




To analyse changes in suicide mortality trends in Spain between 1980−2016 using joinpoint regression models.
MethodsMortality data were obtained from the INE. For each gender, age-group-specific and standardised (overall and truncated) rates (ASR) were calculated by the direct method (using the European standard population). The joinpoint analysis was used to identify the best-fitting points where a statistically significant change in the trend occurred.
ResultsAge adjusted mortality rates due to suicide in men was 9.8 / 100000 males in 1980 and 11.8 in 2016, with an average annual increase of .8%. In women, the rates increased by 1.0% per year from 2.7 women per 100,000 in 1980 to 3.7 in 2016. The joinpoint analysis identified three turning points in the rates for both men (1986, 2000 and 2010) and women (1986, 2004 and 2010), which identify changes in the trend. In the period 2010−2016 the rates increase in women while in men the rates remain stable.
ConclusionsOur work shows a marked increase in mortality by suicide in Spanish women (2010−2016) while in men the rates remain stable. Little is known about the determinants of the increase and, therefore, more studies are needed.
Analizar los cambios en las tendencias de la mortalidad por suicidio en España durante el período 1980−2016 utilizando modelos de regresión joinpoint.
MétodosLos datos de mortalidad se obtuvieron del INE. Para cada sexo, las tasas específicas por grupo de edad y estandarizadas (general y truncada) (ASR) se calcularon por el método directo (utilizando la población estándar europea). El análisis de punto de unión se utilizó para identificar los puntos más adecuados donde se produjo un cambio estadísticamente significativo en la tendencia.
ResultadosLa tasa de mortalidad por suicidio ajustada por edad en hombres pasó en el periodo de estudio de 9,8/100000 varones en 1980 a 11,8 en el año 2016, con un incremento anual medio del 0,8%. En las mujeres, las tasas se incrementaron un 1.0% anual pasando de 2,7 mujeres por 100000 en 1980 a 3,7 en 2016. El análisis joinpoint identificó tres puntos de inflexión en las tasas, tanto en hombres (1986, 2000 y 2010) como en mujeres (1986, 2004 y 2010), que identifican cambios en la tendencia. En el periodo 2010-2016 las tasas se incrementan en las mujeres mientras que en los hombres las tasas permanecen estables.
ConclusionesNuestro trabajo muestra un marcado aumento en la mortalidad por suicidio en las mujeres españolas (2010-2016) mientras que en los hombres las tasas permanecen estables. Poco sabemos sobre los determinantes del aumento y, por ello, son necesarios más estudios.
Suicide, although largely preventable, is a major public health problem. There were an estimated 788,000 suicide deaths worldwide in 2015 (standardised rate of 10.7 per 100,000 population).1
The standardised death rate was 10.9 in the European Union (2015), ranging from 30.8 in Lithuania and 2.2 in Turkey. The rate in Spain (7.5) was lower than the European rate in general, similar to that of the United Kingdom (7.3) but higher than Cyprus (4.4) and Greece (4.7).2 In recent years, suicide rates have declined in the European Union, from 11.7 in 2011 to 10.9 in 2015.2
Suicide mortality rates in Spain increased throughout the last century, reaching a peak in the 1980s.3 Subsequently, the rates decreased in both men and women and recently increases have been described at national level and in some areas of the country,4,5 which have been associated with the financial crisis.6,7
There is little history of suicide mortality trend analysis in Spain in five-year age groups.8
Joinpoint regression methods have been shown to be useful in identifying and describing changes taking place in different time periods along the trend of suicide mortality data.9–11
Taking all the above into account, we set out to provide updated information on suicide mortality in Spain and to analyse recent changes in the trend of this mortality over the period 1980−2016 by five-year age groups and sex using joinpoint regression models.
Patients and methodsMortality data by age and sex correspond to those published by the National Institute of Statistics (INE) for the years 1980–2016. Deaths by suicide were used (codes E950-E959 and X60-X84, Y87.0 of revisions 9.a and 10.a of the International Classification of Diseases [ICD] for the periods 1979–1998 and 1999–2008, respectively). The populations estimated at 1 July by the INE were used to calculate indicators.
Per sex, the specific rates by age group and the standardised rates (all ages) were calculated by the direct method, using the European population as a reference12, and expressed as rates per 100,000 person-years.
Joinpoint regression models were used for trend analysis.13 The purpose of these models is twofold: to identify the moment when significant changes in the trend occur and to estimate the magnitude of the increase or decrease observed in each interval. Thus, the years (period) comprising each trend are expressed in the results, as well as the annual percent change (APC) for each.
Standardised mortality rates and their standard errors were used for the estimation of these models, and deaths and populations were used for the models by age group under a Poisson distribution model.
We set the minimum number of data in the linear trend at both ends of the period at 3. A maximum of 3 turning points was sought in each regression, for which the programme looks for the simplest model that fits the data using the weighted least-squares technique, then estimating their statistical significance using Monte Carlo permutations.
To quantify the trend over the whole period, we calculated the average annual percent change (AAPC) as a geometric weighted average of the APCs of the joinpoint model. This represents a summary measure of the trend over the study period. If an AAPC is entirely within a single segment, the AAPC will be equal to the APC for that segment.
When describing the results of trend analysis, the terms "increase" or "decrease" indicate statistical significance (p< .05), while non-significant results are reported as "stable".
The software's pairwise comparison option was used to check whether the trends were parallel by sex.14 Statistical significance was set at 0.05.
The Joinpoint Regression software was used to perform all the calculations.15
ResultsIn the period 1980−2016, 113,653 deaths by suicide occurred in Spain (85,459 in men and 28,194 in women).
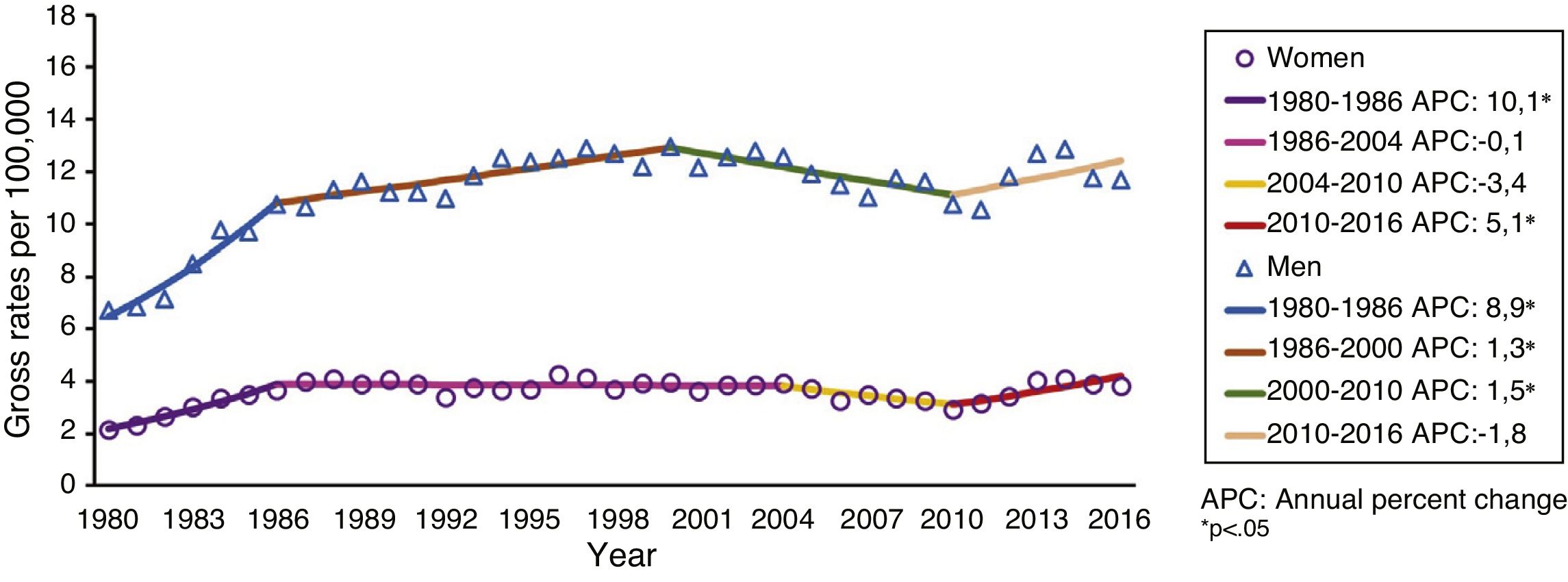
Fig. 1 shows the evolution of gross mortality rates by suicide according to sex and the results of the joinpoint regression analysis, i.e. the points at which the rates change significantly and the APC of each trend in women and men. The rates increased from 6.7 suicides per 100,000 in 1980 to 11.7 in 2016 (AAPC: 1.8%; p<.05) in men. Women show a similar increase to men, from 2.2 in 1980 to 3.8 in 2016. The joinpoint analysis shows 3 turning points in the rates for both men (1986, 2000 and 2010) and women (1986, 2004 and 2010), but the comparability test rejected the hypothesis of parallel trends.

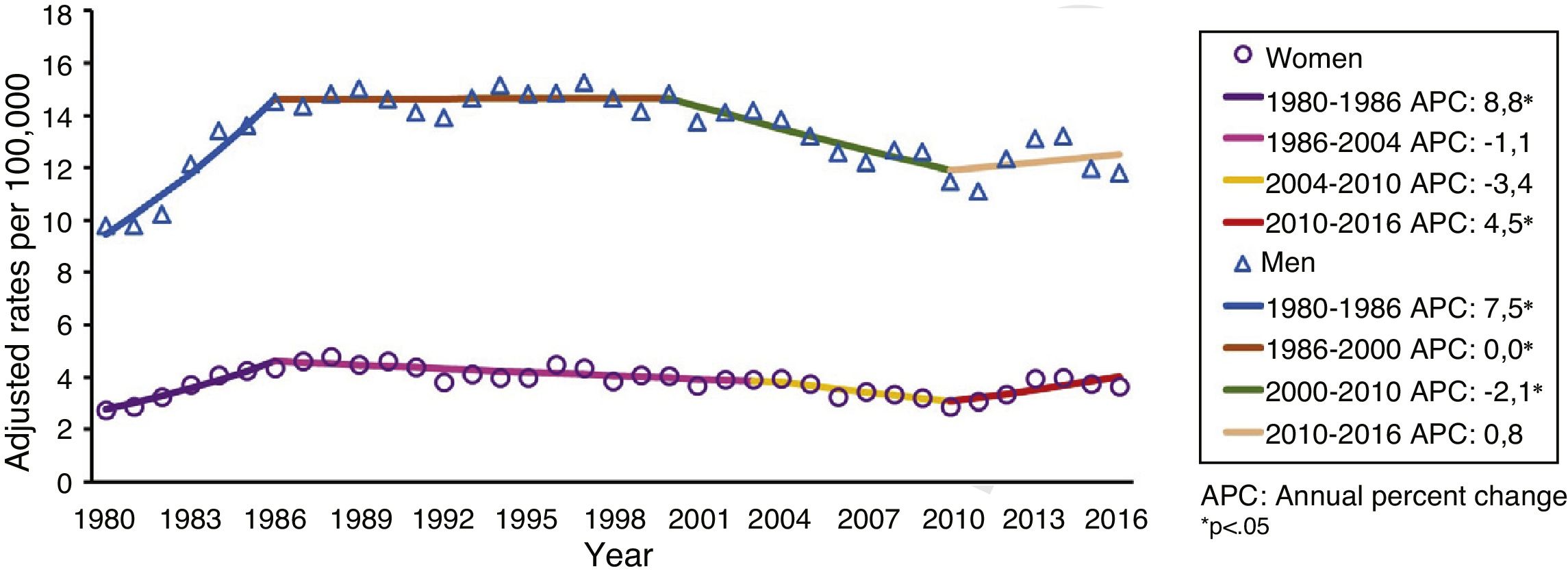
Fig. 2 shows the sex-adjusted suicide mortality rates and the results of the joinpoint regression analysis. The age-adjusted suicide mortality rate in men increased during the study period from 9.8 per 100,000 men in 1980 to 11.8 in 2016, with an average annual increase (AAPC) of .8% (p<.05). In women, the rates increased by 1.0% per year (p<.05) from 2.7 women per 100,000 in 1980 to 3.7 in 2016. The joinpoint analysis identified 3 turning points in the rates, both in men (1986, 2000 and 2010) and in women (1986, 2004 and 2010), which identify changes in the trend. The comparability test showed that the trends were not parallel. In the period 2010−2016 the rates increased in women by 4.5% per year (p<.05), while in men the rates remained stable (APC: .8; not significant).

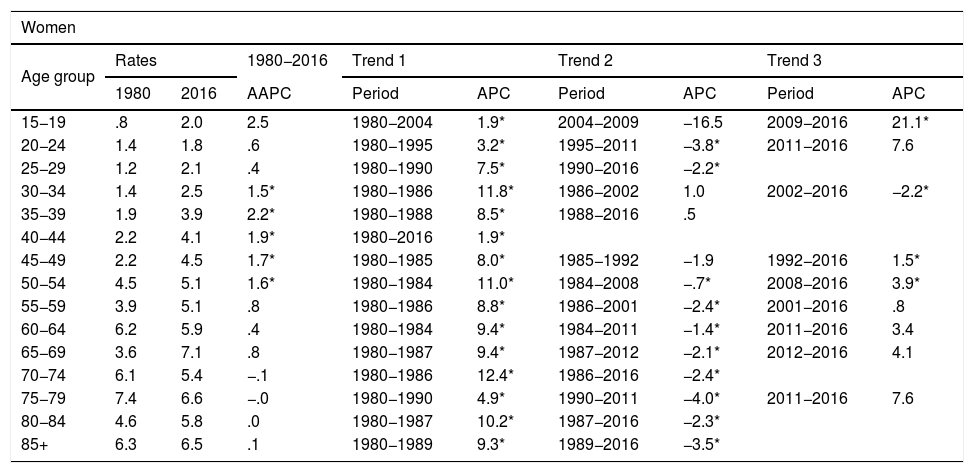
Table 1 shows the results of the joinpoint regression analysis, i.e. the points at which the rates change significantly and the APC of each trend in women and men, respectively.
Specific rates by age group and sex (1980 and 2016). Estimates from the joinpoint analysis. Spain, 1980-2016.
| Women | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Age group | Rates | 1980−2016 | Trend 1 | Trend 2 | Trend 3 | ||||
| 1980 | 2016 | AAPC | Period | APC | Period | APC | Period | APC | |
| 15−19 | .8 | 2.0 | 2.5 | 1980−2004 | 1.9* | 2004−2009 | −16.5 | 2009−2016 | 21.1* |
| 20−24 | 1.4 | 1.8 | .6 | 1980−1995 | 3.2* | 1995−2011 | −3.8* | 2011−2016 | 7.6 |
| 25−29 | 1.2 | 2.1 | .4 | 1980−1990 | 7.5* | 1990−2016 | −2.2* | ||
| 30−34 | 1.4 | 2.5 | 1.5* | 1980−1986 | 11.8* | 1986−2002 | 1.0 | 2002−2016 | −2.2* |
| 35−39 | 1.9 | 3.9 | 2.2* | 1980−1988 | 8.5* | 1988−2016 | .5 | ||
| 40−44 | 2.2 | 4.1 | 1.9* | 1980−2016 | 1.9* | ||||
| 45−49 | 2.2 | 4.5 | 1.7* | 1980−1985 | 8.0* | 1985−1992 | −1.9 | 1992−2016 | 1.5* |
| 50−54 | 4.5 | 5.1 | 1.6* | 1980−1984 | 11.0* | 1984−2008 | −.7* | 2008−2016 | 3.9* |
| 55−59 | 3.9 | 5.1 | .8 | 1980−1986 | 8.8* | 1986−2001 | −2.4* | 2001−2016 | .8 |
| 60−64 | 6.2 | 5.9 | .4 | 1980−1984 | 9.4* | 1984−2011 | −1.4* | 2011−2016 | 3.4 |
| 65−69 | 3.6 | 7.1 | .8 | 1980−1987 | 9.4* | 1987−2012 | −2.1* | 2012−2016 | 4.1 |
| 70−74 | 6.1 | 5.4 | −.1 | 1980−1986 | 12.4* | 1986−2016 | −2.4* | ||
| 75−79 | 7.4 | 6.6 | −.0 | 1980−1990 | 4.9* | 1990−2011 | −4.0* | 2011−2016 | 7.6 |
| 80−84 | 4.6 | 5.8 | .0 | 1980−1987 | 10.2* | 1987−2016 | −2.3* | ||
| 85+ | 6.3 | 6.5 | .1 | 1980−1989 | 9.3* | 1989−2016 | −3.5* | ||
| Men | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Age group | Rates | 1980−2016 | Trend 1 | Trend 2 | Trend 3 | ||||
| 1980 | 2016 | AAPC | Period | APC | Period | APC | Period | APC | |
| 15−19 | 2.5 | 3.3 | 1.0 | 1980−1988 | 10.2* | 1988−2010 | −3.3* | 2010−2016 | 5.2 |
| 20−24 | 6.4 | 5.9 | .6 | 1980−1995 | 3.2* | 1995−2011 | −3.8* | 2011−2016 | 7.6 |
| 25−29 | 6.1 | 5.9 | .4 | 1980−1990 | 7.5* | 1990−2016 | −2.2* | ||
| 30−34 | 6.1 | 9.5 | 1.5* | 1980−1986 | 11.8* | 1986−2002 | 1.0 | 2002−2016 | −2.2* |
| 35−39 | 6.8 | 10.6 | 1.3* | 1980−1998 | 4.1* | 1998−2016 | −1.5* | ||
| 40−44 | 6.2 | 13.7 | 1.9* | 1980−2016 | 1.9* | ||||
| 45−49 | 8.6 | 14.1 | 1.7* | 1980−1985 | 8.0* | 1985−1992 | −1.9 | 1992−2016 | 1.5* |
| 50−54 | 11.0 | 16.5 | 1.6* | 1980−1984 | 11.0* | 1984−2008 | −.7* | 2008−2016 | 3.9* |
| 55−59 | 11.9 | 15.8 | .8 | 1980−1986 | 8.8* | 1986−2001 | −2.4* | 2001−2016 | .8 |
| 60−64 | 13.1 | 15.1 | .4 | 1980−1984 | 9.4* | 1984−2011 | −1.4* | 2011−2016 | 3.4 |
| 65−69 | 16.3 | 15.6 | .8 | 1980−1987 | 9.4* | 1987−2012 | −2.1* | 2012−2016 | 4.1 |
| 70−74 | 22.0 | 16.5 | −.1 | 1980−1987 | 7.2* | 1987−2016 | −1.8* | ||
| 75−79 | 23.0 | 26.1 | .1 | 1980−1986 | 9.5* | 1986−2016 | −1.6* | ||
| 80−84 | 39.4 | 31.1 | .0 | 1980−1987 | 10.2* | 1987−2016 | −2.3* | ||
| 85+ | 30.3 | 38.6 | .4 | 1980−1985 | 9.4* | 1985−1997 | 2.6* | 1997−2016 | −3.2* |
AAPC: average annual percent change; APC: annual percent change.
In both sexes, during the study period (1980−2016) the age-specific rates increased significantly in the 30–54 age groups and remained stable in the rest of the groups. The joinpoint analysis shows no change in trend in the 40−44 age group; both sexes show a continuous increase (APC: 1.9; p<.05) throughout the study period. The rest of the age groups show one or two turning points, with a noteworthy first period of significant increase in the rates (p<.05) in all groups, in both women and men.
The comparability test shows that the rates did not follow parallel trends (p<.05) in the following age groups: 15−19, 35−39, 70−74, 75−79 and 85+.
DiscussionIn Spain (2016), suicide remains the leading cause of unnatural death, producing twice as many deaths as traffic accidents, 13 times more than homicides and 80 times more than gender-based violence.16
Our results, with higher suicide mortality rates in men (Figs. 1 and 2) globally and in all age groups (Table 1), are consistent with those of other studies that show a gender difference in suicide mortality.17 It is also observed that mortality increases as age increases in both sexes (Table 1).
The social construction of gender roles is a common explanation for the higher incidence of suicide in men. Male gender roles tend to emphasise strength, independence and risk-taking behaviour, and it is likely that this prevents men from seeking help for depression and events related to suicidal behavior.18
During the period 1980−1986, Spain experienced a large increase in suicide mortality rates in both men and women. In women, rates then stabilised until 2010, while in men the rates continued to increase until 2000 (Fig. 2).
A decline in suicide mortality rates was observed in several countries in the years prior to the economic crisis of 2008,19 especially among men.20 After 2008, suicide rates increased in Europe and America,21 predominantly affecting men of working age and in countries with higher loss of employment levels.·22
In Spain (2000–2010), suicide rates decreased for men, while for women they remained stable. During the post-crisis period (2008−2016) there was a significant increase in suicide rates, in both sexes, in the 50−54 age group.
Our finding of a recent increase (2010−2016) in adjusted suicide mortality rates in women is similar to that recently observed in Greece.23
In late 2011, the Spanish government introduced austerity measures that involved drastic cuts in the public sector (including health, education and social services).24 Some of these measures, such as reductions in payments under the Dependency Law, may be affecting women more given their predominant role as caregivers.25
Although suicides tend to increase during economic downturns,26 the strength of that association varies between countries, and there is evidence that risks can be mitigated through strong social support and employment programmes.27 Furthermore, it is possible that other factors, other than the crisis, are responsible for the different trends observed by sex in Spain in recent years.
In Spain, there was a dramatic increase in rates in women (aged 15−19) over the period 2009−2016, which must be investigated. In Europe, suicide rates in this age group have decreased in men, while women's rates have been stable or increased.28 The differences in suicide rates between countries and changes within countries are likely due to a complex interaction of culture, socio-economic conditions, availability of means and to public health activities, including adolescent suicide prevention. Factors associated with adolescent suicide would include adverse life events, sexual and psychological abuse, psychiatric problems, impulsiveness and hopelessness.29 The Internet and social networks could have a potential impact on clusters of cases and the dissemination of certain methods of suicide.30
Among the strengths of our study is the long period of time covered (1980−2016), which enabled a systematic analysis of long-term trends in suicide mortality in Spain.
We conducted a descriptive analysis of suicide mortality trends over an extended period (37 years) using joinpoint regression analysis, which is able to identify periods objectively. This avoids the need to pre-specify time periods (which may bias the way trends are analysed).
Although the analysis conducted allows for the identification of objective changes in suicide mortality, this methodology does not enable identification of the causes of these changes.
Despite possible problems of under-recording,31 the reliability of Spain’s suicide statistics is good in comparison with similar countries.32
In conclusion, our study shows a marked increase in suicide mortality in Spanish women (2010−2016), while in men the rates remain stable. Little is known about the determinants of this increase and therefore more studies are needed. Better understanding is essential to plan the most efficient suicide intervention strategies in our country since, as a recent editorial points out, "we must assume that the current state of research does not enable us to predict suicide and the different interventions result in little prevention”.33
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: Cayuela A, Cayuela L, Sánchez Gayango A, Rodríguez-Domínguez S, Pilo Uceda FJ, Velasco Quiles AA. Tendencias de la mortalidad por suicidio en España, 1980-2016. Rev Psiquiatr Salud Ment (Barc.). 2020. https://doi.org/10.1016/j.rpsm.2018.07.002