





Primary vascular tumors of the breast are rare, with angiomatosis and malignant angiosarcoma being the most common. It affects patients from infancy to the sixth decade but typically occurs in young women. Since these lesions are rare and frequently asymptomatic, diagnosis becomes a challenge, in addition to the fact that the histological appearance of benign vascular lesions may resemble those of malignant lesions. The main challenge for the pathologist is the differential diagnosis between angiomatosis and low-grade angiosarcoma due to the similar morphological characteristics that they present in common. Recurrences are frequently encountered in mammary angiomatosis, thus, to prevent this, treatment must include excision with clear margins or mastectomy for lesions that cannot be completely resected. Re-excision is indicated for incompletely excised tumors due to the risk of local recurrence.
Los tumores vasculares primarios de la mama son raros, siendo angiomatosis y angiosarcoma maligno los más comunes. Afectan a los pacientes desde la infancia a la sexta década de vida, pero normalmente ocurren en mujeres jóvenes. Dado que dichas lesiones son raras y a menudo asintomáticas, su diagnóstico es difícil, además del hecho de que el aspecto histológico de las lesiones vasculares benignas puede asemejarse al de las malignas. La dificultad principal para el patólogo es el diagnóstico diferencial entre angiomatosis y angiosarcoma de bajo grado, debido a la similitud de las características morfológicas que presentan en común. A menudo se encuentran recidivas en la angiomatosis mamaria y, por ello, para prevenirla, su tratamiento debe incluir extirpación con márgenes claros o mastectomía para las lesiones que no pueden ser extirpadas completamente. La reextirpación está indicada para tumores no completamente extirpados, debido al riesgo de recidiva local.
The authors present a case of breast angiomatosis, a benign proliferative lesion, rarely described in the literature; whose behavior could be locally aggressive and have a high recurrence rate.1–3 For this reason, in some cases, a complete surgical excision and even mastectomy may be necessary. The purpose of this article is to present, through a review of current evidence and a case report, an update on the dilemma of the differential diagnosis between angiomatosis and low-grade angiosarcoma (LGAS), as well as the treatment of this pathology.
Case reportA 22-year-old woman with no personal or family history of breast disease was referred after presenting an ulcerated lesion in the right breast. The physical examination revealed 2 lesions: a larger firm ulcerated mass (50×40 mm) in the inframammary fold at the junction of the lower quadrants, and another reddish-purple lesion (10×5 mm) with raised growth on the skin (Fig. 1). A breast ultrasound was requested, reporting the absence of solid or cystic nodules in the lesion, with a predominance of fibroglandular tissue, BIRADS 1. There was no evidence of axillary adenopathies, and the contralateral breast did not present abnormalities. The patient was scheduled for surgery (breast sectorectomy) to resect the ulcerated lesion and send it for histopathological analysis.
")
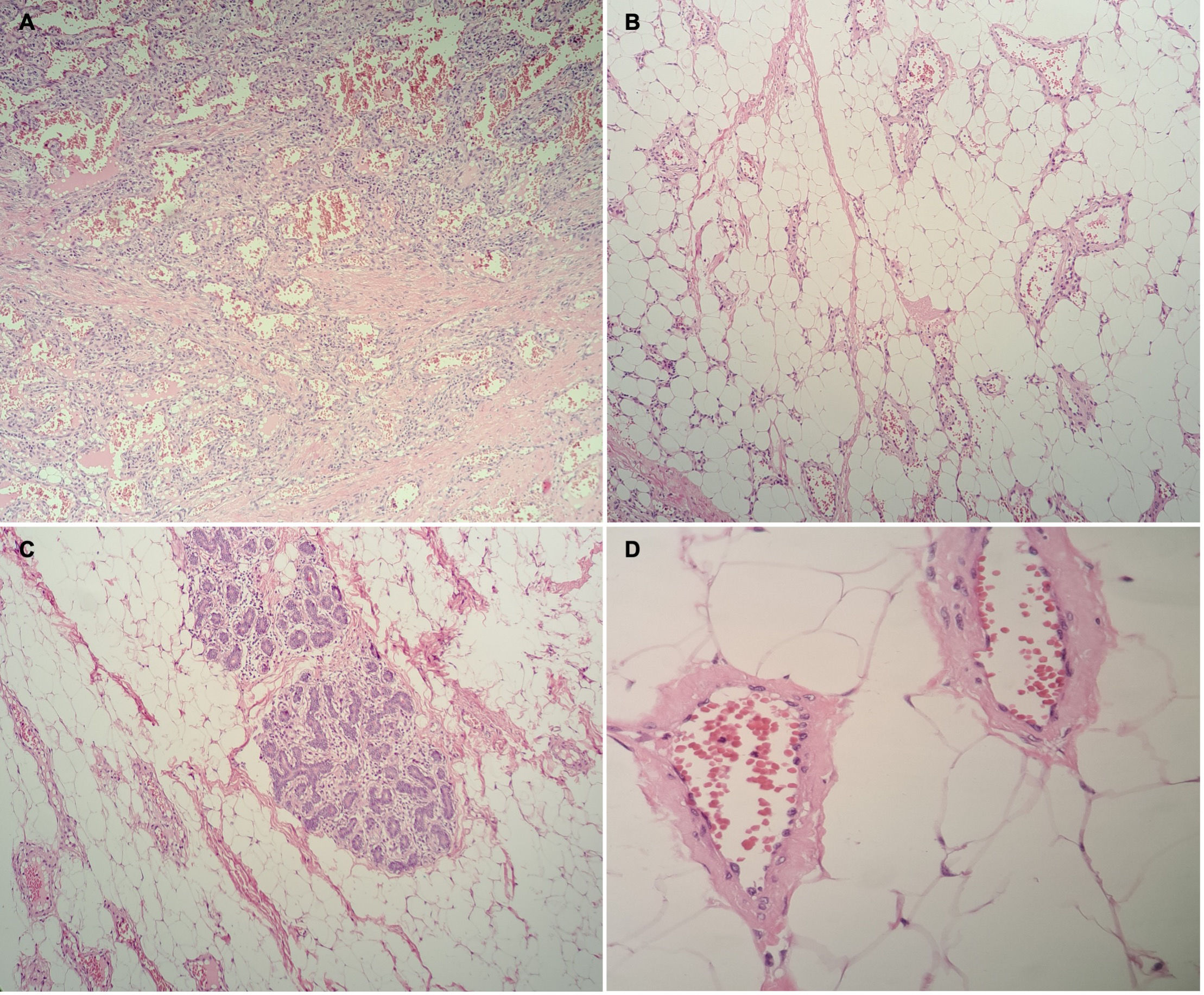
Macroscopic examination of the resected tumor showed an ill-defined lesion with a yellowish appearance and a hemorrhagic surface. Microscopic examination revealed a well-differentiated ulcerated vascular lesion that extended to the reticular dermis, hypodermis, and focally to the perilobular stroma without necrosis and an anastomosing pattern of growth compromising margins (Fig. 2), with low mitotic activity and a very low Ki67 proliferation index (<1%), suggesting the diagnosis of angiomatosis. Margin re-excision and exeresis of the second lesion was performed. Histopathological evaluation confirmed the diagnosis and a lobular capillary hemangioma in the smaller lesion. To date, the patient continues in controls without evidence of lesion recurrence.
 Image shows dermal vascular proliferation with reactive changes underlying skin ulceration. H&E, 100×. (B) Well-differentiated vascular lesion infiltrating hypodermis. H&E, 100×. (C) The lesion infiltrates the interlobular stromal of the breast without invading the intralobular stroma H&E, 100×. (D) High magnification of the vascular lesion shows minimal to no endothelial atypia. H&E, 400×.")
(A) Image shows dermal vascular proliferation with reactive changes underlying skin ulceration. H&E, 100×. (B) Well-differentiated vascular lesion infiltrating hypodermis. H&E, 100×. (C) The lesion infiltrates the interlobular stromal of the breast without invading the intralobular stroma H&E, 100×. (D) High magnification of the vascular lesion shows minimal to no endothelial atypia. H&E, 400×.
Primary vascular tumors of the breast are rare, with malignant angiosarcoma being the most common.1 The current classification of vascular lesions of the breast according to the World Health Organization contains atypical vascular lesions, hemangiomas, angiomatosis, angiosarcomas, and post-radiation angiosarcomas.2
Since these lesions are rare and frequently asymptomatic, diagnosis becomes a challenge, in addition to the fact that the histological appearance of benign vascular lesions may resemble those of malignant lesions.2,3 Therefore, it is important to make an adequate diagnosis including clinical, radiological, and histological information, even with immunohistochemical tests to make a correct differential diagnosis. As a part of the review, we conducted a search through PubMed finding only 197 reports of angiomatosis of the breast from 1975 to date.
Angiomatosis of the breast is defined as a benign proliferation of irregularly shaped small- to medium-sized vessels that diffusely infiltrate the skin, muscle, or bone, and can be locally aggressive with a high recurrence rate.2,4 Clinically, they can present as palpable masses of variable size and progressive growth, with a reddish to purple appearance and sometimes ulcerated. To achieve a better characterization of the lesions, imaging techniques such as Doppler ultrasound and magnetic resonance have been used; however, the diagnosis is made histologically.4 Therefore, complete excision is required for diagnosis and treatment. Histologically, angiomatosis and angiosarcoma may appear similar.
The main challenge for the pathologist is the differential diagnosis between angiomatosis and LGAS due to the similar morphological characteristics that they present in common.5 This distinction is of great importance given the prognostic and treatment implications. Both angiomatosis and LGAS demonstrate anastomosing vascular channels which are typically devoid of erythrocytes and demonstrate diffuse, perilobular growth.4
One of the histological characteristics of angiomatosis is that it grows diffusely surrounding the parenchyma and mammary fat, without invading and destroying the mammary ducts and lobules, with vascular anastomoses and endothelial cells without atypia or mitosis.2,4,5 A distinctive difference with LGAS is that in the latter, the anastomosed vascular spaces invade and rupture the mammary lobules. The endothelial nuclei of angiomatosis appear bland in contrast to the variable degree of cytologic atypia present in the endothelial nuclei of LGAS.6
Overall, in the reported patient, there were similarities and differences in comparison to what was published by other authors. The patient was young and presented a small unilateral mass, in agreement with other publications (mean age: 22 with median size: 9.3 cm, range: 1–17 cm).7,8 There was a difference in tumor's characteristics: the mass was located in lower quadrants (more often arose in the upper outer quadrant or axilla).4,9,10 Histologically, we noted vascular anastomoses; however, the frequency of anastomoses varied. Like the previously reported cases, we observed flat, normochromatic endothelial cells lining the vascular channels.7–9
Recurrences are frequently encountered in mammary angiomatosis and may be related to incomplete excision as well as recruitment of collateral arterial flow into a low resistance vascular bed.4 To prevent this, treatment must include excision with clear margins or mastectomy for lesions that cannot be completely resected. Re-excision is indicated for incompletely excised tumors due to the risk of local recurrence. Angiomatosis of the breast, although prone to local recurrence, is not known to metastasize, contrary to angiosarcoma, which have a poor prognostic and risk for distance metastases.1,4
ConclusionsThe differential diagnosis between angiosarcoma and angiomatosis is essential to define adequate management and treatment; angiosarcoma has a poor prognosis and risk of distant metastasis and requires complete excision or mastectomy with or without adjuvant therapy. On the other hand, the risk of angiomatosis is local recurrence but no metastases have been reported; complete surgical excision or mastectomy is necessary in all cases.
FundingThis research received no external funding.
Ethical disclosuresAll procedures performed in this study involving human participants were conducted ethically according to the ethical standards of the Institutional and with the 1964 Helsinki Declaration and its later amendments and was approved by the Institutional Review Board (Comitê de Ética em Pesquisa em Seres Humanos da Santa Casa de Misericórdia de Porto Alegre).
Patients consentWritten informed consent was obtained from the patient for publication of this case report and any accompanying images.

