

Urothelial bladder carcinoma (UBC), the most frequent type (90%) of bladder cancer and the second most common malignancy of the urogenital region, is a relatively well understood type of cancer, with numerous studies concerning pathogenetic pathways, natural history and bladder tumor biology being reported. Despite this, it continues to remain a challenge in the oncology field, mostly due to its relapsing and progressive nature, and to the heterogeneity in the response to cisplatin-containing regimens. Although the formulae based on clinical staging and histopathological parameters are classically used as diagnostic and prognostic tools, they have proven insufficient to characterize the individual biological features and clinical behaviour of the tumours. Understanding the pathobiology of the disease can add important information to these classical criteria, and contribute to accurately predict outcome and individualize therapy for UBC patients. In this line of investigation, we found that tumour angiogenesis and lymphangiogenesis, the process of invasion and metastasis and the energy metabolism reprogramming/tumour microenvironment encompass several potential biomarkers that seem to infl bladder cancer aggressiveness and chemoresistance. We particularly highlight the roles of lymphovascular invasion, and of RKIP, CD147 and MCT1 immunoexpressions, as relevant prognostic and/or predictive biomarkers, and as promising areas of therapeutic intervention, eliciting for the development of additional studies that can validate and further explore these biomarkers.
O carcinoma urotelial da bexiga (CUB), o tipo de cancro mais frequente deste órgão (90%) e o segundo mais comum da região genitourinária, está relativamente bem caracterizado, fundamentado por inúmeros estudos sobre vias patogenéticas, histogénese e biologia tumoral. No entanto, permanece como um desafio na oncologia, principalmente devido à sua elevada taxa de recidiva e progressão, e à heterogeneidade na resposta a tratamentos de quimioterapia contendo cisplatina. As fórmulas baseadas no estadiamento tumoral e em parâmetros histopatológicos, embora geralmente utilizadas como ferramentas de diagnóstico e prognóstico, são insuficientes para caracterizar as propriedades biológicas e o comportamento clínico dos tumores. A compreensão detalhada da patobiologia da doença poderá adicionar informações importantes aos critérios clássicos, e contribuir para uma correta previsão individual do prognóstico e da terapêutica a utilizar nos doentes com CUB. Nesta linha de investigação, o nosso grupo sugere que na angiogénese e na linfangiogénese tumoral, no processo de invasão e metastização e na reprogramação do metabolismo energético/microambiente tumoral estão implicados potenciais biomarcadores que parecem influenciar a agressividade tumoral e a resistência à quimioterapia no CUB. Salienta-se o papel da invasão linfovascular, e da imunoexpressão das moléculas RKIP, CD147 e MCT1, como biomarcadores de prognóstico e/ou preditivos de resposta à terapêutica, e como áreas promissoras de intervenção terapêutica. É urgente desenvolver estudos adicionais que continuem a explorar e, eventualmente, validar as potencialidades destes biomarcadores.
Thirteen years ago, Hanahan and Weinberg suggested that, although encompassing variable mechanistic strategies, cancers in general acquire a set of functional biological capabilities during their multistep development. These include sustaining proliferative signaling, evading growth suppressors, resisting cell death, enabling replicative immortality, inducing angiogenesis, and activating invasion and metastasis.1 In their recent review, the authors added to their previous model two enabling characteristics and two emerging hallmarks. They considered that genome instability generates the genetic diversity underlying the acquisition of all hallmarks, and that inflammation promotes multiple hallmark functions. Additionally, the establishment of a tumour microenvironment by the malignant cells but also by recruited normal cells importantly contributes to energy metabolism reprogramming and immune destruction evasion in order to effectively support neoplastic proliferation.2 This molecular knowledge is already being applied into clinical practice, with targeted therapies that interfere with each of the hallmarks being developed and entering in clinical trial phase or, in some cases, being approved for clinical use in treating certain forms of human cancer.3-5
In urothelial bladder cancer (UBC) setting, although a reasonable number of biomarkers seem to be prognostically relevant,6,7 there is a substantial delay in the translation into the clinics, and clinical trials with molecularly targeted agents have been few in number and largely unsuccessful.8,9. This is probably due to the unique complexity involved in the dual-track pathway of bladder carcinogenesis, which postulates that UBC develops via two distinct but somewhat overlapping pathways, resulting in two main phenotypic variants with different biological behaviours and prognoses.10 However, areas in which biomarkers may prove valuable are evident, encompassing the three most important risk factors that threaten survival and life quality of bladder cancer patients.7 First, the majority of UBCs emerge as non-muscle invasive (NMI), low grade, papillary lesions. Due to their high risk of recurrence, current guidelines recommend intense follow-up that classically relies on invasive techniques such as cystoscopy and biopsy, causing significant patient discomfort and implicating substantial costs. Thus, prediction of tumour recurrence through non-invasive methods would be of great value.11 Second, an important proportion of NMI tumours, such as high grade or carcinoma in situ lesions, incur at an increased risk of progression to muscle-invasive (MI) disease. Timely prediction of progression would guide a vigilant surveillance, and would help clinicians to identify patients in need of early, aggressive management, while avoiding over-treatment in others.12 Third, the risk of metastasis is the main pitfall for MI-UBC patients, and the majority of bladder cancer deaths occur as a consequence of metastatic disease.13 Although cisplatin-containing chemotherapy is recommended for locally-advanced or metastatic UBC,14 survival benefits are impaired in up to 50% of the patients due to chemoresistance and patient fragility.15 In this scenario, robust biomarkers could help to identify circulating or lymph-node occult micrometastases, could represent potential therapeutic targets, and could forecast and stratify responses to conventional cytotoxic therapies or to emerging targeted therapies (the so called companion biomarkers).9,16-18 Hence, UBC represents a considerable opportunity and challenge for biomarkers’ research.
In the last years, efforts have been taken to uncover prognostic and/or predictive biomarkers that might be useful in the clinical care of UBC patients. Traditional approaches of single-molecule or single-pathway profiling are being replaced by investigations on panels of biomarkers encompassing several hallmarks of cancer.7,19,20 While the few biomarkers of potential clinical relevance that have been identified so far are mainly related to the key molecular pathways of bladder tumourigenesis [e.g. FGFR3 (fibroblast growth factor receptor 3) and TP53 (tumour protein p53) mutations],6,7,21 there is the need to expand the research into poorly explored scenarios of the malignant phenotype, in an attempt to unveil novel promising markers that can be integrated into a molecular signature with accurate prognosis and predictive power. A cancer-related biomarker must be a molecule produced by the tumour, detectable and measurable in patient specimens (tissue, blood or urine), representative of various tumour properties, and reproducible, specific and sensitive.7,22 Several recent reviews have explored the most promising UBC biomarkers, although, to date, no biomarker panel has reached validation for daily clinical practice.6,7,21,23 Immunohistochemical approaches in tissue arrays are well suited for the detection task, by being practical methods that can easily allow the translation of new described biomarkers into clinical practice.24 In this line of investigation, our group used immunohistochemistry to study, in a cohort of well-characterized UBC samples, the clinical and prognostic significance of several poorly studied putative biomarkers encompassing and overlapping three hallmarks of cancer: inducing tumour angiogenesis (and lymphangiogenesis), activating invasion and metastasis, and reprogramming cellular energetics and the tumour microenvironment. We additionally performed validation assays with bladder cancer cell lines. Our research efforts have resulted in important findings concerning some biological parameters that seem to influence bladder cancer aggressiveness and chemoresistance. In the next sections, we will explore the state of the art of these evolving hallmarks, and provide our contribution in unveiling potential prognosis and predictive biomarkers, as well as new therapeutic targets, also reviewing the contribution of other authors to the current knowledge on this field.
Tumour angiogenesis and lymphangiogenesisThe dissemination of malignant cells to distant organs from the primary tumour is the leading cause of mortality from cancer and, with few exceptions, all cancers can metastasize.25,26 Although metastasis can occur by local tissue invasion and direct seeding of body cavities, the main routes of dissemination are the hematogenous and lymphogenous spread. Preclinical and clinical studies suggest that the lymphatic vascular system is preferred over the blood vascular system, and occurrence of lymph node metastasis is an important factor for patients’ prognosis and treatment decision-making.27,28 The malignant cells exploit both vascular systems by expressing growth factors that alter the normal pattern of blood and lymphatic vessel growth, creating conduits for metastasis to occur by tumour-induced angiogenesis and lymphangiogenesis.29
The overexpression of angiogenic and lymphangiogenic growth factors in tumours significantly increases blood vessel density (BVD) and lymphatic vessel density (LVD), and establishes the routes for blood vessel invasion (BVI) and lymphatic vessel invasion (LVI) by malignant cells. A significant number of retrospective studies reported significant associations between the occurrence of angiogenesis and BVI, lymphangiogenesis and LVI, and the risk of tumour recurrence, progression, lymph node metastasis, distant metastasis and death for distinct cancer patients.29,30 Blocking the expression of angiogenic and lymphangiogenic growth factors in preclinical models has inhibited tumour growth and expansion of the tumour-associated vasculature, and reduced malignant spread.31,32 Therefore, it is not surprising that novel anti-angiogenic/lymphangiogenic agents and combinations including chemotherapeutic drugs, as well as targeted inhibitors, are currently under clinical trial phase or have already obtained the approval from the Food and Drug Administration for treating cancer patients.
Similarly to other types of cancer, the role of angiogenesis in UBC is well established. Both VEGF (vascular endothelial growth factor) levels and high BVD counts independently predicted progression and lymph node metastasis, significantly lowering survival rates.33-35 Large scale approaches have also confirmed VEGF as an independent prognosis factor.36 Moreover, although studies on lymphangiogenesis occurrence and its usefulness in urothelial malignancies are fewer in number, the general tendency points out for an important task of lymphatic vessel formation in malignant dissemination.37,38 VEGF-C levels were associated with high lymphatic vessel density (LVD) counts, predicting lymph node metastasis.38,39 Both blood and lymphatic vessels participate in the metastatic cascade, and lymphovascular invasion (LI) has been identified as an independent prognostic factor for recurrence and overall survival.40 Importantly, it has been demonstrated that the LI status helps to stratify N0 UBC patients who are at increased risk of bladder cancer recurrence and death.41 Despite these important associations, LI occurrence is not routinely described on the pathology reports, due to the lack of diagnosis reproducibility.42,43
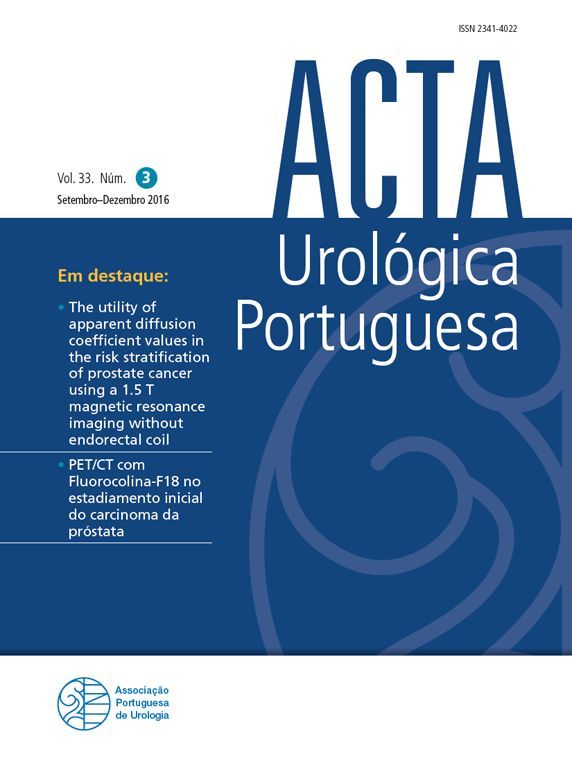
In our research, we assessed angiogenesis, lymphangiogenesis and lymphovascular invasion occurrence in 83 UBC tissue sections, using an immunohistochemical method to differentiate between blood and lymphatic endothelial cells44 (Table 1). We did observe that tumour neovascularization occurrence (Figs. 1A and 1B) determines bladder cancer aggressiveness, although no significant association with outcome variables was found. While contradicting a few prior reports,34,35 others have also failed to demonstrate correlations among BVD and prognosis,45 and it has been advocated that, due to the inconsistency among various studies, BVD alone does not capture the real effect of angiogenesis occurrence on tumour progression and metastasis.21 On the other hand, in our study it was noted that intratumoural lymphatic vessels, described as collapsed and non-functional by some authors,46,47 had visible lumens in a significant proportion of cases, and no edema was observed, which supports an efficient lymphatic flow (Fig. 1B). Moreover, these intratumoural vessels, when functional, seem to actively cooperate in malignant dissemination, as observed by the presence of single malignant cells in the well-preserved intratumoural lymphatic vessels (Fig. 1D), which portended a low overall survival rate. Similar results have been obtained by others.48 Additionally, the specific staining of blood and lymphatic endothelium significantly contributed to an accurate evaluation of LI occurrence, and to a specific distinction between BVI and LVI (Figs. 1C and 1D). This was particularly important in the accurate detection of isolated malignant cells invading lymphatic capillaries, which have a higher propensity to survive in the lymphatic flow, when comparing with the rigors of the blood circulation. In fact, malignant emboli – easily detectable in hematoxylin and eosin (H&E) stained sections if no stromal retraction is observed – are more prone to invade the chaotic and hyperpermeable structure of the blood vasculature and to overcome the hostilities inherent to blood flow, such as serum toxicity, high shear stress and mechanical deformation.49 Conversely, lymph flows slowly, and has a composition similar to interstitial fluid, being ideal for the survival and dissemination of single malignant cells.50 These are more difficult to detect in H&E sections. Thus, the specific staining of lymphatic endothelium contributes to accurately diagnose LVI occurrence (Fig. 1D), which significantly impairs overall survival, as well as BVI by malignant emboli (Fig. 1C). BVI was identified as an independent prognostic factor in our cohort. In another study where we developed a model of bladder cancer aggressiveness by the combined analysis of clinicopathological – stage and grade – and biological – specifically highlighted BVI and LVI, and CD147 expression – parameters51 (Table 1), we found that BVI and LVI clearly contributed to separate between low and high aggressiveness groups. BVI and LVI occurrence may, therefore, represent potential prognostic biomarkers that can guide personalized selection of patients likely to benefit from perioperative chemotherapy regimens and/or targeted therapies. In accordance, a recent review has emphasized that LI should be routinely reported in the pathological report, and that immunohistochemistry identification of blood and lymphatic vessels should be employed in histologically equivocal cases for confirmation.43
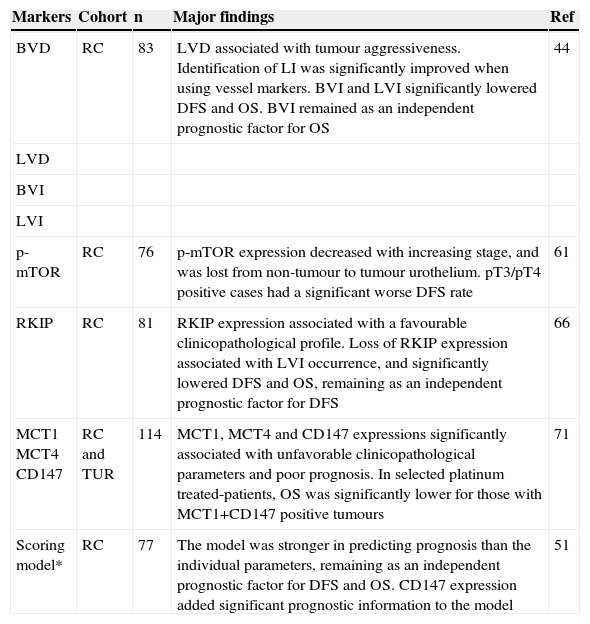
Selected studies on urothelial bladder cancer biomarkers.
| Markers | Cohort | n | Major findings | Ref |
|---|---|---|---|---|
| BVD | RC | 83 | LVD associated with tumour aggressiveness. Identification of LI was significantly improved when using vessel markers. BVI and LVI significantly lowered DFS and OS. BVI remained as an independent prognostic factor for OS | 44 |
| LVD | ||||
| BVI | ||||
| LVI | ||||
| p-mTOR | RC | 76 | p-mTOR expression decreased with increasing stage, and was lost from non-tumour to tumour urothelium. pT3/pT4 positive cases had a significant worse DFS rate | 61 |
| RKIP | RC | 81 | RKIP expression associated with a favourable clinicopathological profile. Loss of RKIP expression associated with LVI occurrence, and significantly lowered DFS and OS, remaining as an independent prognostic factor for DFS | 66 |
| MCT1 MCT4 CD147 | RC and TUR | 114 | MCT1, MCT4 and CD147 expressions significantly associated with unfavorable clinicopathological parameters and poor prognosis. In selected platinum treated-patients, OS was significantly lower for those with MCT1+CD147 positive tumours | 71 |
| Scoring model* | RC | 77 | The model was stronger in predicting prognosis than the individual parameters, remaining as an independent prognostic factor for DFS and OS. CD147 expression added significant prognostic information to the model | 51 |
BVD: blood vessel density; BVI: blood vessel invasion; DFS: disease-free survival; LVD: lymphatic vessel density; LVI: lymphatic vessel invasion; LI: lymphovascular invasion; MCT: monocarboxylate transporter; OS: overall survival; p-mTOR: phospho-mammalian target of rapamycin; RC: radical cystectomy; RKIP: Raf kinase inhibitor protein; TUR: transurethral resection.
* Scoring model: includes clinicopathological parameters – stage and grade – combined with three biological parameters – BVI, LVI and CD147 overexpression.
, and intratumoral lymphatic vessels highlighted by D2-40 (B and D, ×400 amplification), in invasive urothelial carcinoma. Evidence of internal negative control in B (* D2-40 negative blood vessel). A small malignant embolus and an isolated malignant cell are invading intratumoral blood (C) and lymphatic (D) vessels (adapted from Afonso et al.44).")
CD31 and D2-40 immunoexpressions in urothelial bladder carcinoma. Intratumoral blood vessels highlighted by CD31 (A, ×100 amplification, and C, ×400 amplification), and intratumoral lymphatic vessels highlighted by D2-40 (B and D, ×400 amplification), in invasive urothelial carcinoma. Evidence of internal negative control in B (* D2-40 negative blood vessel). A small malignant embolus and an isolated malignant cell are invading intratumoral blood (C) and lymphatic (D) vessels (adapted from Afonso et al.44).
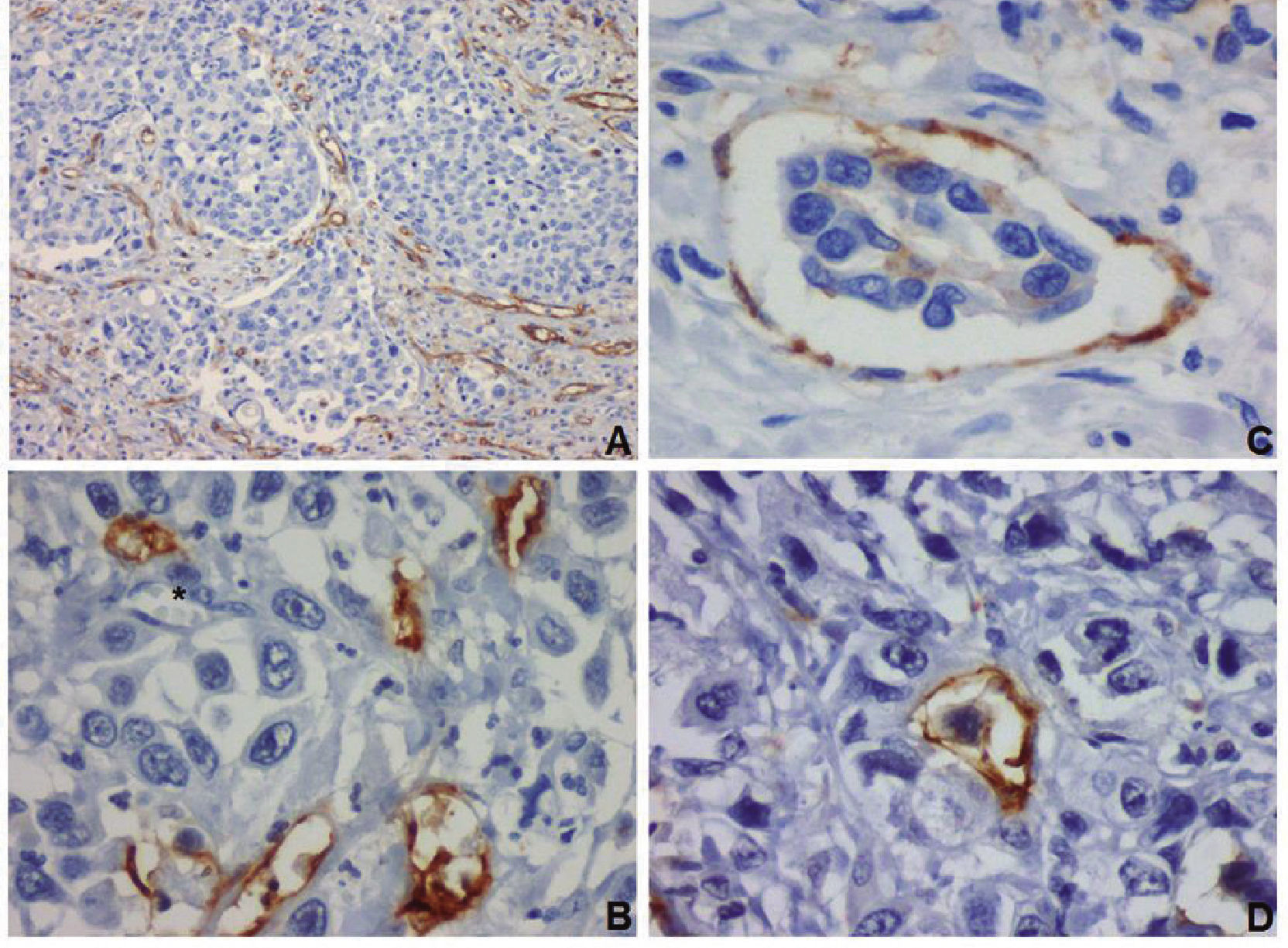
Angiogenesis and lymphangiogenesis represent potential targets for therapeutic intervention in the UBC setting, and several compounds targeting the most relevant neovascularization signalling pathways are being tested in clinical trials.52 However, caution is recommended, due to the risk of refractoriness to VEGFs/VEGFRs signalling blockade.53 In fact, compensation mechanisms to VEGF abrogation in UBC cells lines have been described.54 In alternative, the mammalian target of rapamycin (mTOR) intracellular pathway, besides transducing signals that activate the translational machinery and promote cell growth,55 is also an important signalling mediator in hypoxia-induced angiogenesis.56 Some rapamycin analogues have demonstrated anti-angiogenic effects in UBC pre-clinical57 and clinical trials.58 Nevertheless, the levels of mTOR activation in UBC tissue sections have been poorly explored, and controversial results were found.59,60 We assessed phospho-mTOR (p-mTOR) levels in a series of 76 UBC sections with representative tumour and non-tumour (normal-like or hyperplasic) areas, where blood and lymphatic vessels were also stained by immunohistochemistry, in order to correlate angiogenesis and lymphangiogenesis occurrence with p-mTOR expression61 (Table 1). No significant associations were found between the clinicopathological parameters and vascular density, and p-mTOR expression. Even though, we observed that p-mTOR decreased with increasing stage, and was lost from non-tumour to tumour urothelium, particularly in MI lesions, where immunoexpression was observed in a few spots of cells. Angiogenesis occurrence was impaired in pT3/pT4 negative tumours; conversely, pT3/pT4 positive cases had worse survival rates, as reported by other authors.59 In NMI tumours, p-mTOR was evenly distributed within the malignant urothelium, although staining was stronger at the superficial layers of cells (Fig. 2A), resembling the pattern of expression that was observed in the non-tumour urothelium, where p-mTOR expression was restricted to umbrella cells and some superficial cells of the intermediate layer (Fig. 2B). This pattern of expression has been similarly described in other studies.59 We hypothesized that umbrella cells from non-tumour urothelium express p-mTOR constitutively, as part of their metabolic plasticity, and that NMI lesions with increasing malignant potential extend immunoexpression to the inner layers. The two patterns among MI tumours – absence of expression or expression in cell clusters – probably indicate divergent biological scenarios encompassing the mTOR pathway. Additional studies with larger and more comprehensive UBC series and panels of mTOR upstream and downstream effectors, together with reproducible immunohistochemical and molecular approaches, and with in vivo and in vitro bladder tumour models, are urgently needed to clarify the backstage of the mTOR pathway in human urothelial bladder cancer, in order to expedite the research on potential target therapeutic approaches.
, with the luminal and intermediate cell layers being more intensely stained than the layer of basal cells. B, normal urothelium (×400 amplification) exhibiting cytoplasmic p-mTOR immunoexpression restricted to the superficial layers (adapted from Afonso et al.61).")
p-mTOR immunoexpression in normal and malignant urothelium. A, non-muscle invasive papillary tumour expressing cytoplasmic p-mTOR in a heterogeneous pattern (×100 amplification), with the luminal and intermediate cell layers being more intensely stained than the layer of basal cells. B, normal urothelium (×400 amplification) exhibiting cytoplasmic p-mTOR immunoexpression restricted to the superficial layers (adapted from Afonso et al.61).
Tumour metastasis, the most fearsome aspect of cancer, is a multistage process during which malignant cells separate from the primary tumour and invade discontiguous organs. Angiogenesis and lymphangiogenesis, as already mentioned, are essential for invasion and metastasis to occur, but numerous additional events are also necessary for the success of the metastatic spread. In fact, a long series of sequential, rate limiting, interrelated steps must occur, involving the physical translocation of a malignant cell to a distant organ, and the ability of that cell to develop into a metastatic lesion at the distant site. The final result depends not only on the intrinsic properties of the tumour cells, but also on the host responses.62
High risk NMI and, more often, MI-UBC, carry a significant threat of invasion and metastasis despite radical surgical treatment.13 Timely detection of biomarkers that enable malignant cells with invasive and metastatic properties would allow identifying patients that could benefit from early aggressive approaches such as radical cystectomy and perioperative chemotherapy, and would guide the development of targeted therapies. Conversely, while inhibiting biomarkers of invasion and metastasis emerges as an attractive therapeutic strategy, restoring the function of metastasis suppressor proteins is not less appealing. In this scenario, the role of the metastasis suppressor RKIP (Raf kinase inhibitor protein) in cancer has been highlighted due to its ability to modulate several intracellular signalling cascades involved in cell differentiation, cell cycle kinetics, apoptosis, epithelial to mesenchymal transition and cell migration.63 Given its pleiotropic abilities in maintaining cellular equilibrium, it is not surprising that RKIP downregulation associates with metastatic events in an increasing number of solid tumours.64 Its preponderance in UBC setting is largely unknown, although low mRNA levels have been reported in NMI tumours, when compared with normal urothelium.65
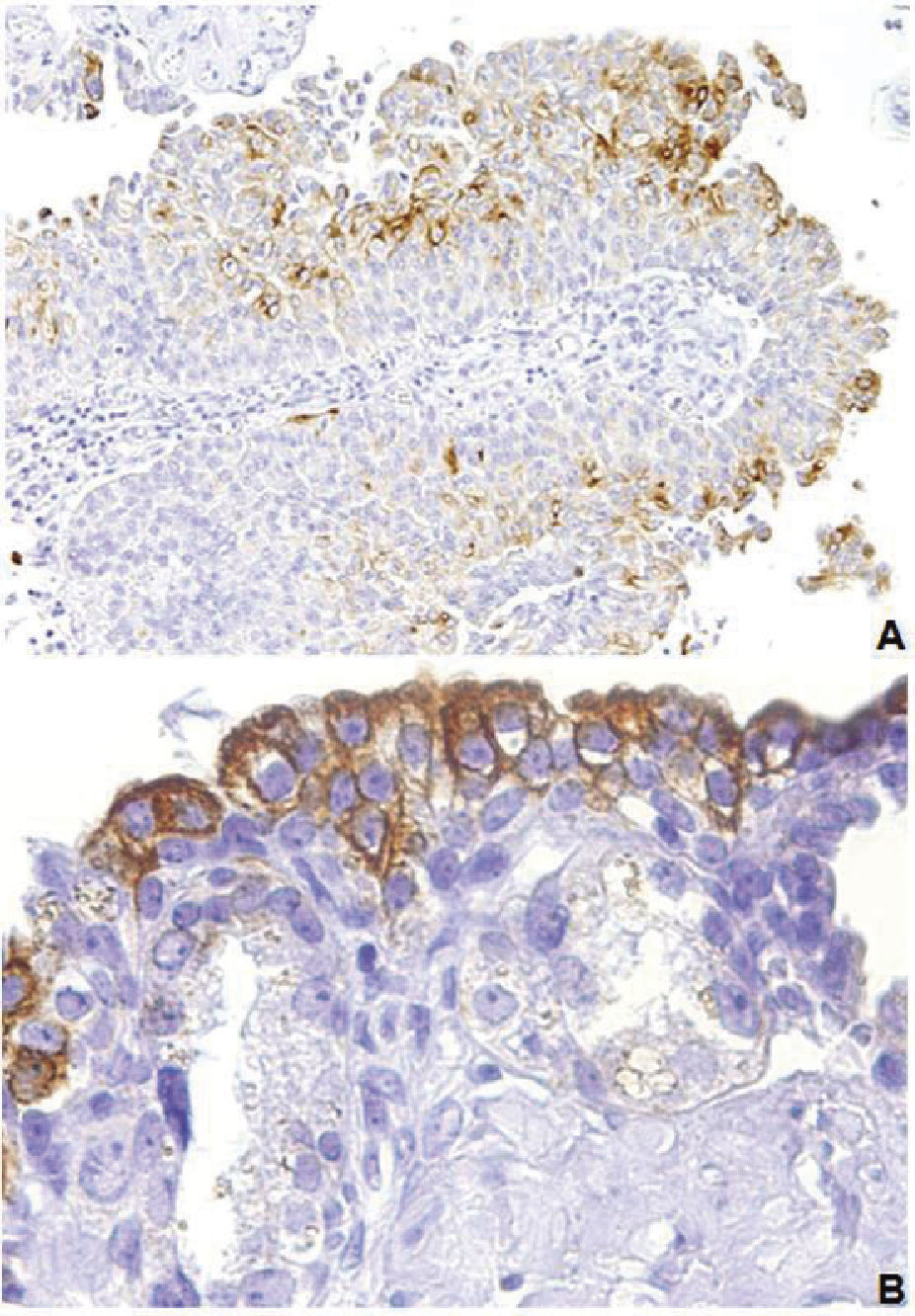
We evaluated RKIP expression in a cohort of 81 tumour sections from UBC patients. Blood and lymphatic vessels were also assessed, in order to correlate BVI and LVI occurrence with RKIP levels66 (Table 1). To the best of our knowledge, this was the first study evaluating RKIP immunoexpression in bladder cancer tissue samples. We observed a homogeneous expression of RKIP in normal urothelium (Fig. 3A) and in tumour sections with a favourable clinicopathological profile, namely NMI tumours where LVI was absent (Fig. 3B). Conversely, a heterogeneous pattern of expression, with loss of RKIP expression intensity from the tumour centre to the invasion front, was associated with LVI occurrence (Fig. 3C). Moreover, low RKIP expression significantly lowered disease-free and overall survival, remaining as an independent prognostic factor for disease-free survival. RKIP loss or diminution had been previously reported in other types of aggressive cancers, significantly impairing prognosis. Clinically, RKIP expression is higher in benign tumors than in malignant tissues while its expression is completely absent in metastases.63 Additional studies in bladder cancer setting need to be urgently developed, in order to confirm our promising results and to expand the research into therapeutic strategies that can potentially restore RKIP functionality. Besides acting as a prognostic biomarker, RKIP status may also have a role as a predictive biomarker, once it has been demonstrated that its expression may potentiate apoptosis induced by chemotherapeutic agents, which might be useful in defining therapy response profiles.67,68
. B, a non-invasive papillary tumour showing a homogeneous pattern of expression (×100 amplification). C, an infiltrating tumour exhibiting a heterogeneous pattern, with the tumour core being more intensely stained than the invasive front (×100 amplification) (adapted from Afonso et al.66).")
RKIP immunoexpression in normal and malignant urothelium. A, immunohistochemical positive reaction for RKIP in normal urothelium (×200 amplification). B, a non-invasive papillary tumour showing a homogeneous pattern of expression (×100 amplification). C, an infiltrating tumour exhibiting a heterogeneous pattern, with the tumour core being more intensely stained than the invasive front (×100 amplification) (adapted from Afonso et al.66).
Altered energy metabolism, although only recently emerged as a new hallmark of cancer,2 is proving to be as widespread in tumour cells as the classical traits of malignancy. In fact, cancer growth is characterized by deregulated cell proliferation and corresponding adjustments of energy metabolism, such as the adoption of the Warburg effect. This necessarily involves different inputs to the tumour microenvironment, namely the extrusion of high amounts of lactate from the malignant cells that will sculpt an acid-resistant phenotype, which supports increased migration and invasion, favouring metastasis.69,70 Molecules and pathways involved in this intricate backstage of malignancy potentially represent new areas of therapeutic intervention.
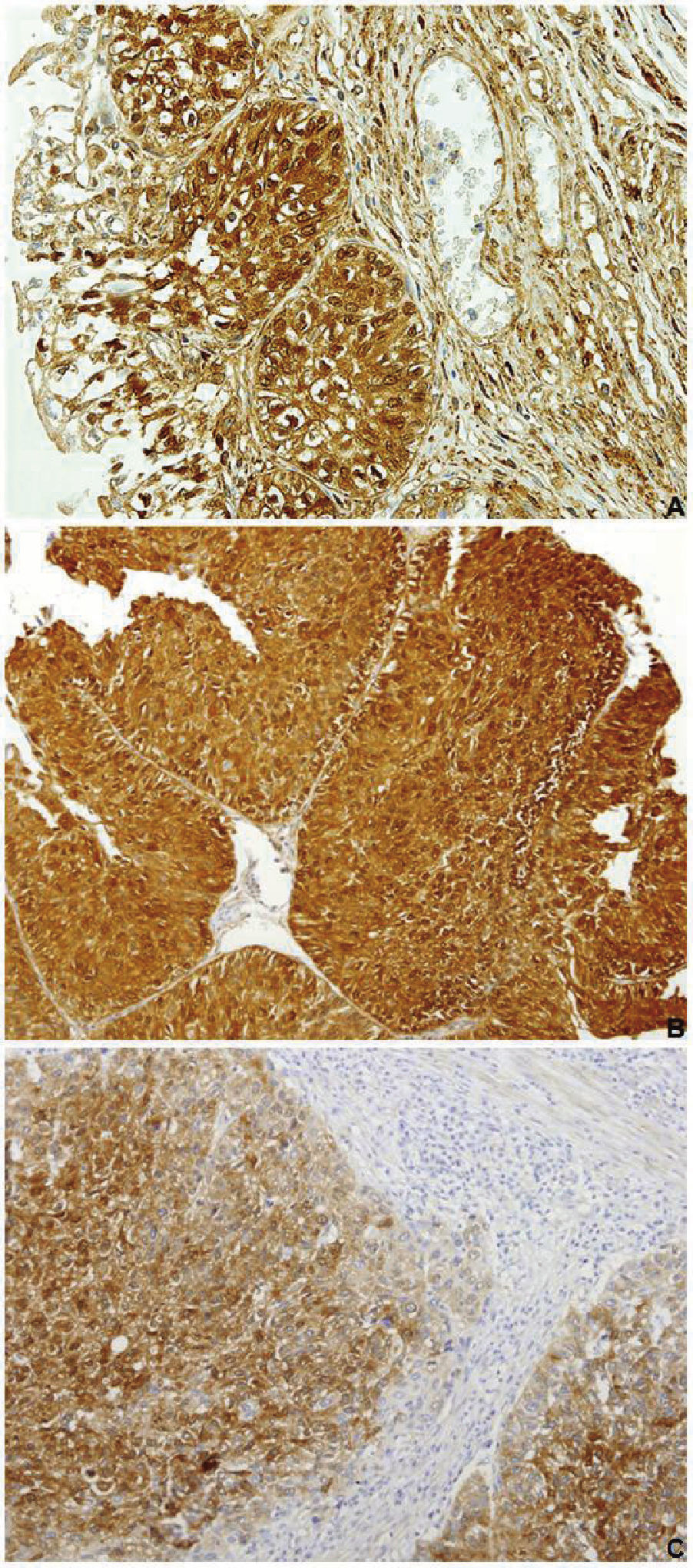
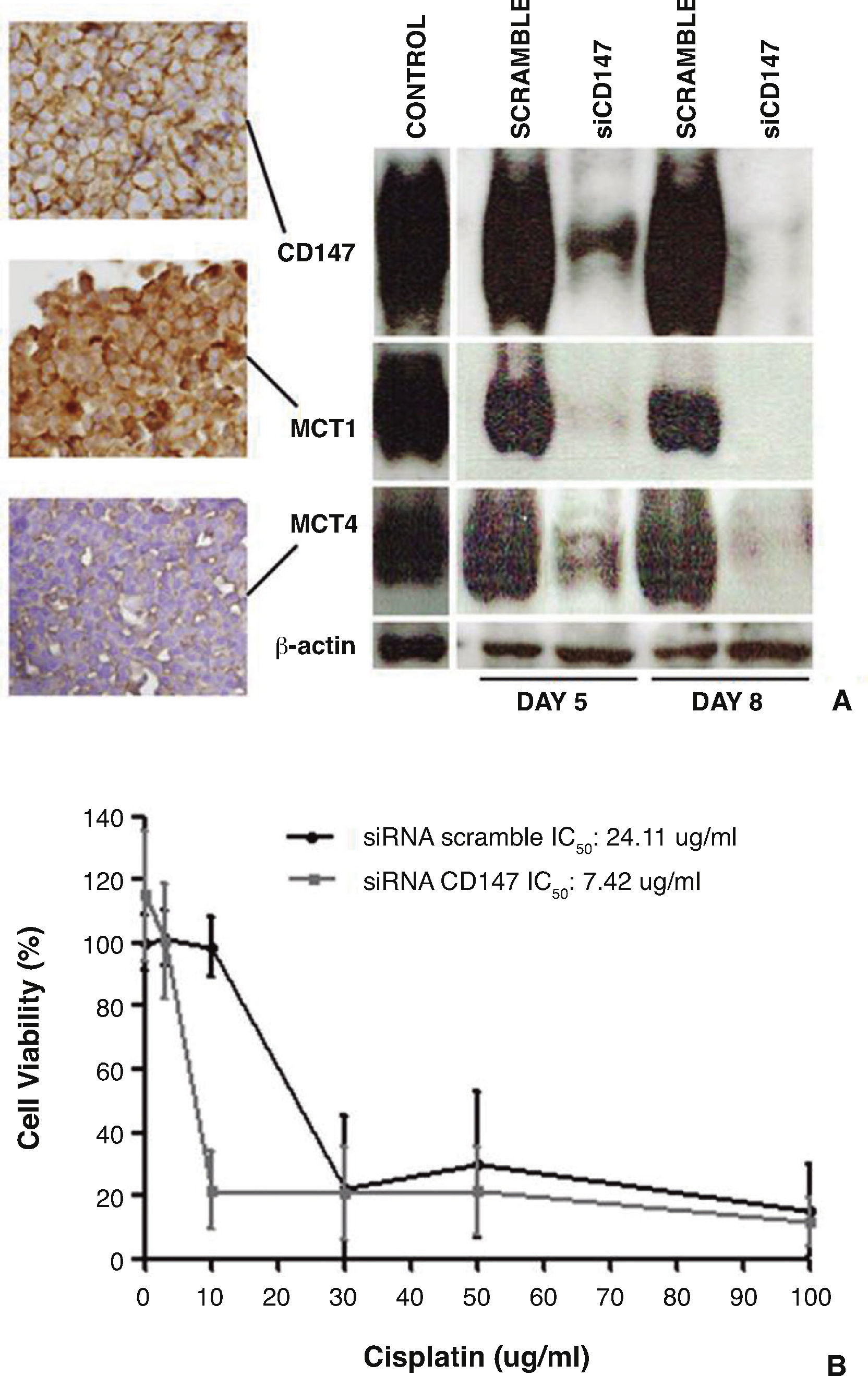
The biological mechanisms that reprogram cellular energetics and model the tumour microenvironment are poorly characterized in bladder cancer. Thus, we elected a panel of three microenvironment-related molecules and investigated their expressions in a subset of tumour tissue sections from 114 UBC patients treated by transurethral resection and/or radical cystectomy71 (Table 1). The central player was CD147, a tumor cell surface molecule implicated in extracellular matrix remodeling, angiogenesis and tumour growth, and related with chemoresistance-promoting events.72 We had previously demonstrated the prognostic impact of CD147 overexpression in bladder cancer patients, when we developed a model of UBC aggressiveness that included clinicopathological and biological parameters51 (Table 1). In fact, CD147 expression was largely preponderant in the high aggressiveness group, and clearly added prognostic information to the model. For that reason, we decided to re-evaluate this glycoprotein in a larger series, together with other molecular companions. Thus, we observed that CD147 was upregulated in bladder tumour tissue (Fig. 4A), significantly associating with a dismal clinicopathological profile and poor prognosis. Other authors have identified CD147 expression in UBC as an independent prognostic biomarker,73,74 and have additionally proposed it as a predictive biomarker in the setting of cisplatin-containing regimens.74 To confirm this hypothesis, we established four CD147-expressing UBC cell lines and studied the effect of cisplatin treatment on cell viability, cell cycle distribution and cell death, as well as on the migration and invasion abilities of the cells. CD147 expression was then downregulated in a cisplatin less-sensitive cell line (Fig. 5A). Importantly, we found that CD147 downregulation clearly increased chemosensitivity to cisplatin (Fig. 5B). To the best of our knowledge, this was the first in vitro study demonstrating that CD147 depletion in UBC cells enhances the therapeutic action of cisplatin, highlighting this molecule as a potential prognostic and predictive biomarker.
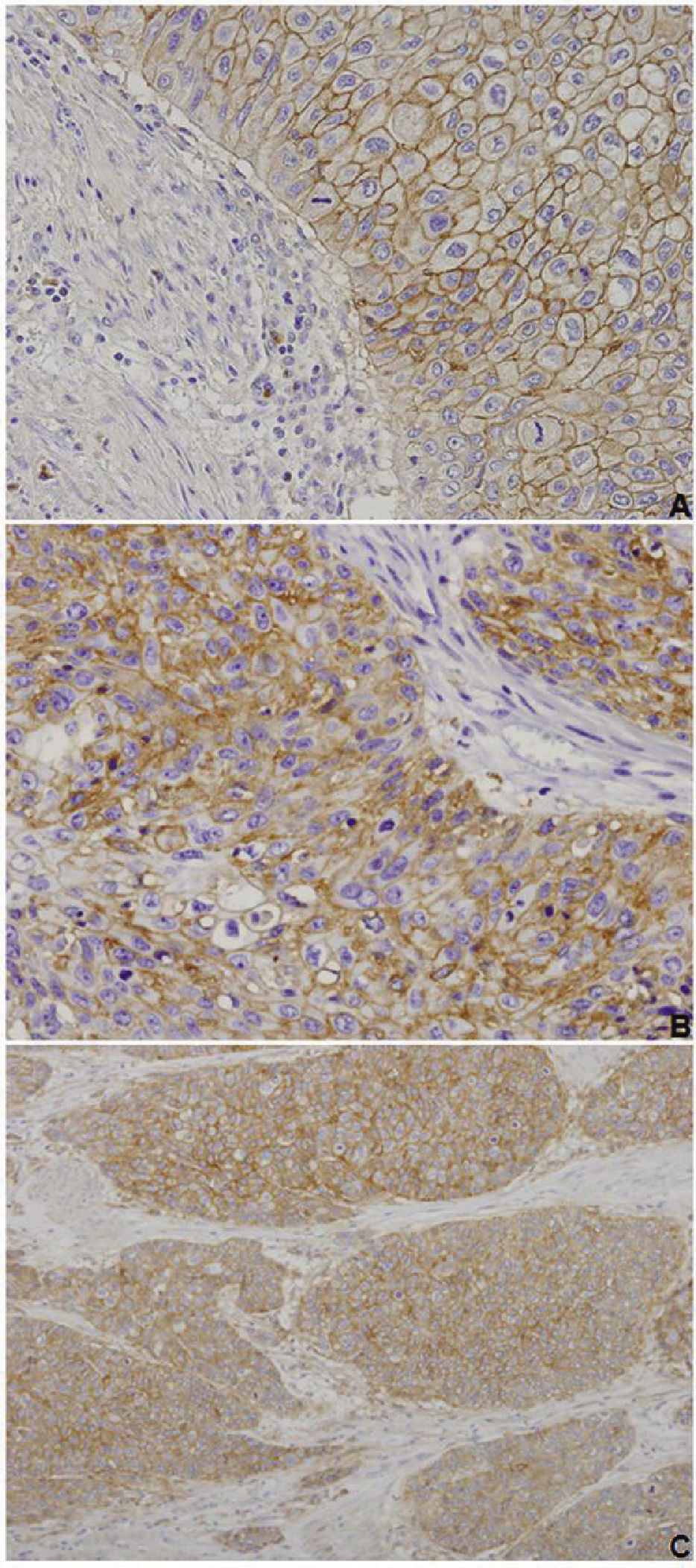
, MCT1 (B, ×200 amplification) and MCT4 (C, ×100 amplification) in the malignant urothelium, with negative stromas (adapted from Afonso et al.71).")
CD147, MCT1 and MCT4 immunoexpressions in urothelial bladder carcinoma. Muscle-invasive tumours exhibiting cytoplasmic and membrane immunoexpression of CD147 (A, ×200 amplification), MCT1 (B, ×200 amplification) and MCT4 (C, ×100 amplification) in the malignant urothelium, with negative stromas (adapted from Afonso et al.71).
. A, CD147, MCT1 and MCT4 immunoexpressions in HT1376 control cells, and Western blot analysis of CD147, MCT1 and MCT4 expressions in control/scramble HT1376 cells and in siCD147 HT1376 cells, showing that CD147 silencing was accompanied by a decrease in MCT1 and MCT4 expressions. B, effect of cisplatin on the viability of scramble and siCD147HT1376 cells, as detected by the MTS assay after 72 hours of treatment, showing that siCD147 cells were more sensitive to cisplatin (adapted from Afonso et al.71).")
Effect of CD147 downregulation in HT1375 cell line on the expression of MCTs and on chemosensitivity to cisplatin (treatment with cisplatin between days 5 and 8 after reverse transfection). A, CD147, MCT1 and MCT4 immunoexpressions in HT1376 control cells, and Western blot analysis of CD147, MCT1 and MCT4 expressions in control/scramble HT1376 cells and in siCD147 HT1376 cells, showing that CD147 silencing was accompanied by a decrease in MCT1 and MCT4 expressions. B, effect of cisplatin on the viability of scramble and siCD147HT1376 cells, as detected by the MTS assay after 72 hours of treatment, showing that siCD147 cells were more sensitive to cisplatin (adapted from Afonso et al.71).
In order to further elucidate CD147 interactions, we also analyzed monocarboxylate transporter (MCT) expressions in the cohort of 114 UBC patients71 (Table 1). MCTs, particularly MCT1 and MCT4, play a key role in the promotion of the hyper-glycolytic acid-resistant phenotype, by exporting lactate from the glycolytic malignant cells to the tumour microenvironment.75 CD147 has been described as a chaperone for the proper expression of MCTs at the plasma membrane,76 and our results support that function. In fact, we found significant associations among MCT1, MCT4 and CD147 expressions. MCT1 and MCT4 were upregulated in highly aggressive tumours (Fig. 4B and 4C), and MCT1 overexpression impaired overall survival. In accordance, a recent study demonstrated the independent prognostic significance of MCT1 and MCT4 in UBC77; their upregulation has also been observed in other malignancies.78 Interestingly, a CD147 and MCT1 double-positive profile was significantly associated with unfavourable clinicopathological parameters and poor prognosis in our UBC series, and discriminated a poor prognosis group in cisplatin-treated patients. We hypothesized that MCT1 cooperates with CD147 in the promotion of a chemoresistance phenotype and, possibly, of other functions that are primarily attributed to CD147. In fact, it appears that CD147 maturation is affected by MCT expression.79 In our in vitro study, CD147 depletion was accompanied by a marked decrease in the expression of MCT1 and MCT4 (Fig. 5A), which suggests CD147 as an MCT1/4 chaperone. It would be interesting to silence MCT1 expression in the UBC cell line and to study CD147 expression levels, in order to confirm the opposite.
Overall, our results point out for an important role of CD147 and their companions in promoting a highly aggressive phenotype where glycolysis is upregulated, contributing to acidify the tumour microenvironment, enabling the malignant cells with growth, migration, invasion and chemoresistance abilities that can only be overcome if new approaches of target therapeutic intervention are investigated.
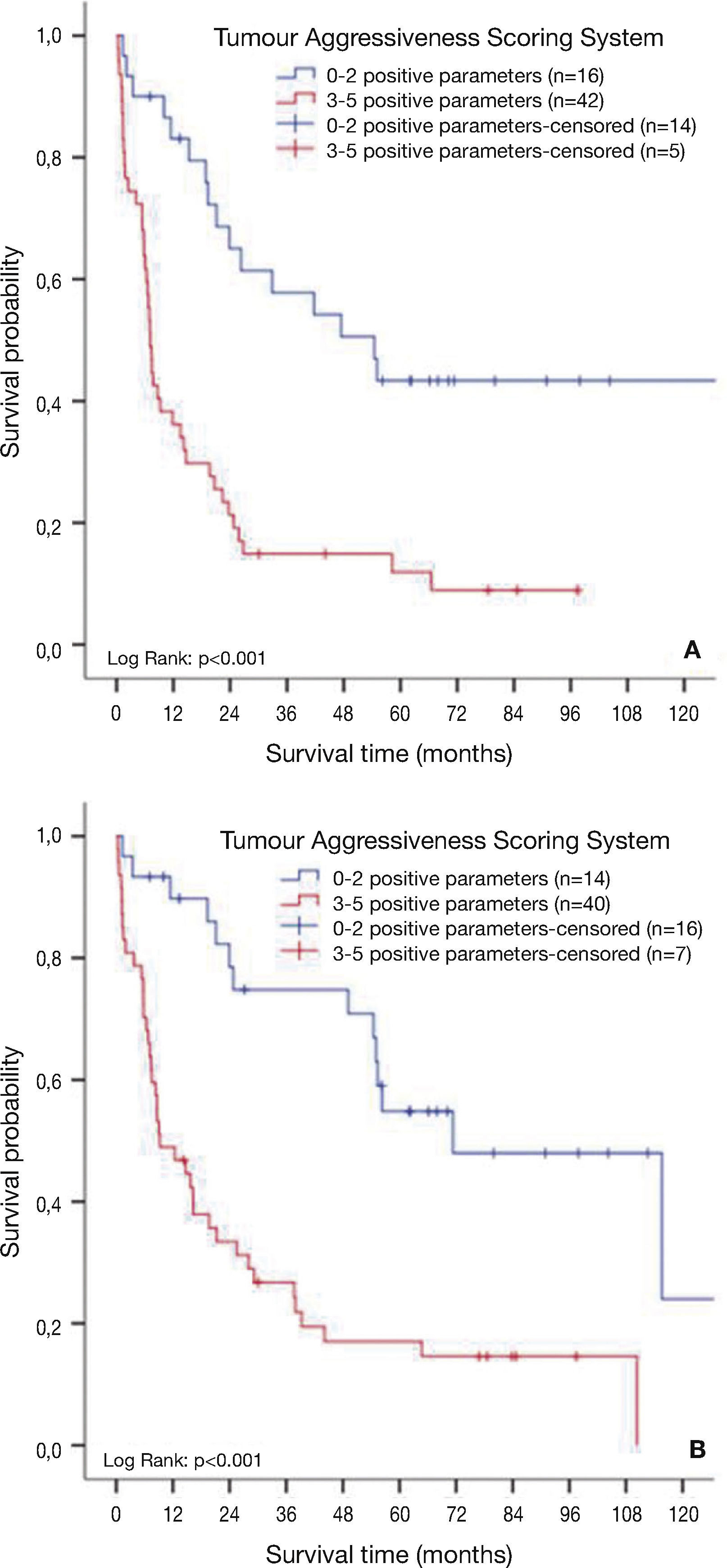
The utility of combining distinct biomarkers – practical implicationsCurrently, there is no doubt that inclusion of prognostic and predictive biomarkers into the classical instruments of diagnosing the disease and predicting outcomes, such as risk stratification tables,80,81 nomograms82,83 and artificial neural networks,84,85 would certainly refine diagnosis, prognosis and therapeutic decision, with several studies demonstrating the potential impact of developing risk stratification tools that integrate clinicopathological and biological parameters.51,86,87 Moreover, it seems that combining biomarkers inherent to different cancer hallmarks improves predictive accuracy over one biomarker abnormality, as several biomarkers may help to elucidate individual biological features of the tumours.12,20,51,88-90 As it was previously mentioned, we developed a model of tumour aggressiveness by the combined analysis of two clinicopathological parameters – stage and grade – with three biological parameters – BVI, LVI and CD147 overexpression51 (Table 1). Therefore, we included biomarkers that are mainly associated with angiogenesis (BVI), lymphangiogenesis (LVI), energy metabolism reprogramming, invasion and chemoresistance (CD147). The parameters included in the model had individual prognostic impact on the 77 UBC patients that were studied, as demonstrated in univariate analysis. However, the model was stronger in predicting prognosis, clearly separating a low aggressiveness from a high aggressiveness group, and remaining as an independent prognostic factor for disease-free (Fig. 6A) and overall survival (Fig. 6B). If an additional biomarker was included in the model, namely immunoexpression of the metastasis suppressor RKIP, its accuracy would be further enhanced (data not shown). Therefore, combining distinct biomarkers with the classical clinicopathological parameters will have undeniable impact for UBC patients, who may benefit, in the future, from accurate prediction of outcomes and response to therapy, and guided targeted therapy.
 and 5-year overall survival (B) based on a tumour aggressiveness scoring system that includes T3/T4 pathologic stage, grade III, occurrence of blood vessel invasion by malignant emboli, occurrence of lymphatic vessel invasion by isolated malignant cells and CD147 overexpression (n=77) (adapted from Afonso et al.51).")
Survival analysis of urothelial bladder cancer patients based on a tumour aggressiveness scoring system. 5-year disease-free survival (A) and 5-year overall survival (B) based on a tumour aggressiveness scoring system that includes T3/T4 pathologic stage, grade III, occurrence of blood vessel invasion by malignant emboli, occurrence of lymphatic vessel invasion by isolated malignant cells and CD147 overexpression (n=77) (adapted from Afonso et al.51).
Bladder cancer, being the second most common malignancy of the urogenital region, represents a significant epidemiological problem, mostly due to its heterogeneous natural history and clinical behavior. Validated biomarkers would certainly help to elucidate unique biological features that may allow identifying patients who are at increased risk of recurrence, progression, metastasis and/or chemorefractory relapse. In addition, biomarkers may improve prediction of response to therapy and guide us to a new era of tailored and targeted treatment. Current research efforts are directed into the elaboration of nomograms that can combine well-established clinicopathological parameters with novel putative biomarkers. In this line of investigation, we suggest that lymphovascular invasion occurrence, and RKIP, CD147 and MCT1 expressions might be relevant prognostic and/or predictive biomarkers, and promising areas of therapeutic intervention, eliciting for the development of additional studies that can validate and further explore the potentialities of our work. We additionally stand up for the specific staining of blood and lymphatic endothelium by immunohistochemistry in histologically equivocal cases that require confirmation, in order to identify images of lymphovascular invasion that could be missed during the classical evaluation on H&E stained tumour sections, and to allow an accurate discrimination between the two forms of lymphovascular invasion. There is the urgent need to transpose these and other biomarker tests on small groups of patients to large-scale independent validation assays, encompassing multi-institutional collaborations, so that prospective validations and randomized trials based on the retrospective findings may then proceed.
Ethical disclosuresProtection of human and animal subjects. The authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of data. The authors declare that no patient data appear in this article.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
