




Improvement in mental health care services is going through a greater involvement of people with mental disorders and their families. Our aim was to directly ask the opinion of people with psychosis and their caregivers about their needs and preference for treatment.
MethodsThe authors designed an anonymous survey containing 9questions about their needs or suggestions on different areas such as personal and social dimensions of the illness, medical and psychotherapeutic treatment, psychosocial rehabilitation or help received from professionals. A pilot study was done to ensure the adequacy and intelligibility of the form. The final survey consisted of 5.205 completed surveys were collected, corresponding to 2.840 people diagnosed with psychotic disorder (including schizophrenia) and 1.341 caregivers, from all over Spain.
ResultsThe most important need as assessed by participants was emotional support (friendships, partner, family). 91% of patients indicated that this need was “quite” or “very important”. Both people with schizophrenia and caregivers perceived their health to be poor (3.29 and 3.30 respectively on an ascending scale from 0 to 5). 43% of males and 39% of females reported having “little” or “no” freedom to make important life decisions. For 35% of participants the psychotherapeutic treatment was instituted too late. Work was “important” or “very important” for 74% of respondents, especially for young people. The most valued anti-stigma initiative was to increase investments in schizophrenia healthcare plans.
ConclusionsDesigners of mental health care services should consider the importance given by people diagnosed with psychosis to emotional needs, perception of freedom to make choices and early intervention.
La mejora en los servicios de atención de salud mental pasa por una mayor participación de las personas con trastornos mentales y sus familias. Nuestro objetivo fue preguntar directamente la opinión de las personas con psicosis y sus cuidadores sobre sus necesidades y preferencias de tratamiento.
MétodosLos autores diseñaron una encuesta anónima que contenía 9 preguntas sobre sus necesidades o sugerencias en diferentes áreas, como las dimensiones personales y sociales de la enfermedad, el tratamiento médico y psicoterapéutico, la rehabilitación psicosocial o la ayuda recibida de profesionales. Se realizó un estudio piloto para asegurar la adecuación y la inteligibilidad de las preguntas. Se recogieron 5.205 encuestas completas, correspondientes a 2.840 personas diagnosticadas de trastorno psicótico (incluyendo esquizofrenia) y 1.341 cuidadores, de toda España.
ResultadosLa necesidad más importante según la evaluación de los participantes fue el apoyo emocional (amistades, pareja, familia). El 91% de los pacientes indicaron que esta necesidad era «bastante» o «muy importante». Tanto las personas con esquizofrenia como los cuidadores percibían que su salud era pobre (3,29 y 3,3, respectivamente, en una escala ascendente de 0 a 5). El 43% de los hombres y el 39% de las mujeres refirieron tener «poca» o «ninguna» libertad para tomar decisiones vitales importantes. Para el 35% del total de participantes el tratamiento psicoterapéutico se instauró demasiado tarde. El trabajo fue «importante» o «muy importante» para el 74% de los encuestados, especialmente para los jóvenes. La iniciativa contra el estigma más valorada fue aumentar la inversión en planes de atención para la esquizofrenia.
ConclusionesLos gestores de servicios de atención de salud mental deben considerar la importancia que otorgan las personas diagnosticadas de psicosis a las necesidades emocionales, la percepción de libertad para tomar decisiones y la intervención temprana.
Psychotic disorders, including schizophrenia, are a group of severe mental disorders which constitute one of the main causes of disability worldwide (Global Burden of Disease Study).1,2 People with psychotic disorders experience significant functional impairment and pose a huge challenge to public health. During recent decades, thanks to the movement towards recovery and patient-orientated care, greater interest has been paid to the comprehension of how the patient perceives of their world and unsatisfied treatment needs. People are increasingly describing and reflecting their experiences as part of a rising written literature, stemming from what we could in general call the user’s outlook on the service. Several self-help groups, such as The Hearing Voices Network (HVN), are explicitly based on the idea that different people have different ideas regarding the nature and origins of their experiences, and about their unsatisfied needs.3 Individuals with psychosis and their caregivers, have been involved in the identification of their individual needs, actively participating in the treatment process.4–6
This has been supported by the development of tools for the assessment of needs and the refinement of a collaborative models based on shared decisión-making.7,8 Within this context, the importance of need assessment and the identification of the patient outlooks relating to the development of services and interventions has been widely recognised.9
The study of needs relating to schizophrenia was originally assessed through satisfaction with services, reported by users and their families,10,11 and also through the development of standardised tools to assess needs, such as the Caregivers’ Needs Assessment for Schizophrenia12 or the Camberwell Assessment of Need (CAN)13 interview. An alternative focus was based on direct and anonymous surveys. Living with schizophrenia, people’s experience of the condition14 was a survey which focused on the care perceived by the people in this situation and by their caregivers. It revealed the problems relating to information provided during diagnosis, access to treatment, support received and lack of involvement in treatment selection. The Scottish Schizophrenia Survey also offered a perspective on the experience of the people who live with schizophrenia and psychosis and their caregivers.15 The majority of participants (77%) who were diagnosed for a psychotic disorder reported that they had faced stigma and discrimination at some time. Lastly, another cross-sectional survey of 138 caregivers in 16 European countries reflected general awareness on aspects relating to schizophrenia, and on the importance of its role in the improvement of weak adherence to medication.16 however, these surveys had a relatively small sample size and were mainly aimed at treatment preferences, at adherence to the same, and at stigma, without covering other major aspects such as emotional needs or the perception of health.
Several tools have already been validated to assess patient and caregiver needs, but they are very broad for such a large scale study and are normally focused on a specific issues: levels of care required;17 satisfaction with services;18 quality of life or social functioning; clinical status or burden of the caregiver.19–22 We therefore decided to develop a very brief and viable questionnaire which could be completed by a sample of people diagnosed with psychosis and by their caregivers, covering areas of different needs and designed by a multi-disciplinary team that included patient and family associations.
Professionals from the areas of mental health and psychiatry, together with numerous associations and interest groups, decided to carry out this research in Spain, to redefine the current focus on psychosis, with the firm desire to explore genuine needs. In this study, our aim was to directly gather the opinions of people with psychosis, as well as that of their family members and close friends, relating to their treatment needs and preferences.
The objectives of this study were to: a) understand the opinions of people with psychosis and their caregivers regarding the value of different basic and personal needs; b) determine their perception of subjective health; c) determine what professional help was perceived as the most highly valued and d) explore their opinions about delayed medical and psycho-social treatment.
MethodsThis survey was conducted between July 2014 and October 2015 with people diagnosed with any psychotic disorder, including schizophrenia, and their caregivers, with the aim of covering all the Spanish autonomous communities. Participants did not receive any incentive to participate.
A panel of experts, consisting of three renowned psychiatrists in the field of psychosis (with over 20 years of experience in clinical research in the field of psychosis, active members of international scientific societies and opinion leaders of social media), one clinical psychologist with extensive experience in clinical treatment and four representatives from patient and family associations jointly agreed on the redaction of an ad hoc questionnaire aimed at achieving the study objectives. The questionnaire preparation process was as follows: firstly, the experts agree on the major aspects to be explored: the basic and personal needs of people diagnosed with psychosis and those of their caregivers; subjective health status; freedom to take decisions; delay in medical and psycho-social treatment; social comprehension and acceptance of the disease, and their opinion on anti-stigma initiatives. Secondly, questions and response options were developed (including several questions focused on obtaining socio-demographic data). The questions were relevant, specific, simple, and comprehensible for the people and there were no design biases. After this, overlapping questions were rejected, together with those that did not satisfy the previous requisites. The final questionnaire therefore consisted of 4 initial questions (age, sex, geographic location and details regarding whether the person completing the questionnaire was a patient or a caregiver) and 9 other questions.
“Subjective health status” included 6 options of response: very poor, poor, medium-poor, medium-good, good and very good. “Freedom to take decisions” included 4 response alternatives: none, some, quite a lot and a lot. “Basic and personal needs” included 4 options which were: 1, unimportant; 2 a little important; 3 quite important and 4, very important. “Delay in medical/psycho-social treatment/rehabilitation included 2 options: yes/no. “Help offered by professionals” and “initiatives to eradicate stigma” scored as: 1, not important; 2 a little important; 3 quite important; and 4, very important. “Acceptance and support” included 2 options: yes/no. “Initiatives to eradicate stigma” included 6 options ranked as: 1, not important; 2, a little important; 3 quite important, and 4, very important. The panel of experts (both professionals and representatives of patients and caregivers) reached a consensus and approved the theoretical construct to be integrated into the operative medium (final questionnaire), with a pilot study being conducted to guarantee the appropriateness and intelligibility of the questions for the users and their family members (from the AMAFE Associations). The final questionnaire was redacted in Spanish (Spanish and English versions are attached as Supplementary material 1).
The target population was the Spanish population of both sexes, aged 18 years and upwards. A total of 170,000 questionnaires were distributed with the installation of 200 collection boxes, in mental health services throughout the country. The printed questionnaire was completed voluntarily by the patient or caregiver, without the help of any other personnel, for an approximate duration of 5min. An online questionnaire was also loaded on the web page <www.vozsaludmental.com>. Patient and caregiver associations (from the Spanish Mental Health Federation) notified the possible participants of the existence of this survey among its members, extending this to hospitals, mental health centres and public and private organisations, that showed an interest in participating. They were all non-profit-making entities of social interest, focused on the adoption of measures which would contribute to the improvement in the quality of life of people with mental disorders and their families. The collected sample was therefore a sample of convenience. Responses to the survey were kept in secure, computerised files. Participants were guaranteed that their answers would not be in any way linked to their name or identifiable information. The study was approved by the Clinical Research Ethics Committee of Hospital Universitario Príncipe de Asturias (code OE 13/2018).
AnalysisBoth data collection and analysis were conducted globally and with stratification, in keeping with participant characteristics (i.e. patient or caregiver), age, sex and geographical location. Variable analysis was strictly categorical and based on the description of frequency and response rate. The exact Fisher test was used to compare these types of variables between categories. To compare ordinary variables the Mann–Whitney U test was used, in the case of 2 groups of comparison, or the Kruskal–Wallis test for 3 or more groups. The internal consistency of the survey was determined using item/total correlations and McDonald omega coefficients. To compare results with the score reported by the general population of the Spanish National Health Survey we converted the subjective health status score into a five-point Likert scale where 1 was very bad and 5 very good. Absent data were not attributed or substituted. Statistical significance was established at p<.05. Analysis was made using the Statistical Package for Social Sciences version 23,23 and the McDonald omega coefficients were calculated with the JASP open source statistical software.24
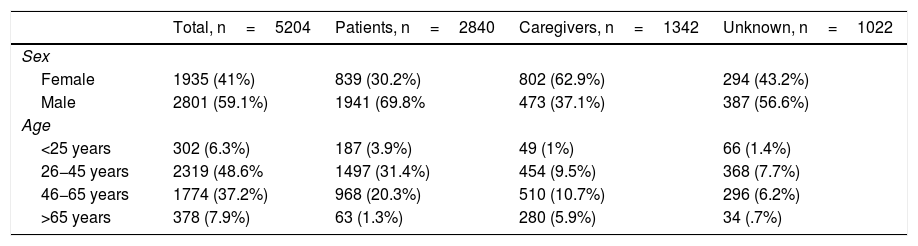
ResultsA total of 5205 respondents completed the questionnaire. Of these, 2840 identified themselves as patients with schizophrenia/psychosis, 1341 were caregivers, and in 1024 cases this information was not available. Age and sex distribution of the sample is contained in Table 1.
Socio-demographic sample characteristics.
| Total, n=5204 | Patients, n=2840 | Caregivers, n=1342 | Unknown, n=1022 | |
|---|---|---|---|---|
| Sex | ||||
| Female | 1935 (41%) | 839 (30.2%) | 802 (62.9%) | 294 (43.2%) |
| Male | 2801 (59.1%) | 1941 (69.8% | 473 (37.1%) | 387 (56.6%) |
| Age | ||||
| <25 years | 302 (6.3%) | 187 (3.9%) | 49 (1%) | 66 (1.4%) |
| 26−45 years | 2319 (48.6% | 1497 (31.4%) | 454 (9.5%) | 368 (7.7%) |
| 46−65 years | 1774 (37.2%) | 968 (20.3%) | 510 (10.7%) | 296 (6.2%) |
| >65 years | 378 (7.9%) | 63 (1.3%) | 280 (5.9%) | 34 (.7%) |
In general, the caregivers were older than the sample of people with psychotic disorders. Only 11% of people with psychosis were over 55 years of age, whilst among the caregivers 43% were over 55. The majority of patients were treated in outpatient departments, although 42% of the data were completed in associations, 12% in psycho-social rehabilitation centres, 11% in general hospitals, 7% in mental health centres and in 28% of the cases this information was not specified. The 17 autonomous communities of Spain were represented. Madrid (21.7%), Andalusia (13.6%) and Catalonia (10.9%) provided the highest number of questionnaires.
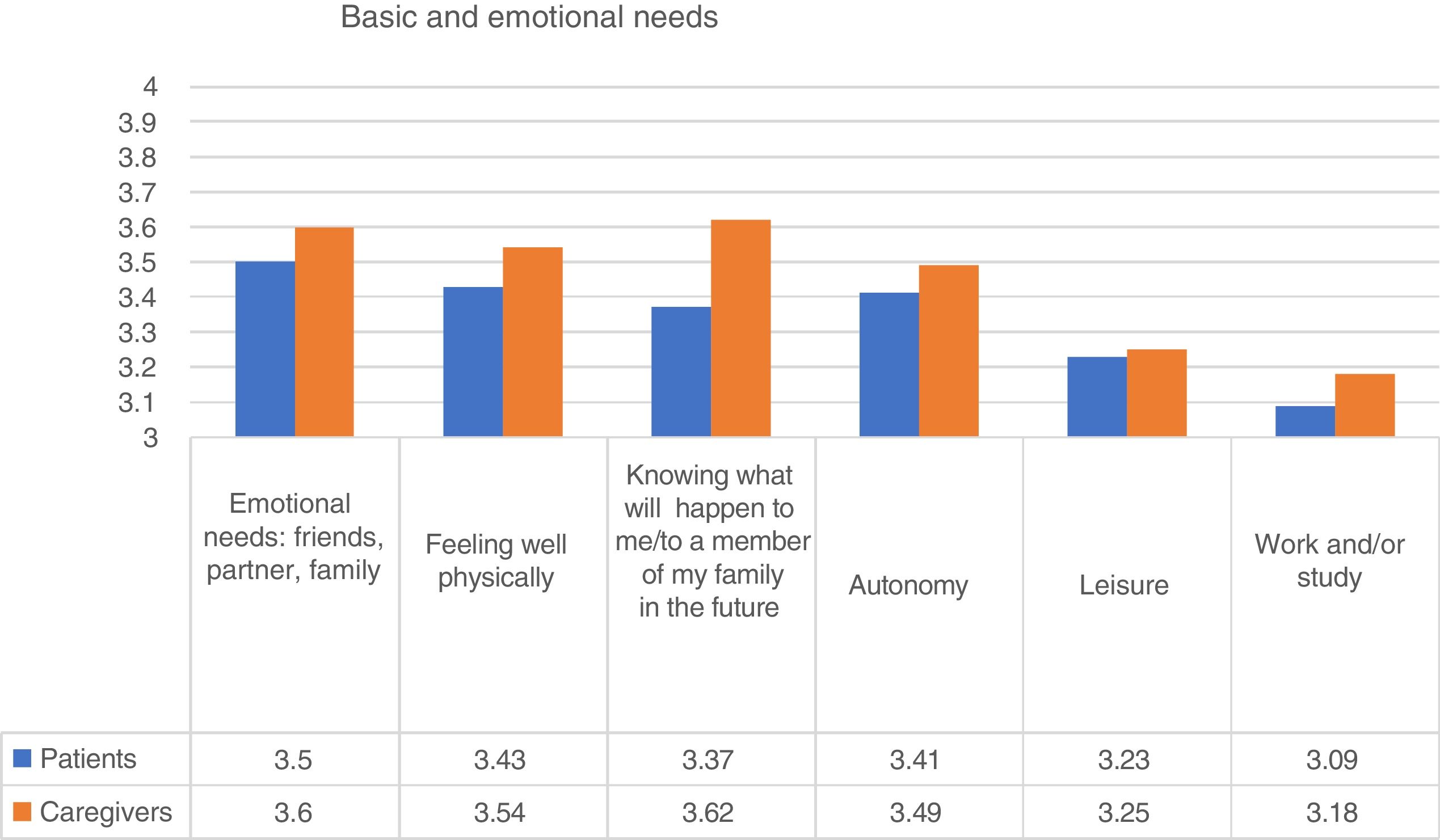
Basic and personal needsWith regard to basic and personal needs, the most highly valued by people diagnosed with psychosis was emotional support (friends, partner, family). Ninety one per cent of people with psychosis indicated that this need was “quite” or “very important”. “Feeling well physically (hygiene, diet, exercise, etc.)” and “increasing autonomy” were the two next needs specified. With regard to the caregivers, their main concern was the uncertainty about what would happen to their family member in the future (Fig. 1). The item “interest in work and/or study” was more important for young participants (Kruskal-Wallis; p<.001).
Subjective state of health
People with psychosis qualifies their subjective health with a mean score of 3.29, very similarly to their caregivers (3.3). A third of the patients and caregivers qualify their own health status as “medium-poor” to “very poor”. In the total sample, being older was associated with poorer subjective health (Kruskal–Wallis, p=.002). However, this did not occur in the individuals with psychosis. Therefore, young people perceived they had a similar health status to middle aged or older people.
Sensation of freedomForty one per cent of the participants reported they felt they had little or no perception of freedom when major decisions about their lives were taken. This percentage was 45% if only patients were included and 35% for caregivers (Mann–Whitney U test; p<.001). It was interesting that the members of associations and users of psycho-social rehabilitation centres reported a lower sensation of loss of freedom than the respondents from hospitals: 46% versus 35%, respectively, reported “no” or “little” sensation of freedom.
Delay in treatmentThirty three point four per cent of people with psychosis and 46.8% of caregivers thought that medical treatment began too late (Fisher test; p<.001). Again, the age of the participants had an effect on this response. Up to approximately 25 years, the age of the participant was associated with a longer delay in treatment. However, once they were older (i.e. over 25 years of age), the percentage of participants who referred to treatment delay progressively increased (Fisher test; p<.001).
Many patients (91%) received psychotherapeutic treatment. However, 37.1% of them (and 42% of the caregivers) thought that psychotherapy began too late. This delay was reported by more women than men (Fisher test; p<.001). Eighty seven point one per cent of patients did not receive any type of psycho-social rehabilitation, including training, workshops and procreative psycho-social rehabilitation.
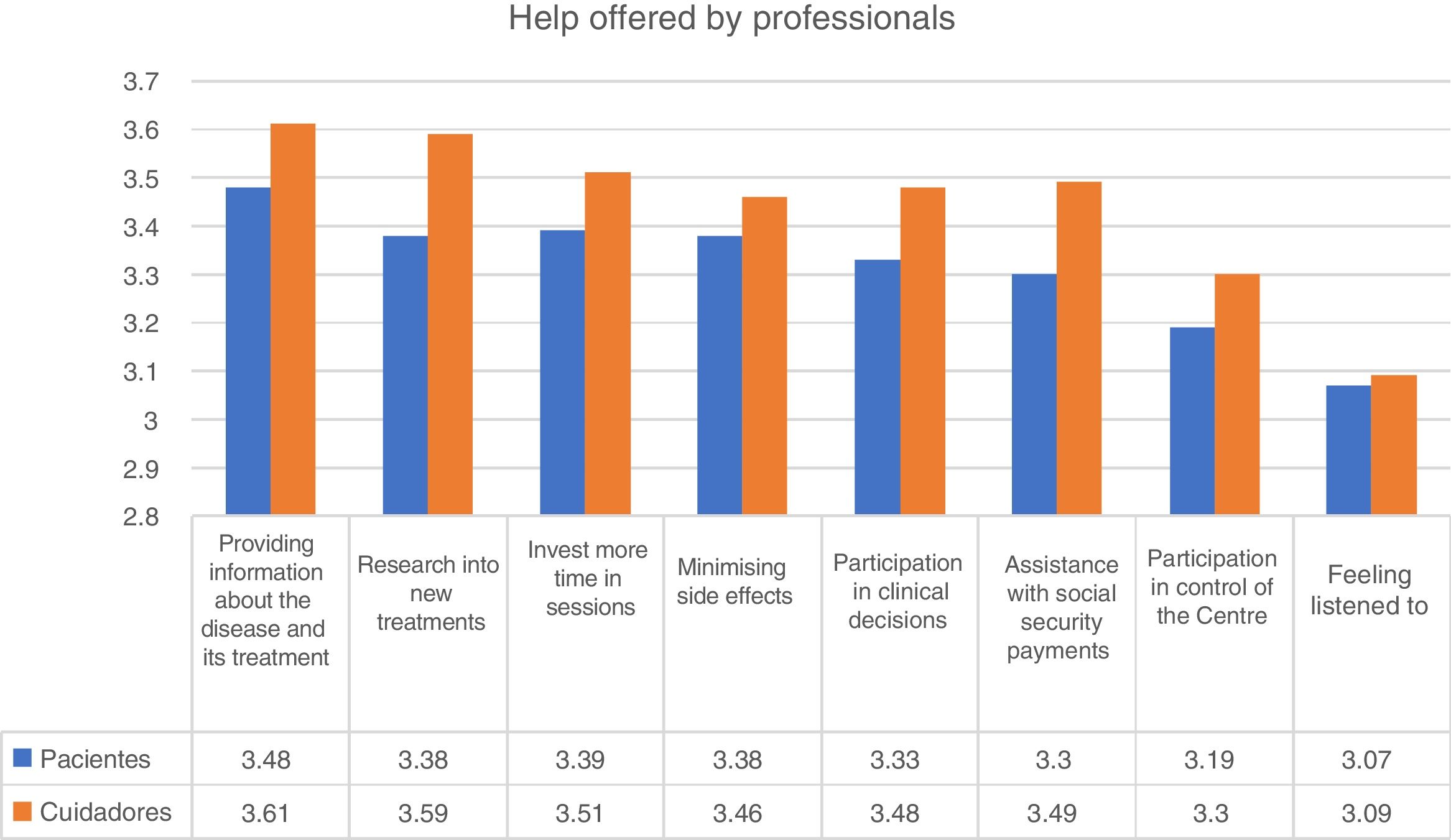
Help from professionalsWith regard to the help offered by professionals, the highest score was given to “provide more information about the disease and treatment”. This obtained a mean score of 3.49 out of 4. In fact, 84% of participants indicated that this help was fairly or very important. The best valued help in second place was to “research into new treatments” and “invest more time in sessions” (Fig. 2).
Comprehension and stigma
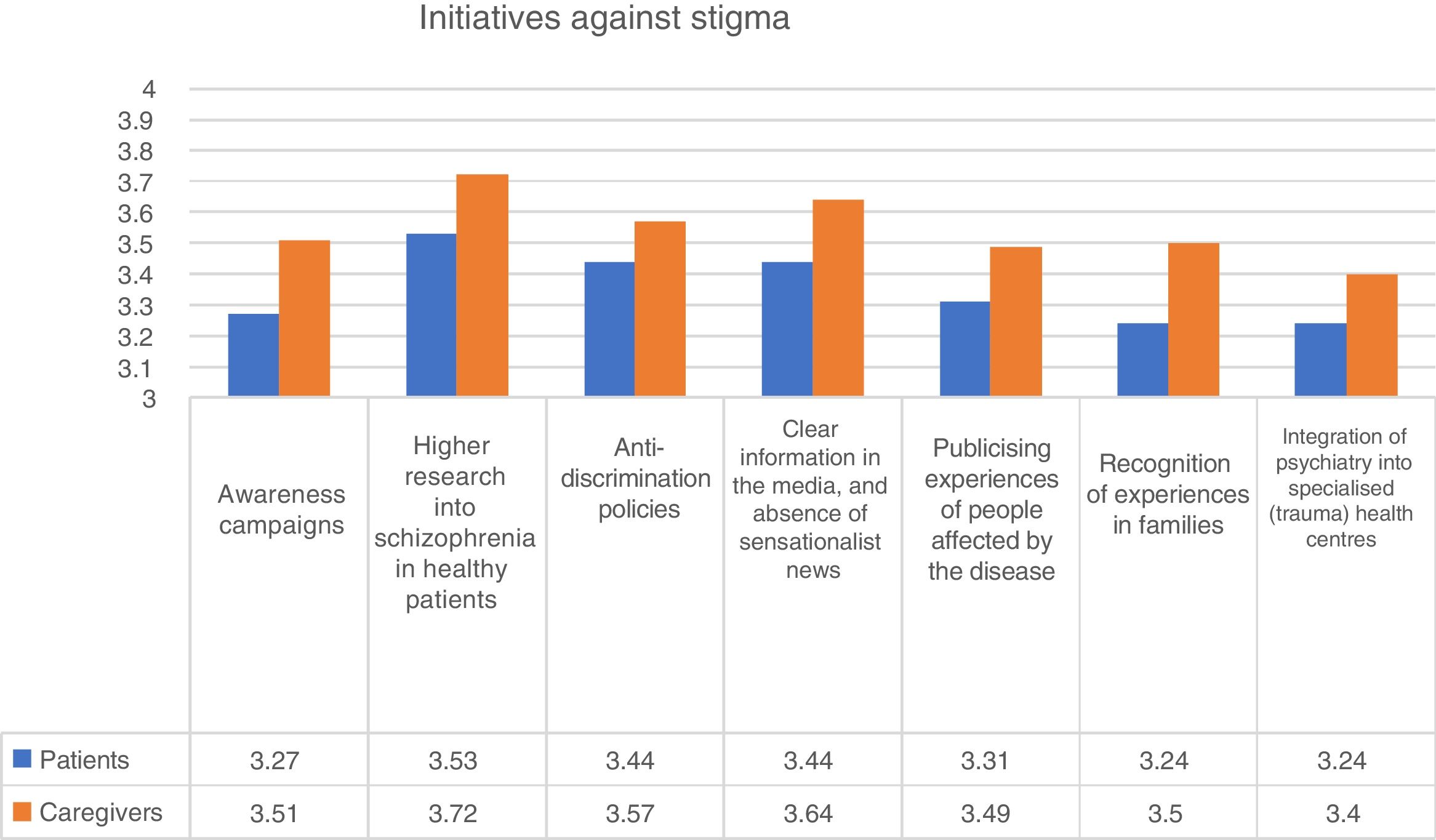
Respondents were asked if they had felt accepted and understood by their environment at the beginning of the disease. Among the people diagnosed with psychosis, 35.8% felt “not” or “not very accepted” at the time of the survey. On a scale of 1 (not accepted) to 4 (highly accepted), the mean score was 2.83 for the patients and 2.97 for the caregivers Mann-Whitney U test; p<.001). This study was no different with respect to age or gender. In contrast, the users of psycho-social associations and centres of rehabilitation reported a higher level of acceptance and comprehension from the beginning of the disease. With regard to the initiatives for reducing stigma, higher scores were given to the increase of investments in health plans for schizophrenia, with a mean score of 3.59 out of 4. In fact, 91% of respondents indicated that this initiative was “quite” or “very important” in reducing stigma (Fig. 3).

We found there to be several differences between the participants who completed the online (n=434; 8.3% of the total sample) or offline questionnaires. The online sub-sample was younger (p=.001), had a similar distribution by gender (p=.418) and higher representation of caregivers (48%; p≤.000). Online participants score significantly higher in the importance of emotional needs (p<.000), worse in subjective health (p<.000) and identified the help “to bear in mind the side effects of medication” as the most relevant.
Internal consistency and reliability of the surveyAnalysis of internal consistency, the McDonald internal consistency coefficient of the survey was calculated as .848 for the 6 Likert type items. The omega coefficient of basic and emotional needs was .638. The coefficient corresponding to the aid offered by professionals was .77, and that corresponding to the initiatives to eradicate the stigma associated with psychosis was .841.
DiscussionThe main findings of this anonymous survey applied to 5205 people diagnosed with psychosis and their caregivers were: 1. The highest scoring need was emotional (emotional relationship with friends, partner and family). 2. The subjective health status of patients and caregivers was similar. 3. Up to 45% of individuals with psychosis reported a zero or low level of freedom to take major decisions regarding their lives. 4. A third of participants declared that medical and therapeutic treatments had been delayed. 5. The anti-stigma initiative most highly valued was to “increase research into schizophrenia in healthcare plans”.
The importance given by people with psychosis and their caregivers in covering emotional needs (friends, partner, family…) is shared by the general population.25 Although professional support may be useful, often the most important source of help and support is the network of relationships the patient has with friends, family and community.26 The project Strategies for Living of the Mental Health Foundation asked people with mental health problems what was the thing that most helped them. Their relationships with professionals and therapists were useful but, as with our findings, relationships with friends, family and other users of the services were more important. What appears to underlie the strategies chosen or discovered was the need for acceptance, emotional support, shared experience and the existence of a meaning to or objective in life.27 Attachment seems to be the most important loving tie, and a resource that helps the patients to feel more secure, confident and emotionally stable. This finding contrasts with the barrier the people with psychosis have developed to survive social relations.
The National Survey of Australia reported that only one in ten men and one in four women with a psychotic disorder were married or in a de facto relationship. Approximately half of the women (56.2%) had children of any age, 25% had children under their care and only 5.5% of the men had dependent children in their care.28 Solitude is associated with the deterioration of social cognition, it is a generalised morbidity risk factor in useful adult life.29 One major factor for understanding this unsatisfied emotional need is the social stigma towards psychosis and the desire for social distancing, which is more pronounced in intimate relationships and is expressed by a high proportion of the general population.30,31 Given the importance of this issue, we asked people who had been diagnosed with psychosis, and their caregivers, about their opinions regarding the most relevant anti-stigma initiatives. The most highly valued was the increase in research on schizophrenia in health plans, which suggests that better and more comprehensive treatment may reduce this painful social gap.
The score of 3.3 out of 5 for subjective health status is lower than the score reported by the general population (3.97), according to the Spanish National Health Survey.32 This underlines the fact that diagnosis of schizophrenia and psychosis affects the individual’s physical health and life expectancy.33 More impacting is the fact that younger people have even greater differences to the general population. Whilst 92.8% of people aged between 15 and 25 in the general population report “good” or “very good” health (Spanish National Health Survey), only 47.6% of all patients referred to this situation. These results reflect the importance of becoming aware of physical health in psychosis/schizophrenia,34,35 and introducing physical training programmes in both hospitals and outpatient care.36,37 Results also underline the physical health of the caregivers, some of whom are older. Gupta et al.38 reflected that the caregivers of schizophrenic patients reported a poorer quality of life related to health than non caregivers, and there were more likely to experience sleep disorders, insomnia, pain and anxiety than the caregivers of other conditions. They could therefore benefit from additional financial, social and health support as well as having better treatment options for their families, which could relieve this care-related burden.39
One notable finding from our study was that up to 45% of people with psychosis reported a zero or low level of freedom in taking major decisions concerning their lives. Although this result did not solely refer to psychiatric treatment one clinical implication of these dramatic data would be the reinforcement of shared decision-making identified by patients from other studies of intrinsic value.40–42 This is also consistent with other results from the survey, such as the need to share more time with the doctor during sessions, and obtaining further information about their disease and treatments. Another implication would be placing emphasis on reducing internalised stigma and the increases in the perception of empowerment,43 which includes the sensations of competence, self-confidence, self-efficacy and the desire and intention to take part in the social sphere and control one’s own life.44–46 The empowerment of people with psychosis may derive from better self-care (and therefore, better physical health) and greater confidence in developing emotional ties. With regard to the lower level of freedom in hospitals than in rehabilitation programmes, the initial possible reason is that hospitals offer care to younger people and to acutely ill patients, most of whom are in the early stages of their disease. Improving the information about these states is also essential, and in Spain several projects exist aimed at optimising this outcome.47
The delay in treatment reported by participants coincides with that found in the literature, where delays of 1–3 years for seeking treatment in the initial episode of psychotic disorders are not infrequent.48 Indeed, barriers exist for seeking early psychiatric treatment among patients with an initial episode of psychosis. These include inappropriate beliefs regarding the cause, fear of being labelled, poor comprehension of the nature of the disease, financial problems or limited access to early intervention on psychosis.49,50 Both the patients and caregivers of our survey complained about this delay, highlighting the importance of an urgent assessment of the people who presented with any type of psychotic symptom, and potential referral to specialised coordinated, evidence-based and multi-disciplinary services.50–52 The survey participants also highlighted the importance of “providing information about the disease and treatment” (many assessed the help provided by professionals). A recent online interview also reported that over half of the caregivers declared that they had not received any information at the time of diagnosis and almost a third ad received verbal information.14 People affected by schizophrenia should receive the right, precise and high quality information about the situation, the different treatment options available and the potential side effects of the medication.
This study had two different limitations that should be taken into account. Firstly, the objective of this study was not to develop a scale or a test but simply to directly describe the opinion of a population—patients and caregivers—on different issues under the general title of “the basic needs of people diagnosed with psychosis and those of their caregivers”, and as a result some of the steps recommended for the development of a test or scale were not followed.53 The interpretation of studies based on surveys must be undertaken with precaution as in our case, which used a self-selected recruitment procedure. This assessment of a large population may cover a high number of potential participants, although the researcher has no control over the selection process and may only work on the study advert design.54 This large-scale data collection method may also give rise to a high rate of absent data (e.g. in 1024 cases the identification of the patient or caregiver was not available and 24% of the participants did not report the treatment centre). Furthermore, administration of the survey was not standardised, which may have potentially increased error variance. Several data could not be verified due to the anonymous nature of the survey design (e.g. the situation as patient or carer), and several clinical data, such as specific diagnosis or medication administered were not recorded. The participant patients were diagnosed with “schizophrenia” or “psychotic disorder”, which included heterogeneous situations. The difference in the survey between delay in medical and psycho-social treatment may be artificial, since appropriate medical focus should be extensive and bio-psycho-social. Lastly, this study was limited to participants who were resident in Spain. A large-scale, international survey would enable us to compare opinions of participants from different cultural and geographical locations.
ConclusionsThis study is a form of focusing on the reality of living with psychosis from a totally personal and committed viewpoint. Through a direct and anonymous survey, 5205 people diagnosed with psychosis and their caregivers expressed their opinions about the needs and preferences in different areas, such as personal and social dimensions of the disease, freedom to take decisions, delay in medical and psychotherapeutic treatment, psycho-social rehabilitation, help offered by professionals, social acceptance and stigma. The study results may be an opportunity to consider and manage these identified needs, thus improving mental health care services. At least four requests arose from participant opinions which were to: 1) increase patient confidence and their subjective sensation of freedom (empowerment); 2) improve early detection and intervention systems, as proposed by many experts in the field; 3) provide the correct medical, psychological and social care to the caregivers of patients with psychosis and 4) invest decisively in health plans and research into new therapeutic strategies for psychosis/schizophrenia.
FinancingThis study was partially subsidised by Otsuka–Lundbeck. The financiers did not play a role in the design, data collection and analysis, the decision to publish or the preparation of the study document.
Conflict of interestsWith no relevance whatsoever to this study, Dr. Lahera has been an adviser or has received fees or subsidies from Janssen-Cilag, Otsuka-Lundbeck, Lilly, Astra-Zeneca, CIBERSAM and the Instituto de Salud Carlos III.
Dr. Gonzalez-Pinto has received subsidies and has acted as a consultant, adviser or speaker of CME for the following entities: Janssen, Lundbeck, Otsuka, Pfizer, Sanofi-Aventis, Servier, Ministry of science and innovation (CIBERSAM), Ministry of Sciences (Instituto Carlos III), Basque Government, University of Basque Country and Stanley Medical Research Institute.
Ms. Ana Cabrera Cifuentes has been an adviser or has received fees from CIBERSAM, Janssen-Cilag, Ferrer, Lundbeck and Otsuka.
Dr. Arango has been an adviser or received fees or subsidies from Acadia, Abbot, AMGEN, Astra-Zeneca, Bristol-Myers Squibb, Caja Navarra, CIBERSAM, Fundación Alicia Koplowitz, Forum, Instituto de Salud Carlos III, Gedeon Richter, Janssen Cilag, Lundbeck, Merck, Ministry of Science and Innovation, Ministry of Health, Ministry of the Economy and Competitiveness, Mutua Madrileña, Otsuka, Pfizer, Roche, Servier, Shire, Schering Plough, Sumitomo Dainippon Pharma, Sunovio and Takeda.
Dr. Vieta has received grants and has acted as a CME consultant, adviser or speaker for the following entities: AB-Biotics, Allergan, Angelini, Astra-Zeneca, Bristol-Myers Squibb, Dainippon Sumitomo Pharma, Farmindustria, Ferrer, Forest Research Institute, Gedeon Richter, Glaxo-Smith-Kline, Janssen, Lundbeck, Otsuka, Pfizer, Roche, Sanofi-Aventis, Servier, Shire, Sunovion, Takeda, the Brain and Behaviour Foundation, Ministry of Science and Innovation (CIBERSAM), Seventh European Framework Programme (ENBREC) and the Stanley Medical Research Institute.
The other authors have no conflict of interests to declare.
We wish to thank all respondents for their participation in the study and in particular the users and family members of the AMAFE Associations for their incalculably useful comments on the document.
Please cite this article as: Lahera G, Cid J, Gonzalez-Pinto A, Cabrera A, Mariner C, Vieta E, et al. Necesidades de las personas con psicosis y sus cuidadores: «en voz propia». Rev Psiquiatr Salud Ment (Barc.). 2019. https://doi.org/10.1016/j.rpsm.2019.11.002