





Evaluar la relación entre el cáncer de próstata (CaP) y la presencia de síndrome metabólico (SM) y síndrome de hipogonadismo tardío (SHT).
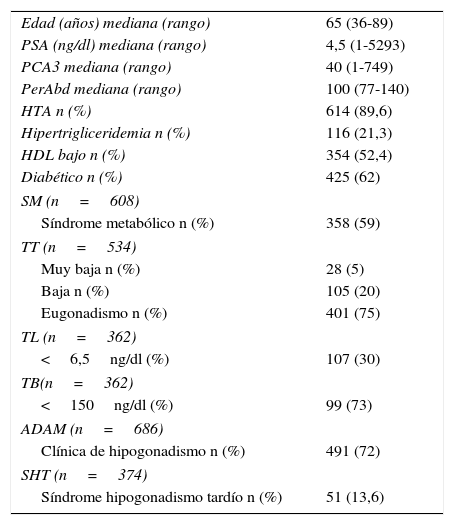
Material y métodoEstudio retrospectivo de 686 pacientes sometidos a biopsia prostática. Analizamos: variables demográficas, datos clínicos y resultados de la biopsia. Para diagnosticar el SM se utilizaron los criterios de la American Heart Association. Para el diagnóstico de SHT se utilizó el cuestionario ADAM y los niveles de testosterona (TT). Evaluamos la relación de la testosterona libre (TL) y testosterona biodisponible (TB) con el CaP y su agresividad y la utilidad de la ratio TT/PSA en el diagnóstico de CaP.
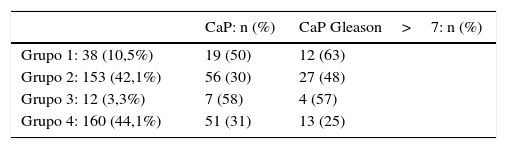
ResultadosMediana de edad 65 años. El SM no se asoció al CaP (39,4% vs 35% p=0,1) pero sí a un CaP Gleason>7 (50,4% vs 29,44% p=0,002). El SHT, TL baja y TB baja se asociaron a una mayor presencia de CaP (51% vs 35% p=0,02; 44,86% vs 33,33%, p=0,03; 46,46% vs 33,08%, p=0,01 respectivamente) y a mayor probabilidad de CaP Gleason >7 (61,54% vs 37,5% p=0,02; 54,17% vs 34,12%, p=0,02; 54,35% vs 34,48% p=0,02 respectivamente). Además, la mediana de la ratio de TT/PSA fue significativamente menor en los pacientes con BxP positiva (p=0.022).
Conclusionesel SM no se asoció con la probabilidad de tener CaP, pero sí con el CaP Gleason>7. Por otro lado, el SHT presentó un mayor porcentaje de CaP y una mayor presencia de CaP Gleason>7, al igual que los niveles bajos de TL y los niveles bajos de TB.
To assess the relationship between prostate cancer (PC) and the presence of metabolic syndrome and late-onset hypogonadism (LOH) syndrome.
Material and methodA retrospective study was conducted on 686 patients who underwent prostate biopsy. We analysed the demographic variables, clinical data and biopsy results. To diagnose metabolic syndrome, we employed the criteria of the American Heart Association. For the diagnosis of LOH syndrome, we employed the Androgen Deficiency in the Aging Male questionnaire and testosterone levels (TT). We evaluated the relationship between free testosterone (FT) and bioavailable testosterone (BT) on one hand and PC and its aggressiveness on the other, as well as the usefulness of the TT to prostate specific antigen (TT/PSA) ratio in the PC diagnosis.
ResultsThe patient's median age was 65 years. Metabolic syndrome is not associated with PC (39.4% vs. 35%; P=.1) but is associated with a PC Gleason score >7 (50.4% vs. 29.44%; P=.002). LOH, low FT and low BT are associated with an increased presence of PC (51% vs. 35%, P=.02; 44.86% vs. 33.33%, P=.03; and 46.46% vs. 33.08%, P=.01, respectively) and with an increased probability of a PC Gleason score >7 (61.54% vs. 37.5%, P=.02; 54.17% vs. 34.12%, P=.02; 54.35% vs. 34.48%, P=.02, respectively). Additionally, the median TT/PSA ratio was significantly lower in patients with positive biopsies (P=.022).
ConclusionsMetabolic syndrome was not associated with the probability of having PC but was associated with a PC Gleason score >7. Moreover, LOH syndrome had a higher percentage of PC and a greater presence of PC Gleason scores >7, as did low levels of FT and low levels of BT.
Artículo

Comprando el artículo el PDF del mismo podrá ser descargado
Precio 19,34 €
Comprar ahora


