




Vacunas COVID-19: desarrollo y práctica - COVID-19 vaccines: development and practice
More infoSeasonal fruit workers are a high-risk group for SARS-COV-2 infection. We aimed to estimate vaccination coverage and factors associated with vaccination in seasonal fruit workers.
MethodsWe carried out an anonymous survey of seasonal fruit workers in the 2021 campaign in Baix Segria region and Lleida city (Spain) on vaccination, knowledge and attitudes about the COVID-19 vaccine. Univariate and bivariate descriptive analyses were performed comparing vaccinated versus non-vaccinated. Multivariate analysis was performed using to assess factors associated to vaccination uptake.
ResultsWe included 286 seasonal workers. The prevalence of confirmed COVID-19 background was 39.5% and overall vaccination coverage was 78.7%. Factors associated with vaccination were age (aOR = 0.96; 95% CI: 0.94–0.99), good knowledge of disease (aOR = 1.87; 95% CI : 1.01–3.47) and having a high-perceived vaccine effectiveness (aOR = 2.94; 95% CI : 1.50–5.73). High vaccination coverage in workers was associated to knowledge (OR = 3.69; 95% CI: 1.61–8.48), safe transport (OR = 2.84; 95% CI: 1.40–5.76) and appropriate housing (OR = 2.62; 95% CI: 1.25–5.46) as important non-pharmacological measures to reduced transmission.
ConclusionThe study confirms the high prevalence of COVID-19 history and moderate vaccination coverage in seasonal fruit workers. Health education programs to improve knowledge about COVID-19 and its vaccination can help improve vaccination uptake.
Los trabajadores temporales de la fruta son un grupo de alto riesgo de infección por SARS-COV-2. El objetivo fue estimar la cobertura vacunal y los factores asociados a la vacunación en los trabajadores temporales de la fruta.
MétodosSe realizó una encuesta anónima a los temporeros de la campaña de la fruta 2021 en la comarca del Baix Segrià y en la ciudad de Lleida sobre la vacunación, y los conocimientos y actitudes sobre la vacuna de la COVID-19. Se realizaron análisis descriptivos y bivariantes comparando los vacunados con los no vacunados y se realizó un análisis multivariante para evaluar los factores asociados a la vacunación.
ResultadosSe incluyeron 286 trabajadores temporales. La prevalencia de haber sido COVID-19 confirmado previamente fue del 39,5% y la cobertura global de vacunación fue del 78,7%. Los factores asociados a la vacunación fueron la edad (ORa = 0,96; IC 95%: 0,94-0,99), el conocimiento correcto de la enfermedad (ORa = 1,87; IC 95% : 1,01-3,47) y tener una alta percepción de la eficacia de la vacuna (ORa = 2,94; IC 95% : 1,50-5,73). Se observó una alta cobertura vacunal en los trabajadores manifestaron que los conocimientos de la enfermedad (OR = 3,69; IC 95%: 1,61-8,48), el transporte seguro (OR = 2,84; IC 95%: 1,40-5,76) y el alojamiento adecuado (OR = 2,62; IC 95%: 1,25-5,46) son importantes medidas para reducir la transmisión.
ConclusionesEl estudio confirma la alta prevalencia de haber pasado la COVID-19 y la moderada cobertura de vacunación en los trabajadores estacionales de la fruta. Los programas de educación sanitaria para mejorar el conocimiento sobre el COVID-19 y su vacunación pueden ayudar a mejorar la aceptación de la vacunación.
Congregate workplaces and residential locations have an increased risk of infectious disease transmission, including respiratory disease outbreaks. COVID-19 is an infectious disease caused by SARS-COV-2, which spreads from person to person through respiratory droplets.1 Most people have mild respiratory symptoms, but when transmission increases, a percentage of patients may develop severe disease and require hospital care and even admission to the Intensive Care Unit (ICU).2
Several studies3,4,5,6 have reported a high risk of spread of SARS COV-2 in workers in the meat and poultry industries, all of them considered essential services. In these industries, as in the seasonal fruit campaign, people may work without safety distance and workers may have inadequate knowledge of non-pharmacological measures.3 However, few studies have described prevalence and outbreaks of SARS-CoV-2 in seasonal fruit workers.7,8,9
In July 2020, there was a very important outbreak of SARS-CO-2 in the region of Segrià (Lleida, Spain), one of the most important agricultural fruit regions in Europe. Most of the cases in this outbreak were migrant and seasonal fruit workers. The outbreak caused an increase in transmission at the community level in the region as a whole causing an increase in hospital pressure. Through this outbreak, an inadequate knowledge of non-pharmacological preventive measures were observed, especially among seasonal workers.10 Given this situation, at the beginning of the 2021 fruit season, a vaccination campaign was implemented connecting directly with employers of emigrant/migratory and seasonal fruit workers. Due to special circumstances, employers often provide information on transportation, housing, and health. For this reason, employers were willing to facilitate workplace vaccination or provide transportation for employees to vaccination centers. Because migrant/migratory and seasonal food and agriculture workers are a difficult group to access, it is especially important to document vaccination uptake among these workers. At the same time, different health education interventions were carried out for the different workers involved in the fruit campaign in order to promote knowledge and attitudes to prevent the transmission of the virus.
The present study aimed to estimate vaccination coverage and factors associated with vaccination in seasonal fruit workers and to study the influence of knowledge, attitudes and behaviours on vaccination uptake.
Material and methodsStudy population and settingThis is a prevalence study of seasonal workers who were working in the 2021 in the fruit campaign in Baix Segrià sub-region and Lleida city. This area is located in the south-west of the Segrià region (western Catalonia, Spain), with a population of 160,282 inhabitants distributed in 8 municipalities (Aitona, Alcarràs, Granja d'Escarp, Massalcoreig, Seròs, Soses, Torres de Segre and Lleida city). Every year in June, during the fruit season campaign, this region receives a population of about 30,000 temporary workers.
A survey was designed to collect information on vaccination and the importance of non-pharmacological measures to prevent SARS-COV-2 transmission. The survey was conducted between July 01 and July 30 2021, through personal interview by trained staff. To assess the structure, feasibility, comprehensibility and completion time of questionnaire, we carried out a pilot study on a convenience sample of 30 participants.
By a cluster sampling, we selected 10% of the total number of workers identified in the main fruit companies (N = 286). From each company, a proportional number of workers to interview was calculated based on the total number of workers registered in the census. Because these seasonal workers are people difficult to contact, training staff went to the companies to carry out the surveys.
Study variablesFor the current study, sociodemographic data included were age and gender. To collect background and attitudes towards SARS-COV-2, the following questions were asked: have you been a confirmed case previously?; have you ever been quarantined?; if you had a fever, cough or sore throat, would you suspect that you were infected with Covid-19?; if you have these symptoms (fever, cough or sore throat) you will isolate yourself preventively?; and if you were a confirmed COVID-19 you would disclose close contacts?. Additionally we collected the assessment of self-perceived severity of the disease with a Likert scale from 1 to 5 (1 = mild disease; 5 = severe disease). To assess knowledge of the disease, we asked about the most frequent incubation period with different options (only one answer was correct). To collect information of COVID-19 vaccine, we included vaccine perceived effectiveness using a Likert scale from 1 to 5 (1 = not effective; 5 = very effective) and if he/she has been vaccinated or would be vaccinated if they could.
Finally, perceived importance of the following 11 measures to reduce the transmission of SARS-COV-2 was collected using a Likert scale from 1 to 5 (1 = not important; 5 = very important): 1. Handwashing, 2. Use of masks, 3. Safety distance, 4. Cases isolation, 5. Contacts quarantine, 6. Use of tests (PCR, TAR), 7. Knowledge of the disease, 8. Safe transport, 9. Appropriate housing, 10. Adapted dining rooms, and 11. Frequent ventilation.
Statistical analysisUnivariate and bivariate descriptive analyses were performed comparing vaccinated versus non-vaccinated participants, using percentages for qualitative variables and means and standard deviation for quantitative variables. Statistical significance between groups were estimated using the chi-squared test and t-student test.
Additionally, the strength of association for each studied factor on vaccination status (vaccinated versus non-vaccinated) in seasonal fruit workers was calculated using Odds Ratio (ORs) and their 95% CIs. The estimated ORs were adjusted (aOR) by age, sex, confirmed case previously, be a contact before, severity of disease, incubation period and vaccine effectiveness.
Data management and statistical analyses were performed using the IBM SPSS Statistics program, version 18. Statistical significance was set at p < 0.05.
Ethical aspectsThe study was approved by the Ethics Committees of Arnau de Vilanova Hospital (code: CEIC-2503). All the participants were informed about the study and gave their consent to participate.
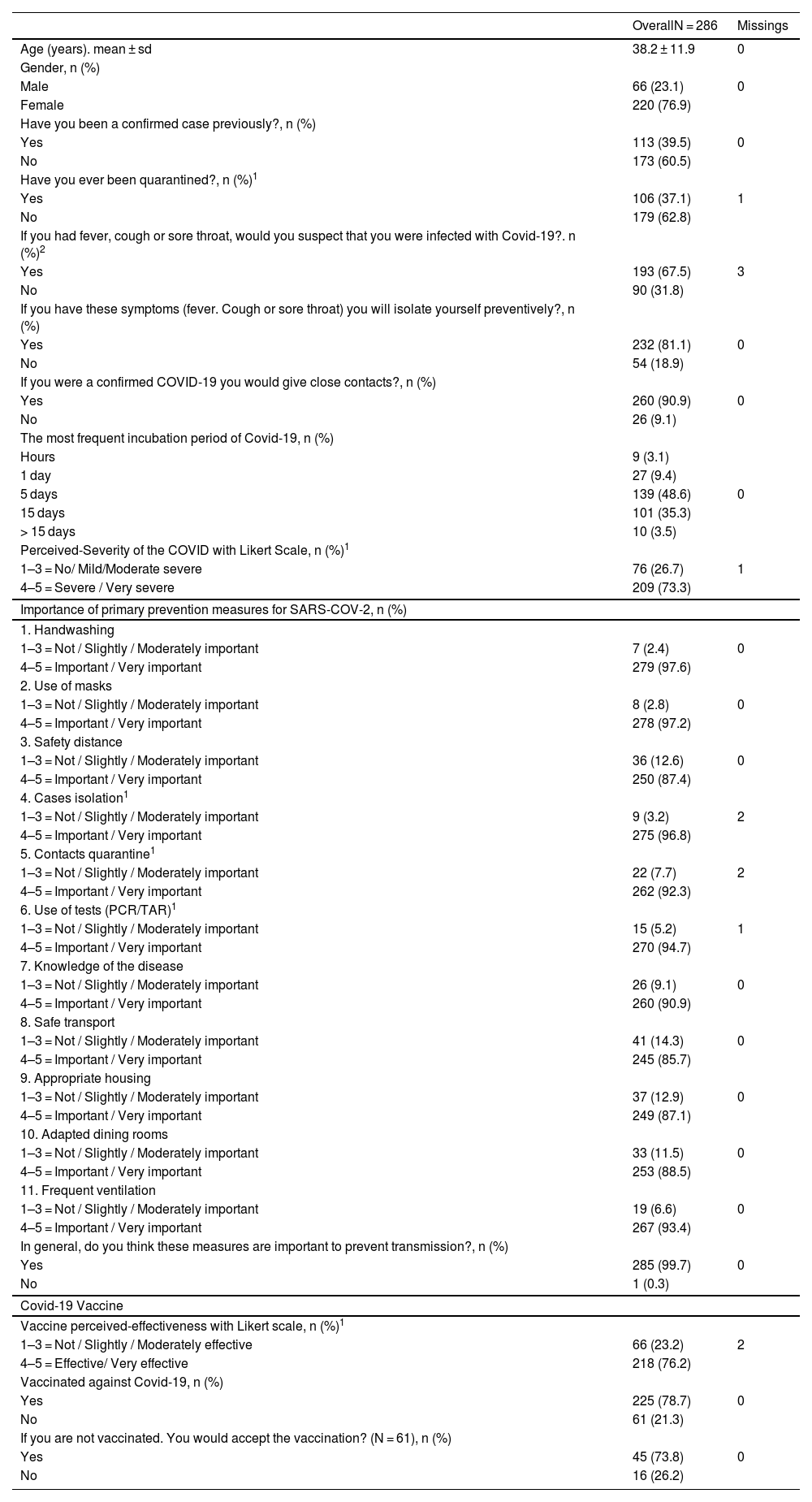
ResultsWe surveyed 286 seasonal fruit workers with a mean age of 38.2 years (± 11.9), of whom 220 (76.9%) were female. The prevalence of having been a previously confirmed case and had to be quarantined before were 39.5% and 37.1%; respectively. Participants report that if they had a fever, cough or sore throat only 67.5% would suspect that they might be sick with Covid-19 and 81.1% would isolate themselves preventively if they had any symptoms. Only 9.1% of the participants would not be willing to disclose close contacts. The vaccination coverage of participants included was 78.7%. In addition, of the 61 unvaccinated, 45 (73.8%) wanted to be vaccinated. (Table 1).
Characteristics of Seasonal Fruit Workers surveyed.
| OverallN = 286 | Missings | |
|---|---|---|
| Age (years). mean ± sd | 38.2 ± 11.9 | 0 |
| Gender, n (%) | ||
| Male | 66 (23.1) | 0 |
| Female | 220 (76.9) | |
| Have you been a confirmed case previously?, n (%) | ||
| Yes | 113 (39.5) | 0 |
| No | 173 (60.5) | |
| Have you ever been quarantined?, n (%)1 | ||
| Yes | 106 (37.1) | 1 |
| No | 179 (62.8) | |
| If you had fever, cough or sore throat, would you suspect that you were infected with Covid-19?. n (%)2 | ||
| Yes | 193 (67.5) | 3 |
| No | 90 (31.8) | |
| If you have these symptoms (fever. Cough or sore throat) you will isolate yourself preventively?, n (%) | ||
| Yes | 232 (81.1) | 0 |
| No | 54 (18.9) | |
| If you were a confirmed COVID-19 you would give close contacts?, n (%) | ||
| Yes | 260 (90.9) | 0 |
| No | 26 (9.1) | |
| The most frequent incubation period of Covid-19, n (%) | ||
| Hours | 9 (3.1) | |
| 1 day | 27 (9.4) | |
| 5 days | 139 (48.6) | 0 |
| 15 days | 101 (35.3) | |
| > 15 days | 10 (3.5) | |
| Perceived-Severity of the COVID with Likert Scale, n (%)1 | ||
| 1–3 = No/ Mild/Moderate severe | 76 (26.7) | 1 |
| 4–5 = Severe / Very severe | 209 (73.3) | |
| Importance of primary prevention measures for SARS-COV-2, n (%) | ||
| 1. Handwashing | ||
| 1–3 = Not / Slightly / Moderately important | 7 (2.4) | 0 |
| 4–5 = Important / Very important | 279 (97.6) | |
| 2. Use of masks | ||
| 1–3 = Not / Slightly / Moderately important | 8 (2.8) | 0 |
| 4–5 = Important / Very important | 278 (97.2) | |
| 3. Safety distance | ||
| 1–3 = Not / Slightly / Moderately important | 36 (12.6) | 0 |
| 4–5 = Important / Very important | 250 (87.4) | |
| 4. Cases isolation1 | ||
| 1–3 = Not / Slightly / Moderately important | 9 (3.2) | 2 |
| 4–5 = Important / Very important | 275 (96.8) | |
| 5. Contacts quarantine1 | ||
| 1–3 = Not / Slightly / Moderately important | 22 (7.7) | 2 |
| 4–5 = Important / Very important | 262 (92.3) | |
| 6. Use of tests (PCR/TAR)1 | ||
| 1–3 = Not / Slightly / Moderately important | 15 (5.2) | 1 |
| 4–5 = Important / Very important | 270 (94.7) | |
| 7. Knowledge of the disease | ||
| 1–3 = Not / Slightly / Moderately important | 26 (9.1) | 0 |
| 4–5 = Important / Very important | 260 (90.9) | |
| 8. Safe transport | ||
| 1–3 = Not / Slightly / Moderately important | 41 (14.3) | 0 |
| 4–5 = Important / Very important | 245 (85.7) | |
| 9. Appropriate housing | ||
| 1–3 = Not / Slightly / Moderately important | 37 (12.9) | 0 |
| 4–5 = Important / Very important | 249 (87.1) | |
| 10. Adapted dining rooms | ||
| 1–3 = Not / Slightly / Moderately important | 33 (11.5) | 0 |
| 4–5 = Important / Very important | 253 (88.5) | |
| 11. Frequent ventilation | ||
| 1–3 = Not / Slightly / Moderately important | 19 (6.6) | 0 |
| 4–5 = Important / Very important | 267 (93.4) | |
| In general, do you think these measures are important to prevent transmission?, n (%) | ||
| Yes | 285 (99.7) | 0 |
| No | 1 (0.3) | |
| Covid-19 Vaccine | ||
| Vaccine perceived-effectiveness with Likert scale, n (%)1 | ||
| 1–3 = Not / Slightly / Moderately effective | 66 (23.2) | 2 |
| 4–5 = Effective/ Very effective | 218 (76.2) | |
| Vaccinated against Covid-19, n (%) | ||
| Yes | 225 (78.7) | 0 |
| No | 61 (21.3) | |
| If you are not vaccinated. You would accept the vaccination? (N = 61), n (%) | ||
| Yes | 45 (73.8) | 0 |
| No | 16 (26.2) | |
sd: standard deviation.
n: absolute number.
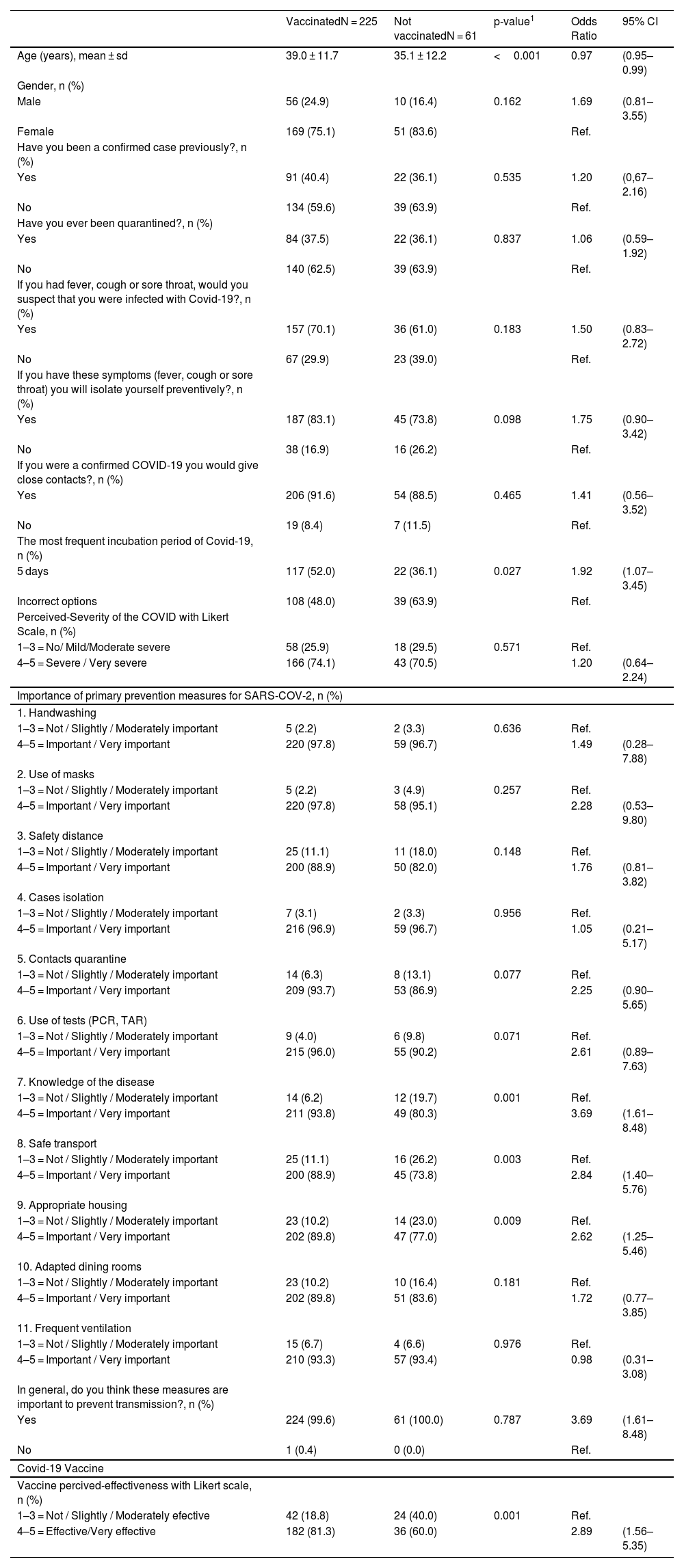
Table 2 shows absolute numbers and percentages of vaccinated versus not-vaccinated workers for factors influencing on vaccination status. We observed 225 workers vaccinated, with a mean age ± standard deviation of 39.0 years ±11.7, of whom 75.1% were female. On the other hand, 61 workers were not vaccinated with a mean age ± standard deviation of 35.1 years ±12.2, of whom 83.6% were female. The prevalence of having been a previously confirmed case in vaccinated and not-vaccinated workers were 40.4% and 36.1%, respectively.
Descriptive and Bivariate logistic regression of factors associated with vaccination coverage in seasonal fruit workers.
| VaccinatedN = 225 | Not vaccinatedN = 61 | p-value1 | Odds Ratio | 95% CI | |
|---|---|---|---|---|---|
| Age (years), mean ± sd | 39.0 ± 11.7 | 35.1 ± 12.2 | <0.001 | 0.97 | (0.95–0.99) |
| Gender, n (%) | |||||
| Male | 56 (24.9) | 10 (16.4) | 0.162 | 1.69 | (0.81–3.55) |
| Female | 169 (75.1) | 51 (83.6) | Ref. | ||
| Have you been a confirmed case previously?, n (%) | |||||
| Yes | 91 (40.4) | 22 (36.1) | 0.535 | 1.20 | (0,67–2.16) |
| No | 134 (59.6) | 39 (63.9) | Ref. | ||
| Have you ever been quarantined?, n (%) | |||||
| Yes | 84 (37.5) | 22 (36.1) | 0.837 | 1.06 | (0.59–1.92) |
| No | 140 (62.5) | 39 (63.9) | Ref. | ||
| If you had fever, cough or sore throat, would you suspect that you were infected with Covid-19?, n (%) | |||||
| Yes | 157 (70.1) | 36 (61.0) | 0.183 | 1.50 | (0.83–2.72) |
| No | 67 (29.9) | 23 (39.0) | Ref. | ||
| If you have these symptoms (fever, cough or sore throat) you will isolate yourself preventively?, n (%) | |||||
| Yes | 187 (83.1) | 45 (73.8) | 0.098 | 1.75 | (0.90–3.42) |
| No | 38 (16.9) | 16 (26.2) | Ref. | ||
| If you were a confirmed COVID-19 you would give close contacts?, n (%) | |||||
| Yes | 206 (91.6) | 54 (88.5) | 0.465 | 1.41 | (0.56–3.52) |
| No | 19 (8.4) | 7 (11.5) | Ref. | ||
| The most frequent incubation period of Covid-19, n (%) | |||||
| 5 days | 117 (52.0) | 22 (36.1) | 0.027 | 1.92 | (1.07–3.45) |
| Incorrect options | 108 (48.0) | 39 (63.9) | Ref. | ||
| Perceived-Severity of the COVID with Likert Scale, n (%) | |||||
| 1–3 = No/ Mild/Moderate severe | 58 (25.9) | 18 (29.5) | 0.571 | Ref. | |
| 4–5 = Severe / Very severe | 166 (74.1) | 43 (70.5) | 1.20 | (0.64–2.24) | |
| Importance of primary prevention measures for SARS-COV-2, n (%) | |||||
| 1. Handwashing | |||||
| 1–3 = Not / Slightly / Moderately important | 5 (2.2) | 2 (3.3) | 0.636 | Ref. | |
| 4–5 = Important / Very important | 220 (97.8) | 59 (96.7) | 1.49 | (0.28–7.88) | |
| 2. Use of masks | |||||
| 1–3 = Not / Slightly / Moderately important | 5 (2.2) | 3 (4.9) | 0.257 | Ref. | |
| 4–5 = Important / Very important | 220 (97.8) | 58 (95.1) | 2.28 | (0.53–9.80) | |
| 3. Safety distance | |||||
| 1–3 = Not / Slightly / Moderately important | 25 (11.1) | 11 (18.0) | 0.148 | Ref. | |
| 4–5 = Important / Very important | 200 (88.9) | 50 (82.0) | 1.76 | (0.81–3.82) | |
| 4. Cases isolation | |||||
| 1–3 = Not / Slightly / Moderately important | 7 (3.1) | 2 (3.3) | 0.956 | Ref. | |
| 4–5 = Important / Very important | 216 (96.9) | 59 (96.7) | 1.05 | (0.21–5.17) | |
| 5. Contacts quarantine | |||||
| 1–3 = Not / Slightly / Moderately important | 14 (6.3) | 8 (13.1) | 0.077 | Ref. | |
| 4–5 = Important / Very important | 209 (93.7) | 53 (86.9) | 2.25 | (0.90–5.65) | |
| 6. Use of tests (PCR, TAR) | |||||
| 1–3 = Not / Slightly / Moderately important | 9 (4.0) | 6 (9.8) | 0.071 | Ref. | |
| 4–5 = Important / Very important | 215 (96.0) | 55 (90.2) | 2.61 | (0.89–7.63) | |
| 7. Knowledge of the disease | |||||
| 1–3 = Not / Slightly / Moderately important | 14 (6.2) | 12 (19.7) | 0.001 | Ref. | |
| 4–5 = Important / Very important | 211 (93.8) | 49 (80.3) | 3.69 | (1.61–8.48) | |
| 8. Safe transport | |||||
| 1–3 = Not / Slightly / Moderately important | 25 (11.1) | 16 (26.2) | 0.003 | Ref. | |
| 4–5 = Important / Very important | 200 (88.9) | 45 (73.8) | 2.84 | (1.40–5.76) | |
| 9. Appropriate housing | |||||
| 1–3 = Not / Slightly / Moderately important | 23 (10.2) | 14 (23.0) | 0.009 | Ref. | |
| 4–5 = Important / Very important | 202 (89.8) | 47 (77.0) | 2.62 | (1.25–5.46) | |
| 10. Adapted dining rooms | |||||
| 1–3 = Not / Slightly / Moderately important | 23 (10.2) | 10 (16.4) | 0.181 | Ref. | |
| 4–5 = Important / Very important | 202 (89.8) | 51 (83.6) | 1.72 | (0.77–3.85) | |
| 11. Frequent ventilation | |||||
| 1–3 = Not / Slightly / Moderately important | 15 (6.7) | 4 (6.6) | 0.976 | Ref. | |
| 4–5 = Important / Very important | 210 (93.3) | 57 (93.4) | 0.98 | (0.31–3.08) | |
| In general, do you think these measures are important to prevent transmission?, n (%) | |||||
| Yes | 224 (99.6) | 61 (100.0) | 0.787 | 3.69 | (1.61–8.48) |
| No | 1 (0.4) | 0 (0.0) | Ref. | ||
| Covid-19 Vaccine | |||||
| Vaccine percived-effectiveness with Likert scale, n (%) | |||||
| 1–3 = Not / Slightly / Moderately efective | 42 (18.8) | 24 (40.0) | 0.001 | Ref. | |
| 4–5 = Effective/Very effective | 182 (81.3) | 36 (60.0) | 2.89 | (1.56–5.35) | |
sd: standard deviation.
n: absolute number.
CI: Confidence Interval.
We observed higher vaccination coverage in men than in women (OR = 1.69; 95% CI: 0.81–3.55); but differences were not statistically significant.
Statistically significant differences were observed by age, knowledge of the disease (verified with a correct answer about incubation period) and perceived effectiveness of vaccine. Vaccination coverage in young workers was lower (OR = 0.97; 95% CI: 0.95–0.99). In contrast, vaccination coverage was significantly higher in workers with good knowledge of the disease (OR = 1.92; 95% CI: 1.07–3.45) and with high perceived effectiveness of vaccine (OR = 2.89; 95% CI:1.56–5.35).
When looking at the perceived importance of the measures to reduce the transmission of SARS-COV-2 we observed a statistically significant high vaccination coverage in workers that perceiving knowledge (OR = 3.69; 95% CI: 1.61–8.48), safe transport (OR = 2.84; 95% CI: 1.40–5.76) and appropriate housing (OR = 2.62; 95% CI: 1.25–5.46) as important measures to reduce transmission. No significant differences in vaccine coverage were observed for other factors studied (Table 2).
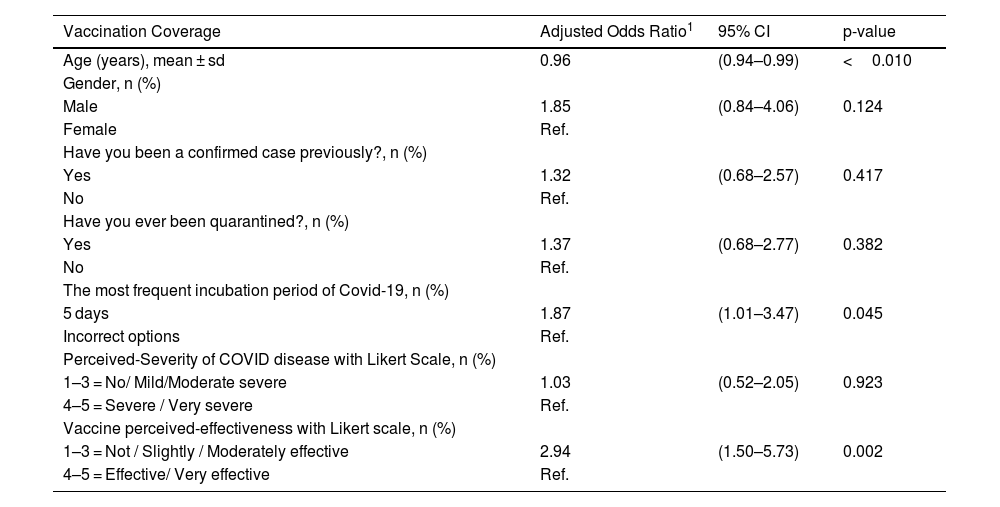
In multivariate analysis, vaccination coverage increases with age (aOR = 0.96; 95% CI: 0.94–0.99), in people with knowledge of the disease (aOR = 1.87; 95% CI = 1.01–3.47) and with a high-perceived effectiveness of the vaccine (aOR = 2.94; 95% CI = 1.50–5.73) (Table 3).
Multivariate logistic regression of factors associated with vaccination coverage in seasonal fruit workers.
| Vaccination Coverage | Adjusted Odds Ratio1 | 95% CI | p-value |
|---|---|---|---|
| Age (years), mean ± sd | 0.96 | (0.94–0.99) | <0.010 |
| Gender, n (%) | |||
| Male | 1.85 | (0.84–4.06) | 0.124 |
| Female | Ref. | ||
| Have you been a confirmed case previously?, n (%) | |||
| Yes | 1.32 | (0.68–2.57) | 0.417 |
| No | Ref. | ||
| Have you ever been quarantined?, n (%) | |||
| Yes | 1.37 | (0.68–2.77) | 0.382 |
| No | Ref. | ||
| The most frequent incubation period of Covid-19, n (%) | |||
| 5 days | 1.87 | (1.01–3.47) | 0.045 |
| Incorrect options | Ref. | ||
| Perceived-Severity of COVID disease with Likert Scale, n (%) | |||
| 1–3 = No/ Mild/Moderate severe | 1.03 | (0.52–2.05) | 0.923 |
| 4–5 = Severe / Very severe | Ref. | ||
| Vaccine perceived-effectiveness with Likert scale, n (%) | |||
| 1–3 = Not / Slightly / Moderately effective | 2.94 | (1.50–5.73) | 0.002 |
| 4–5 = Effective/ Very effective | Ref. |
The study documents high COVID-19 vaccination coverage (78.9%) in seasonal fruit workers through a vaccination program coordinated with employers and health centres, in an area where an important COVID-19 outbreak occurred the previous year.
According to the seroprevalence report, the global cumulative prevalence of Covid-19 in November 2020 in Spain was 9.9%, in Catalonia 11.6% and in Lleida 12.2% 11. In our study, we observed the high prevalence of confirmed COVID history among workers (39.5%) and the high percentage of previous quarantine indicates that it is a high-risk group for SARS-CoV-2 infection. However, knowledge about the disease seems limited since only 67.5% would suspect of being affected by COVID-19 with compatible symptoms of the disease. Different outbreaks reported in these workers confirm the high risk of infection and suggest the importance of improving their knowledge and working and housing conditions 3,6,12.
Vaccination of COVID-19 in temporary fruit workers was associated with older age, with better knowledge of the disease (verified with a correct answer about the incubation period) and a good opinion on the effectiveness of the vaccine. According to the literature,13--18 our study reflects that vaccination coverage is higher in the older age group. This could be attributed to the fact that older adults have a higher risk of comorbidities and mortality than young adults. Risk perception plays a crucial role as a predictor of protection intentions and preventive health behaviours. In addition, we observed a non-statistically significant higher vaccination coverage in men than in women, which has also been observed in other studies.19--21
Several publications have reported greater acceptance of the COVID-19 vaccine based on knowledge of the disease 13,15,22,23 and self-perceived effectiveness of the vaccine.23--25 These previous studies showed that increasing the population's consciousness about disease severity and benefits of vaccine could improve their willingness to be vaccinated. Therefore, public health interventions should focus on providing adequate information to the public, both on the disease and on the evidence of safety and efficacy of vaccines from reliable trials.
Vaccination was also higher among workers who believed that safe transportation to the workplace, adequate housing, and knowledge of the disease were important to prevent COVID-19. One study in healthy primary healthcare workers on pandemic influenza vaccination also observed better coverage of vaccination in workers with good knowledge about the incubation period of the disease and of the opinion that the vaccine was effective.26 In general, the percentages in the perception of the importance of non-pharmacological measures in the prevention of SARS-COV-2 transmission are higher in vaccinated workers than in unvaccinated workers and differences were observed in the measures of knowledge of the disease, safe transport and adequate housing.
The multivariate analysis confirmed the implication of age, the correct knowledge about the incubation period of COVID-19 and the opinion that the vaccine is effective. All this suggests that health education programs to improve knowledge about COVID-19 and gain positive opinions and attitudes about vaccination can improve vaccination coverage. In addition, improving work and housing conditions together with knowledge about compatible symptoms and the importance of complying with quarantines and identifying contacts can reduce transmission in the high-risk group.1,27,28
Several studies have been conducted on attitudes of general population or healthcare workers towards COVID-19 vaccines and potential influencing factors.29,30 However, this is the first study to assess these factors in seasonal fruit workers and also reflects the importance-perceived of non-pharmacological measures to reduce the transmission of SARS-COV-2.
The study has some limitations. The sample of patients was made through direct contact with the companies and it is not a probabilistic sample of all the workers in the region, but all the companies were represented. The interviews were carried out by public health technicians through personal interviews, which could induce some responses, but in the survey the interviewers could confirm that the respondents were not identified and that the information was anonymous. The vaccination was self-reported by the workers, but since the surveys were carried out very close to the days of the vaccination, it is considered that there were few wrong answers.
The study confirms that high vaccination uptake can be achieved in seasonal fruit workers through vaccination strategies coordinated with employers and health centres. Health education programs to improve knowledge about COVID-19 and its vaccination can help improve vaccination uptake.
FundingThere was no funding source for this study.