



The approval in 2009, of the Protocolo Nacional de actuación Médico-Forense y de Policía Científica en sucesos con víctimas múltiples, was the basic normative to formally regulate both the technical procedures that must be applied, and the different tasks to be carried out in a disaster victim incident in Spain. This article reviews the procedures and techniques used in forensic odontology for human identification in DVI incidents with multiple victims. Given that the recognition of the individualising characteristics of the teeth, and in general the odontological data, supposes a highly specialised process, it is essential the assistance of forensic dentists with experience in this field, who will have the training and the knowledge to carry out the dental procedures such as documenting dental records, accurate interpretation of the results, and withdraw precise dental identification conclusions. Finally, recommendations for the preparation of forensic dental identification reports are included in this review.
La aprobación en 2009, del Protocolo Nacional de actuación Médico-Forense y de Policía Científica en sucesos con víctimas múltiples, supuso la base normativa para regular formalmente los procedimientos y técnicas que deben aplicarse, como las distintas tareas forenses que se tienen que realizar en los supuestos de sucesos con víctimas múltiples en España. En este artículo se revisan los procedimientos y métodos que se emplean en odontología forense para la identificación humana en casos de grandes catástrofes con múltiples víctimas. Dado que el reconocimiento de las características individualizadoras de las piezas dentarias, y en general los datos buco-dentales, supone un proceso altamente especializado, resulta imprescindible el apoyo técnico de odontólogos/as forenses con experiencia en este campo, quienes dispondrán de la formación y los conocimientos necesarios para la realización de la toma de registros dentales, interpretación precisa de los resultados, y obtención adecuada de conclusiones. Finalmente se incluyen recomendaciones para la elaboración de los informes forenses de identificación odontológica.
In order to correctly resolve the medical and legal problems arising in events with multiple victims, it is essential to plan and organise the joint interventions of various professionals and specialists in advance so that a plan of action can be put into operation immediately. Furthermore, advances in forensic medicine in relation to identification techniques and the peculiarities of the organisation of judicial scientific activity in Spain require the participation and coordination of various bodies dependent on different administrative bodies, such as the National Corps of Forensic Doctors and the Institutes of Legal Medicine, the National Institute of Toxicology and Forensic Sciences, the General Commissariat of Scientific Police and the Criminalistics Service of the Civil Guard, and the regional police forces where they are constituted. This need for participation and coordination required the creation of a national protocol to formally regulate both the techniques to be applied and the different tasks to be carried out in cases of events with multiple victims, all of which is regulated by Royal Decree 32/2009 of 16 January, which approves the National Protocol for Forensic Medical Forensic and Scientific Police action in events with multiple victims.1
Currently, there are different scientific methods of identification that must complement each other in order to achieve positive or established human identification. The International Criminal Police Organisation (INTERPOL) has developed and proposed several guides and protocols for the application of scientific methods for the identification of victims of major disasters.2 Among all methods,odontostomatological methods,3–12 are of utmost relevance in situations of multiple casualty events, depending on the nature of the disaster; the nationality and country of residence of the victims; the different types of dental treatment; the availability of adequate antemortem dental records, and the degree of tooth decay.
The relevance of dental methods in human identification in multiple casualty events mainly stems from 2 causes: firstly, because teeth are very resistant to putrefaction and relatively extreme environmental conditions (traumatic, physical and chemical agents); and secondly, because given the enormous variety of individualising characteristics provided by teeth, it could be stated that no two people have the same set of teeth and, at least theoretically, there are an infinite number of points of comparison through the study of the teeth.
The individualising dental characteristics of major forensic interest3 are as follows: teeth present in the mouth (erupted, partially erupted, included, supernumerary), missing teeth (congenital absences, antemortem losses, and postmortem losses), type of dentition (deciduous, mixed, and permanent), position of teeth (malpositions and interdental separations), morphology and diseases of the crown (caries, attrition, abrasion and erosion, alterations-fusions, gemmations, enamel pearls), changes due to defects in the formation of enamel or dentine, habits (smoking, eating habits) and occupational stigmata (microfractures and abrasions of the enamel), staining and colourations, root morphology and diseases (fracture, hypercementosis and resorption), periapical disease (abscess, granuloma and cementomas), morphology and diseases of the pulp chamber and root canals (size, shape, number, formation of secondary dentine and calcification), secondary dentine formation and calcification), dental restorations (type of treatment, teeth and surfaces involved, material used), root canal treatment and prosthetic treatments (fixed, partial removable, complete and dental implants).
Due to the particularities involved in the process of comparative identification of dental data, a summary of the methodology to be followed for dental identification in multiple-casualty events is presented below.
Antemortem dental data recordingOdontogramsAntemortem dental data can be obtained from various sources such as dentists, doctors and relatives of the victim. The most usual way of obtaining this type of information is through the contacts that law enforcement agencies (national or regional police and Civil Guard) make with the victim's relatives. In the interrogation, one should insist on how many dentists or doctors have treated the victim, trying to gather as much information as possible. Regarding the kind of clinical material that should be requested, try to obtain all available material, since, at least a priori, it is not possible to know with certainty which will be the most useful. Whenever possible, try to obtain copies of the original documents, rather than transcriptions, in order to try to reduce the number of errors
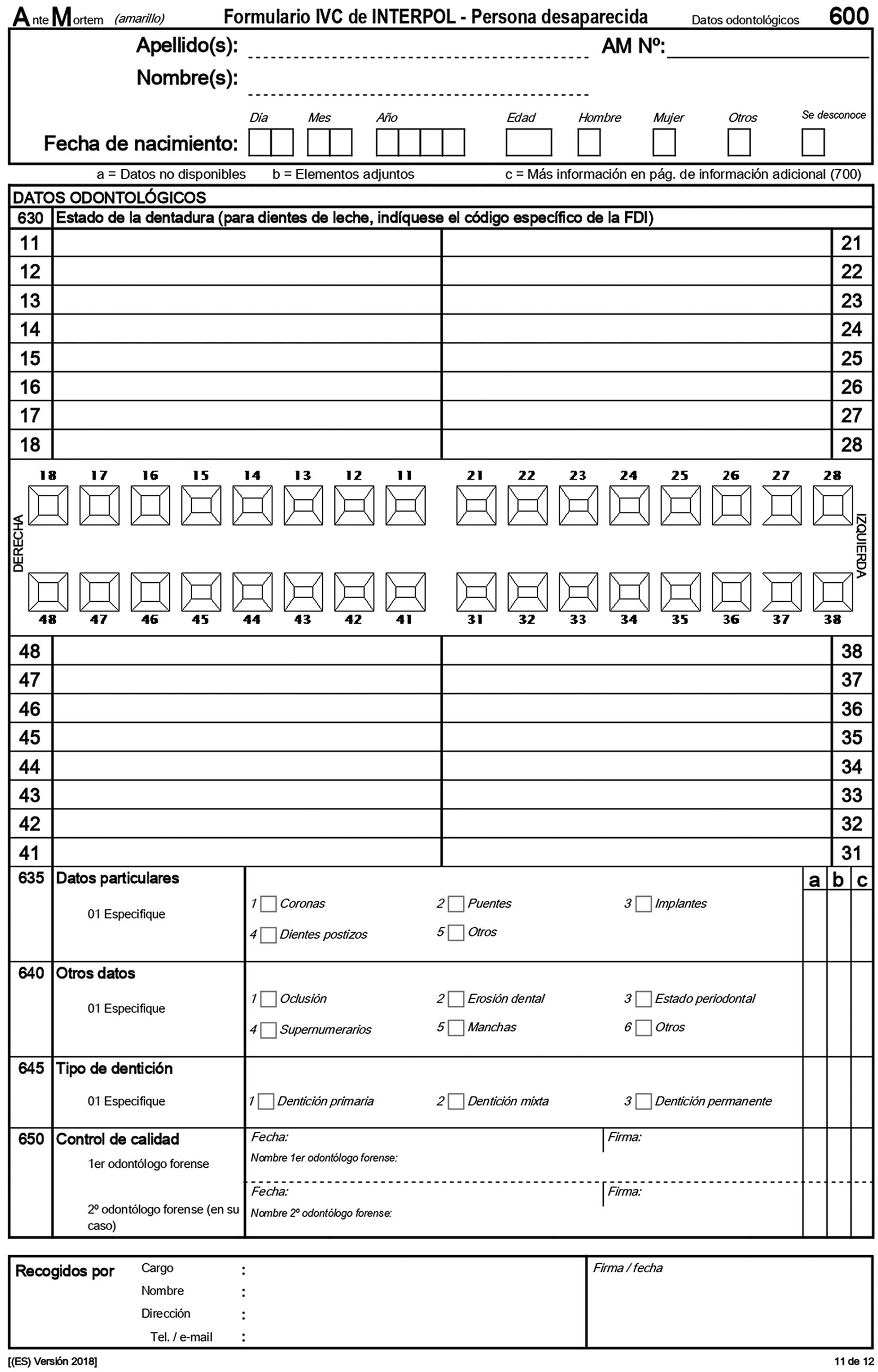
From the information in the patient's dental history, transcribe the entries into an odontogram or dental chart, using the dental nomenclature suggested by the FDI double-digit dental nomenclature and the dental forms proposed by INTERPOL (Fig. 1). Available odontograms will be examined, noting the date and quality of the records, recording whether they are originals, copies or transcriptions, and noting by whom they were made. The most recent records should be reviewed first, and older records should be used for corrections and additional information. However, great care should be taken with the dental data provided because dental records are often poorly documented, incomplete or difficult to understand.
Dental radiographs form for the collection of dental data. (For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article.)")
Radiographs are an invaluable source of information, as they are objective records that provide real data on the findings present,13 and sometimes even allow information to be obtained on dental treatments that are not visible or go unnoticed in the oral examination, such as endodontics. The findings found for each of the teeth are recorded, starting with the oldest radiographs, recording the dates on which the radiographs were taken. It is advisable to keep the radiographs in case it is possible to make later direct comparisons with the postmortem radiographs, and it should be taken into account that nowadays all types of panoramic or intraoral radiographs are available, in radiographic paper format or, more and more frequently, in electronic format.9
Other useful dental material for identificationDental photographs usually only provide information on the anterior teeth and this can be of some interest by providing individual details that may not have been collected in the dental history. Photographs can also be useful in making superimpositions of teeth and facial structures with the available cadaveric remains.
Study models can be considered as excellent antemortem material and should be analysed whenever available. They can provide data on the dental anatomy, the position of the teeth, the size of the individual structures and even the dental treatments carried out.
Postmortem examination and collection of dental dataThe postmortem examination begins with the extraoral examination focusing on 2 aspects of interest: the first is the analysis of injuries of a violent nature present in the stomatognathic area and, secondly, the recognition, description and analysis of injuries of oral origin appearing in another body location, as would be the case of the recognition of bite injuries.
The next step consists of the intraoral examination including, firstly, the examination of the oral soft tissues in which any type of information useful for the identification of the subject is collected (tattoos, pigmentation, diseases, etc.), and the reconstruction of the events that occurred (soft tissue wounds, burns, etc.). The intraoral examination is completed by an exhaustive examination of the teeth and the transcription on an odontogram, which should be the one proposed by INTERPOL (pink postmortem forms). All data providing information on the individualising characteristics of the teeth, such as the presence and absence of teeth, diseases and dental treatments present, shall be recorded.
The estimation of age through dental studies can be very useful for classifying corpses into a specific age group. During the first 2 decades of life, the dentition of the subjects is in a period of formation, development and eruption. It is therefore possible, in these subjects, to study the stage of tooth eruption and the degree of mineralisation of the tooth in order to estimate the dental age. For the assessment of tooth eruption, reference tables are used, such as those of Nolla (1960), Schour and Massler (1941 and 1982), or Demirjian.14 The study of the degree of mineralisation of the tooth allows the estimation of dental age; existing methods are based on the comparison of the degree of mineral development of the different teeth, observed by radiological study and standardised schemes obtained from populations of known age and sex.14–16
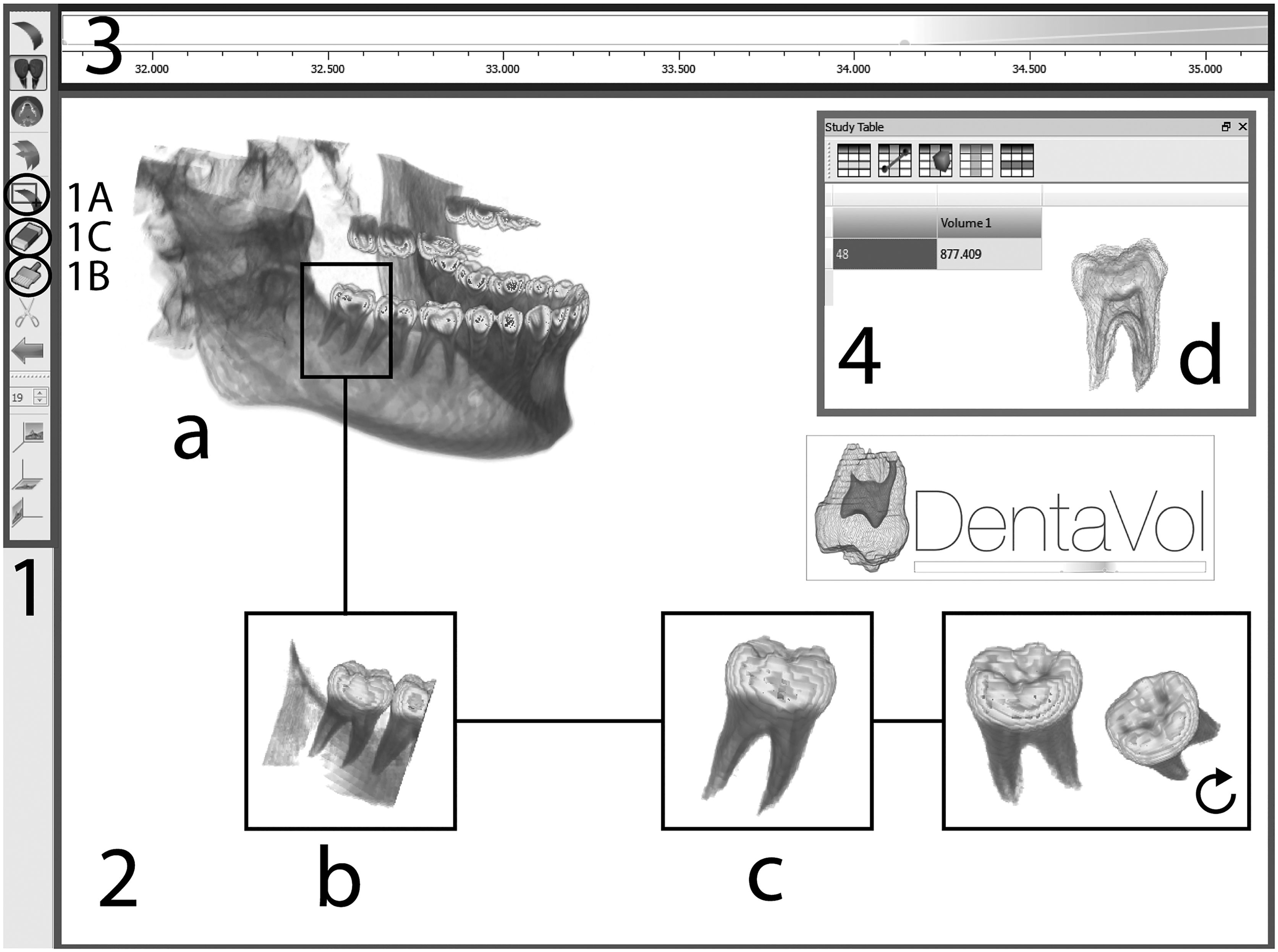
In the age of majority, dental age is estimated by the development of the third molar and its comparison with standardised schemes.17 Most studies of third molar development have been carried out on orthopantomographies in different populations, including those of Spain.18,19 A computer application, DentaVol©,20 has recently been developed, which allows 3D visualisation of third molars and automated calculation of their volume from dental CT images, thus allowing the degree of mineralisation to be objectified and improving the estimation of the age of majority (Fig. 2).
; and image processing sequence (a: 3D image display; b: study area selection; c: third molar isolation; and d: volume measurements). Taken from Márquez et al.20")
DentaVol© interfaces. 1: toolbar; 2: display area; 3: greyscale filter; and 4: case study area); and image processing sequence (a: 3D image display; b: study area selection; c: third molar isolation; and d: volume measurements). Taken from Márquez et al.20
After the complete development of the dentition, from the second decade of life onwards, dental age is estimated by the changes that the dental structure undergoes over the years. These changes are morphological (macroscopic and microscopic) and biochemical. The most studied morphological changes are: attrition or tooth wear, tooth colour change, periodontal attachment level, secondary dentine formation, root transparency, root resorption and cementum apposition. Several authors have studied these changes in extracted teeth and have related them in mathematical formulae that, with greater or lesser precision, are used to estimate dental age.21–23 Methods have also been proposed for estimating age in adults by assessing dental morphological changes using radiographic studies.24,25
Although all dental tissues undergo changes in biochemical composition over the years, of particular relevance are those in dentine. The most relevant changes described include an increase in aspartic acid racemisation,26 an increase in collagen double bonds27 and a decrease in the presence of collagen-degrading enzymes.28 Molecular changes have also been detected, such as alterations in DNA levels, including mitochondrial deletions, telomeric shortening and increased DNA methylation markers.29
Finally, other complementary identification tests can be carried out, such as intraoral radiographs, panoramic radiographs or computerised tomography;9,30 taking impressions; occlusal records, photographs or collection of samples for subsequent study in the laboratory (DNA, toxicological, microbiological, biochemical analysis for age determination, etc.). Of particular relevance for human identification is the study of the victim's genetic profile, as the tooth provides an excellent source of genetic material that is well insulated from putrefaction, degradation and external contamination.31
Comparison of antemortem and postmortem dataThe purpose of the process is to classify antemortem and postmortem records and.
To compare them in order to be able to identify the victims. In dental comparison, as in all comparative identification processes, we must proceed objectively, with scientifically based arguments that allow us to obtain solid conclusions.
Once we have ensured that both the sex and age of the antemortem and postmortem records are compatible, we begin with the comparison of the dentition as a whole and then continue with the detailed comparison, tooth by tooth, to establish identification, analysing the individual characteristics of each tooth. Firstly, we would have to determine which teeth are present and which are absent, and of the latter, differentiate whether the loss was antemortem or postmortem. In addition, the presence of diseases and dental treatments (restorative, prosthetic and implantological), which are a key factor in establishing identities, should also be assessed. Although of lesser identification interest, an occlusal and periodontal study should not be forgotten in search of possible individualising characteristics.
The comparison process can be carried out manually or with the use of some computerised systems that have been designed specifically for this purpose, among which we can highlight the CAPMI3, developed by the American Armed Forces, the WinID® proposed by the American Board of Forensic Odontology (ABFO), or the more recent and widely used DVI System International®, initially known as Plass Data, which was developed at the suggestion of INTERPOL after the 2004 Indian Ocean tsunami. The use of computerised systems is absolutely essential when dealing with multiple-victim events with a large number of corpses, as manual comparison of antemortem and postmortem dental data is impossible.
Conclusions on the oral identification - the identification reportThe final step in the comparison process is to draw conclusions about the odontostomatological identification. In making the tooth-by-tooth comparison, similarities, discrepancies or exclusions should be noted as they occur. Similarities are antemortem and postmortem characteristics that coincide. Discrepancies are findings that do not match, but some of them may have an explanation. For example, a tooth may be present in the antemortem records and absent in the postmortem ones, as it may have been extracted. In the same vein, a discrepancy could be explained by the presence of a cavity in an antemortem tooth and the filling of the same tooth in the postmortem records. If the discrepancies can be explained, identification may be possible. When the discrepancies are totally unexplained and there has been no error in the process, identification is not possible with that person and is excluded. Dental identification will therefore be made on the basis that there are no absolute discrepancies, that relative discrepancies can be explained with reasonable logic, and on the existence of coincidences. Points of coincidence must be documented as well as possible in order to demonstrate them. Although the requirement of a minimum number of coincidences is not deduced from reading the scientific literature on the subject, the identity conclusion will be all the more consistent the greater the number of coincidence points or the more unusual the finding.
It would be desirable to be able to present figures on the probability of identification or the degree of certainty of the same. However, given the current state of odontostomatological science it is not yet possible to make a precise estimate in terms of probability, since this requires knowing the exact frequencies of the presentation of the different dental diseases and treatments and their variations related to age. This has been done for some populations.32 When the results cannot be expressed in precise terms of probabilities, the conclusions obtained after the comparison should be those recommended by the ABFO and the International Organisation of Forensic Odonto-Stomatology, as follows:
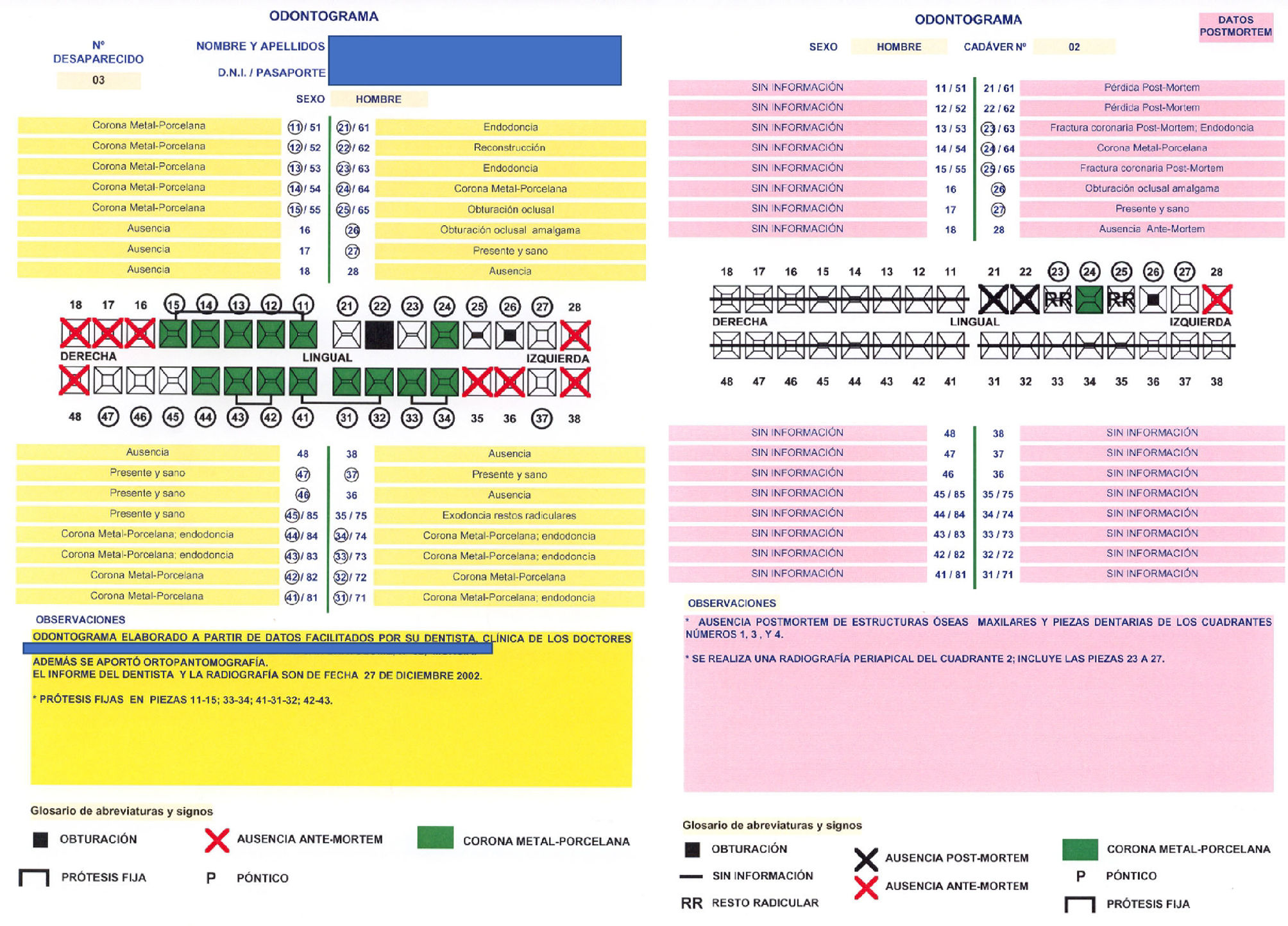
Positive or Established Dental Identity: This conclusion is reached when antemortem and postmortem data agree strongly enough to establish that they belong to the same individual. Also, there are no unexplained discrepancies. Although it cannot be totally ruled out that any other person by chance would have the same type of finding, it does have at least 12 matching features, or a probability of ≤1/10,000, that any other person in the general population will match; the probability of error is so low that we could conclude that it is the same person. The identification can be established based on the coincidence of the dental study, even without other indications. As an example, Fig. 3 shows the process of comparing odontograms, in a case of established dental identity.

Probable dental identity: in this case the dental evidence is strong, but it needs to be supported by other biological, physical, technical and/or tactical findings. In these cases there are between 6 and 11 matching features, or an estimated probability of ≤1/100 that anyone else matches.
Possible dental identity: there are similar characteristics, but none are consistent enough to establish positive identification of the cadaver. The discrepancies have possible explanations and there is no excluding characteristic. If there are 5 or fewer matching characteristics, it will be necessary to resort to other types of techniques that study the possible identity of the subject.
Dental identity excluded: with the existence of a single discrepancy that cannot have a possible explanation, the identity of the subject is excluded. However, one must take into account the possibility of errors made by both the dentist and the forensic odontologist.
The recognition of the individualising characteristics of dental pieces, and oral data in general, is a specialised process that necessarily involves the collaboration of forensic odontologists with experience in this field, possessing the necessary training and knowledge for record taking, precise interpretation of the results, and appropriate obtainment of the conclusions. In the medical/legal report on the identification of the victim, after the medical/legal considerations on the possibilities and limitations of the identification technique used, all matching details on which the identification is based must be described, together with their degree of certainty.
FundingFunding of the open access fee: University of Granada / CBUA.
Please cite this article as: Valenzuela-Garach A. La odontología en la identificación de sucesos con víctimas múltiples. Revista Española de Medicina Legal. 2023. https://doi.org/10.1016/j.reml.2022.11.005.