained values for sensitivity of 98.86% (95% confidence interval [CI], 97.41–99.54%), specificity of 67.68% (95% CI, 59.88–74.65%), positive predictive value of 90.77% (95% CI, 88.02–92.95%) and negative predictive value of 94.87% (95% CI, 88.71–97.90%). The diagnostic accuracy was 91.46% (95% CI, 80.06–93.39%). The kappa concordance index between the gold standard (open clinical interview) and the CAADID was 0.74.
Concurrent validitySymptoms of attention deficit with hyperactivity in childhood1. ADHD symptoms in childhood:
- WURS: We assessed the childhood ADHD symptoms that were collected using CAADID, correlating these symptoms with the results of the WURS. The correlation between the WURS results and the symptoms of inattention and hyperactivity in childhood reported by the interview was significant for both symptom clusters (symptoms of inattention, r=0.37, P<.01; symptoms of hyperactivity, r=0.46, P<.01; and total symptoms, r=0.52, P<.01).
2. Current ADHD symptoms:
We assessed the adult ADHD symptoms collected using the CAADID, correlating them with the results of the self-administered patient and observer scales.
- ADHD Rating Scale: The correlation between the results of the self-administered Rating Scale and the ADHD symptoms collected using Part ii of the CAADID was significant for the inattention and hyperactivity symptom clusters (symptoms of inattention, r=0.59, P<.01; symptoms of hyperactivity, r=0.70, P<.01; and total symptoms r=0.67, P<.01).
- Conners’ Adult ADHD Rating Scale (CAARS):
- •
Self-reported version (CAARS S-L): A significant correlation was observed when the association between the interview and the patient CAARS S-L self-reports with the CAARS S-L in the 3 groups of symptoms: r=0.601, P<.01 in inattention; r=0.699, P<.01 in hyperactivity; and r=0.656, P<.01 in total symptoms.
- •
Observer version (CAARS O-L): The results in this case were similar to those obtained with the patient self-administered scale, as there was a statistically significant correlation (symptoms of inattention, r=0.42, P<.01; symptoms of hyperactivity, r=0.58, P<.01; and total symptoms, r=0.51, P<.01).
The objectives of this study were to analyse the criterion validity and the concurrent validity of the Spanish version of the semi-structured clinical CAADID Part ii for the diagnosis of ADHD in adults. The results show that the Spanish version of the CAADID is a tool that possesses sufficient characteristics at the level of criterion and concurrent validity to be used in the diagnosis of ADHD in adults. Our study is the first one to assess the psychometric properties of a semi-structured interview in Spanish for the diagnosis of ADHD in adults.
The results showed a diagnostic accuracy of 91.46% and a kappa index of concordance with the gold standard of 0.74. The concurrent validity study reflected correct correlation with respect to the WURS in assessing childhood ADHD, with a value of r=0.522, P<.01 for total symptoms. Likewise, the concurrent validity was also optimum in assessing the current adult symptoms with respect to the ADHD Rating Scale and the CAARS. The correlation between the CAADID and the ADHD Rating Scale for total ADHD symptoms in adulthood showed significant results (r=0.670, P<.01). The same was true for the CAARS in both its self-reported version (r=0.656, P<.01) and that of the observer (r=0.514, P<.01) for the total ADHD symptoms in adulthood.
Our results with the Spanish version of the CAADID are in line with those obtained by previous studies19 using the English version of the interview.
The results of this study are also congruent with those of other previous studies26,33–38 in which good predictive value was observed between the diagnosis obtained using a structured interview and that provided by self-reported questionnaires, in childhood as well as adulthood.
The main advantage of the CAADID is that it makes it possible to assess in depth the ADHD symptoms during both childhood and adulthood. In addition, it adapts the definition of childhood hyperactivity symptoms to adulthood. It also provides a series of examples that help to assess better the presence of each of the symptoms of the disorder, with the examples being adapted for childhood and adulthood.
However, 2 of the symptoms of adult hyperactivity (restlessness and sensation of an internal motor) are defined differently from how the DSM-IV defines them, in an attempt to reflect the changes in symptoms that ADHD undergoes with age. This fact can cause differences. CAADID results are compared with those of the gold standard (DSM-IV criteria).
Nevertheless, the fact that the interview attempts to adapt childhood symptoms to those of adulthood makes it easier to detect ADHD in adults, given that the DSM-IV symptoms are excessively restrictive for diagnosis in adults, as various authors have suggested.5,39 Despite children and adults sharing many clinical characteristics, the field studies that led to the ADHD criteria for the DSM-IV were performed with child populations and did not include adult samples. Consequently, the symptoms are not adapted to the clinical reality of adults.Having a semi-structured interview in Spanish available to assess the symptoms of ADHD in adults in depth can allow us to improve ADHD detection in clinical contexts. In addition, it can make research in adult domains easier, given that administering the CAADID lets us define groups that are more homogeneous and better limited clinically. Not in vain, it is one of the diagnostic interviews of ADHD in adults most widely used in research.19 In this sense, the CAADID has been utilised in clinical trials22 and in basic research with good results.27,40–42
In the area of research, another tool used for diagnosing ADHD in adults is the ADHD module of the K-SADS.43–46 This methodology limits the detection of adult cases of ADHD, because it is an interview validated in child populations and the symptoms are not adapted to the clinical characteristics of adults. It does not follow the DSM-IV criteria. However, one limitation of the CAADID is that publishing costs have to be paid to use it; in contrast, this is not true of the K-SADS interview,43 which is freely available.
The results from this study should be interpreted taking into consideration a series of limitations that it presents. The patients who are sent to the PIDAA (specialised programme for ADHD in adults) at the Hospital Universitari Vall d’Hebron arrive with an existing suspicion of ADHD, so our sample is one in which there are greater possibilities for detecting the disorder. In this context CAADID specificity was low (67.68%). Sensitivity and specificity make it possible to assess the validity of the test and what a low specificity tells us is that it detects healthy individuals (non-cases) poorly. There is a good chance that a healthy individual would obtain a positive result in the test, as the low specificity indicates. This limitation should be especially taken into consideration in expert witness situations. Another point is that it would be advisable to observe CAADID properties in the general population or in programmes focused on other psychiatric problems (bipolar disorder, personality disorders, etc.) and observe its psychometric properties. One of the limitations attributed to the CAADID, and to the other semi-structured interviews, is the administration time it requires (approximately an hour), which can condition its use outside the research environment.
In conclusion, the results of the present study indicate that the CAADID interview presents good properties at the level of criterion validity and concurrent validity.
Ethical disclosuresProtection of humans and animals. The authors declare that the procedures followed conform to the ethical standards of the responsible committee of human experimentation and are in agreement with the World Medical Association and the Helsinki Declaration.
Data confidentiality. The authors declare that they followed all the protocols of their work centre on the publication of patient data and that all patients included in the study received sufficient information and gave their written informed consent to participate in this study.
Right to privacy and informed consentThe authors obtained the informed consent of the patients and/or subjects referenced in the article. This document is in the power of the corresponding author.
Conflict of interestThe authors have no conflict of interest to declare.
Please cite this article as: Ramos-Quiroga JA, et al. Validez de criterio y concurrente de la versión española de la Conners Adult ADHD Diagnostic Interview for DSM-IV. Rev Psiquiatr Salud Ment (Barc). 2012;5:229–35.